Article Text

Abstract
Objective: To evaluate biomechanical properties of skin in patients with systemic sclerosis (SSc) using the BTC-2000 suction device.
Methods: Twenty five patients with limited cutaneous SSc (lcSSc), 20 patients with diffuse disease (dcSSc), and 25 age matched healthy controls were evaluated. Viscoelastic deformation (VED, mm), elastic deformation (ED, mm), ultimate deformation (UD, mm), and pressure-deformation ratio (PDR, mm Hg/mm) were measured on the dorsal surface of the forearm, shoulder, and above the trapezius muscle on the back.
Results: Indices of skin extensibility (VED, ED, UD) were reduced and resistance to stress (PDR) increased in patients with dcSSc compared with healthy controls, or patients with lcSSc, at all three sites (p<0.001). At all sites, and overall, UD, ED, and VED were lower and PDR was higher at skin score above grade 2, compared with clinically normal skin. For both lcSSc and dcSSc biomechanical differences from controls were found even at sites of clinically normal skin.
Conclusion: BTC-2000 is a sensitive tool for clinical evaluation of skin involvement in SSc and may be a valuable adjunct to skin sclerosis score in disease monitoring.
- scleroderma
- biomechanical properties
- systemic sclerosis
- dcSSc, diffuse cutaneous systemic sclerosis
- ED, elastic deformation
- lcSSc, limited cutaneous systemic sclerosis
- PDR, pressure-deformation ratio
- SSc, systemic sclerosis
- UD, ultimate deformation
- VED, viscoelastic deformation
Statistics from Altmetric.com
- dcSSc, diffuse cutaneous systemic sclerosis
- ED, elastic deformation
- lcSSc, limited cutaneous systemic sclerosis
- PDR, pressure-deformation ratio
- SSc, systemic sclerosis
- UD, ultimate deformation
- VED, viscoelastic deformation
Scleroderma (SSc) is an autoimmune rheumatic disease characterised by obliterative microvascular lesions and development of fibrosis in skin and internal organs. Skin involvement is a hallmark of the condition and SSc is subdivided into two major subsets according to the extent and distribution of skin sclerosis: diffuse cutaneous (dcSSc) and limited cutaneous (lcSSc) systemic sclerosis.1 The latter is characterised by skin changes restricted to the face, neck, and distal extremities (hands, forearms, feet) and occurs in around 60% of all patients with SSc. In contrast, dcSSc skin involvement extends proximally on the limbs, chest wall, abdomen, and buttocks. Patients with limited and diffuse disease exhibit different autoantibody patterns, which are associated with particular patterns of internal organ complication.2 Studies have shown that the extent, distribution, and rate of progression of skin involvement in dcSSc correlate with internal organ involvement and general outcome of patients with SSc.3,4 A modified Rodnan skin score, based on the ability to “pinch” skin into a fold, is widely used for assessment of skin involvement in SSc, and has been the primary end point used to assess efficacy in several recent controlled trials.5,6
Oedema and inflammatory cell infiltration, particularly around blood vessels in the dermis, are the main pathological processes in early stage scleroderma. Progression of the skin lesions is associated with microvascular obliteration, extensive collagen accumulation and, finally, fibrosis. Eventually, some regression may occur as patients enter a plateau phase of their disease, typically three to five years from onset.
Progression of skin sclerosis disturbs normal skin architecture and compromises biomechanical skin properties.7 Biomechanical assessment of normal skin has shown that the skin has the unique ability to deform under low pressures (extensibility). When the load is increased further, skin shows resistance to stress (stiffness—Young's modulus) but continues to stretch even under stable pressure (viscoelasticity). Skin has a strong tendency to resume its original shape and dimensions after release of the stretching force (elasticity). In vivo studies have shown changes in extensibility, stiffness, and elasticity in different sexes and ages, which in part may be attributed to differences in skin thickness.8–,13 Clinical conditions affecting the fibre framework of skin are likely to alter its biomechanical properties.7,14–,17 In this study we have evaluated the use of a newly developed suction device (BTC-2000, SRLI Technology, Nashville, USA) to assess the biomechanical properties of skin in patients with SSc in comparison with those of healthy controls.
PATIENTS AND METHODS
Patients
Twenty five patients with lcSSc (21 women), aged 25–76 years (mean (SD) 59.4 (9.2)), disease duration 3–26 years (11.5 (7.7)); 20 patients with dcSSc (15 women), aged 21–71 years (48.8 (11.0)), disease duration 1–15 years (4.6 (3.2)) followed up at the Centre for Rheumatology of the Royal Free Hospital of London; and 25 healthy control subjects, matched for age and sex, were enrolled in the study. Patients with SSc were classified according to the American Rheumatism Association (now ACR) preliminary criteria for the classification of systemic sclerosis.1 All patients gave their informed consent before entering the study. At entry all patients with SSc underwent clinical and serological assessment. A modified Rodnan skin score was used to assess total skin involvement and local changes in three areas: dorsal surface of the forearm, dorsal surface of the shoulder, and above the trapezius muscle on the back.
Biomechanical skin properties assessment
The skin biomechanical measurements were carried out on the patients in sitting position after 15 minutes of acclimatisation at a temperature of 22±1°C. The measurement of skin properties was performed on the dorsal forearm surface at the midpoint of a line between the right lateral epicondyle and the right radial styloid process, on the back at the midpoint of a line joining the seventh cervical spinous process to the right acromial process, and the shoulder at the midpoint of a line between the right olecranon and the right acromial process, using the biomechanical tissue characterisation device BTC-2000 (Surgical Research Laboratory, Nashville, USA). This device uses a laser beam to determine accurately the height of a dome induced by applying a multiaxial load of subatmospheric pressure (50 mm Hg) through a 10 mm chamber aperture. Time synchronised pressure and deformation data were displayed and analysed in real-time, and stored to hard disk. The device was connected through BTC-Term interface with a desktop personal computer; and after transferring data from skin measurements, the information was further analysed and stored using Microsoft Excel software. Figure 1⇓ shows a schematic representation of the BTC-2000.

Schematic representation of the BTC-2000 suction device. Simple schematic representation of the suction chamber, laser for measuring the skin dome height, and the arrangement of computerised analysis hardware for the BTC-2000.
The vacuum chamber was placed on the skin surface while using a double sided adhesive disc. The subatmospheric pressure was raised at the rate of 10 mm Hg/s; after it achieved 50 mm Hg it was kept unchanged for three seconds and then interrupted for a three seconds' relaxation period. Elastic deformation (ED, mm), viscoelastic deformation (VED, mm), ultimate deformation (UD, mm), and pressure-deformation ratio (PDR, mm Hg/mm) were recorded. Measurements were performed over five consecutive cycles to derive a mean value for each biomechanical variable.
Data analysis
For normally distributed data, analysis of variance was used for comparison of variables from different sampling sites or study cohorts. Once statistically significant differences were confirmed, these were further analysed by simple statistics. Non-parametric data were analysed by Wilcoxon Mann-Whitney testing. p Values <0.05 were considered significant.
RESULTS
Table 1⇓ summarises the demographic data for healthy controls, and clinical features of patients with SSc. There were no significant differences between healthy controls and patients with dcSSc in age and sex ratio. As predicted by the natural history of the two subsets, patients with limited disease had longer disease duration than patients with dcSSc, and the mean age of patients with lcSSc was greater than that of the dcSSc or control groups. Patients with dcSSc had significantly higher total skin score as well as a local skin score on forearm, shoulder, and back. As expected, patients with limited disease had no clinically apparent skin changes on forearm, shoulder, and back. Both patient groups had similar rates of gastrointestinal, kidney, and heart disease. Patients with limited disease had a higher prevalence of pulmonary hypertension than patients with diffuse disease, whereas lung fibrosis occurred significantly more often in patients with diffuse disease. Fifty per cent of patients with lcSSc had positive anticentromere antibodies and half of the patients with dcSSc had antitopoisomerase-1 antibodies (anti Scl-70).
Demographic data of healthy controls and clinical features of patients with SSc
The raw data for measures of deformation (ED, VED, UD) were normally distributed, but the distribution of values for PDR was somewhat skewed (mean 142.9, median 120.1) and so an additional non-parametric analysis (Wilcoxon Mann-Whitney test) was applied for this variable. Patients with lcSSc showed significantly reduced extensibility (ED, UD) and raised resistance to stress (PDR) of forearm skin (p<0.05) and even more of shoulder skin (p<0.005) compared with healthy controls (table 2⇓). There were no differences in biomechanical features in skin on the back between healthy controls and patients with lcSSc. In contrast, significantly reduced indices of extensibility and increased resistance to mechanical stress (p<0.005) were found in all areas tested for patients with dcSSc compared with healthy controls. Viscoelasticity measured on the forearm, shoulder, and back was significantly reduced in patients with dcSSc compared with that of healthy controls and patients with lcSSc. Subgroup analysis showed no significant differences between the sexes for the variables assessed in SSc or control groups. No correlation was found between biomechanical data and subjects' age or disease duration.
Biomechanical properties of skin on forearm, shoulder, and back in healthy controls and patients with limited and diffuse SSc
Differences in biomechanical properties were recorded between the two SSc groups (table 3⇓). Extensibility (ED, UD) was significantly reduced and resistance to stress (PDR) was greater in patients with diffuse SSc compared with patients with limited disease on forearm and back. A similar trend was present for shoulder skin but was not statistically significant. Although the back is generally considered to be relatively spared from involvement in dcSSc, we found a significant difference in biomechanical properties at this site compared both with patients with lcSSc and healthy controls. By analogy, patients with limited disease showed significantly reduced indices of skin extensibility at the shoulder and forearm, despite undetectable skin sclerosis clinically. Indices of elasticity were not significantly different between healthy controls and both SSc subsets.
Differences in biomechanical properties of the skin of patients with diffuse and limited SSc (p value)
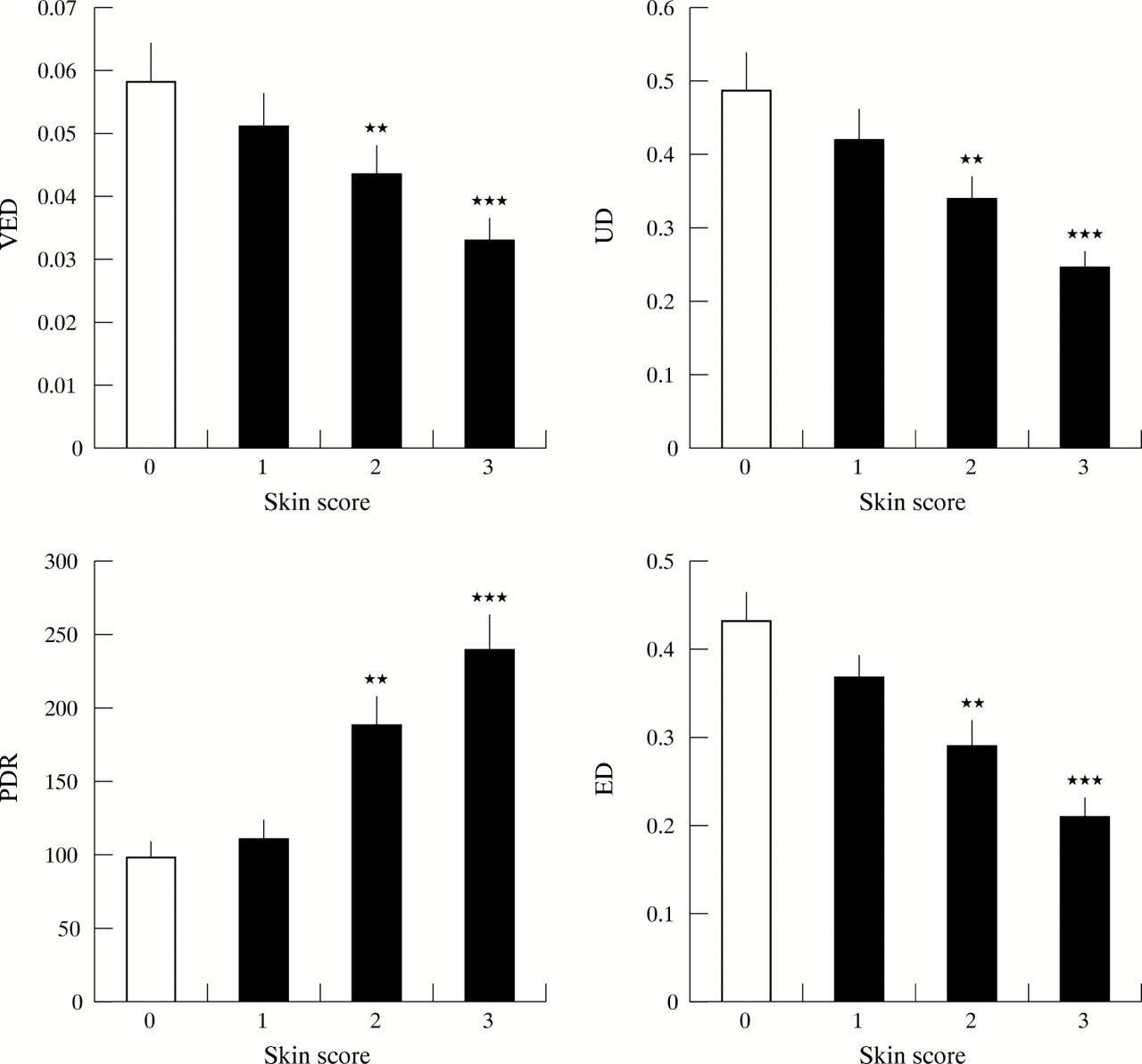
To determine whether biomechanical indices reflect skin properties as assessed by conventional skin scoring, mean values of VED, UD, ED, and PDR were compared for skin areas scored between 0 and 3 in the cohort of patients with dcSSc. Figure 2⇓ summarises the results, confirming that indices of skin deformity are different between normal and sclerotic skin at all sites in these patients. Similar results were obtained for each site analysed individually (data not shown).
{kind=link}
{kind=link}
Relation between sclerosis score and biomechanical properties of skin. For each of the three skin areas assessed (forearm, shoulder, and back) the VED, UD, PDR and ED were compared for areas scored between 0 and 3. Representative histograms summarise data from forearm skin sites scored 0 (n=14), 0 (n=24), 2 (n=15), or 3 (n=8). Indices of skin deformity were lower at higher skin scores, whereas the PDR, reflecting stiffness, was increased. Data show means (SEM) and comparison is by Student's unpaired t test. **p<0.01, ***p<0.001.
DISCUSSION
Skin sclerosis is present in almost all patients with SSc, and is often regarded as a surrogate marker of the severity of the disease. Indeed it has been suggested that changes in skin score are the most reliable index for assessment of potential disease modifying treatments.18 However, several studies have suggested that interobserver and intraobserver variations may confound patient assessment.5,6 Objective methods for assessing skin sclerosis offer greater potential accuracy and sensitivity, together with less variability between measurements. Skin ultrasound examination has been used in several centres, and has proved to be a valuable tool for assessment of skin thickness19,20 as well as providing additional information on density and patterns of echogenicity.21 In contrast, biomechanical properties of skin depend not only upon the thickness of the skin but also on tissue composition, inflammatory changes, and oedema. All of these properties are likely to be altered in SSc and related conditions and our study used the BTC-2000 to compare biomechanical properties between different subsets of patients with SSc and healthy control subjects.
Biomechanical properties of skin particularly depend upon the dermis, which comprises most of the overall skin thickness, and together with a thin epidermis mainly determine skin response under applied pressure.8,9 Collagen content, which is the major dermis component (collagen comprises about 75% of dry dermis weight), mainly determines skin dynamics under stress. Enzymatically isolated collagen fibres under load have shown a “stress-strain curve” similar to that of skin samples.10 At lower loads collagen fibres become aligned (“take up the strain” or “slack phenomenon”) in the load direction, and when collagen fibres become fully oriented, the resistance to further extension rapidly increases, and from this point is governed by the behaviour of the collagen itself.9 Altered collagen metabolism in SSc leads to the accumulation of large amounts of dermal collagen and increased skin thickness, which in turn interferes with skin extensibility and stiffness under stress. Alteration in biomechanical skin properties is therefore likely to reflect, in part, abnormalities in dermal collagen content. Mucopolysaccharides comprise about 20% of dry dermis weight and are responsible for binding of intradermal fluids. As the meshwork moves under pressure, these structures contribute to extensibility, especially under stable pressure when additional skin stretch might be achieved. These viscoelastic skin properties are impaired in inflammatory skin conditions where oedema and interstitial free fluid accumulation exist. Elastin (about 5% of dry dermis weight) mainly contributes to skin elasticity, acting as an energy store to return the collagen fibres to their relaxed condition after interruption of the load. Decreased elasticity has been seen in patients with cutis laxa, in which the elastin network is thought to play a part.7,14
Correlation between structural skin abnormalities and biomechanical properties should make precise and objective skin assessment possible. Vacuum suction devices have been used for assessment of biomechanical features of skin in patients with polyfibromatosis, scleromyxoedema, diabetes mellitus, and patients undergoing chronic haemodialysis. Significant changes in skin extensibility and elasticity have been seen in these groups compared with healthy controls.15,16 Pierard and Lapiere found reduction in skin extensibility in patients with acrosclerosis,7 and other investigators have shown significantly higher skin thickness and stiffness while using a torsion method in morphoea skin and in patients with dcSSc.17 A number of studies of experimental wounding have confirmed an association between biochemical changes in skin composition and differences in skin thickness with biomechanical changes assessed using the BTC-2000.22,23
We found that reduced skin extensibility in patients with SSc is mainly reflected by reduction in skin elastic deformation (ED—later phase of strain) and ultimate (total) deformation (UD). These indices were consistently significantly lower in both groups of patients with SSc compared with healthy controls on forearm and shoulder skin. Reduction in skin extensibility was significantly prominent in patients with dcSSc. Resistance to stress (PDR) was significantly higher in both SSc groups than in healthy controls on forearm and shoulder.
Our control data confirm that biomechanical properties of healthy skin vary between different sites. Thus we found an increase in extensibility (ED, UD, VED) and reduced resistance to stress (PDR) on shoulder skin (compared with forearm or back skin) in healthy controls. It might be assumed that such high elastic properties of shoulder skin contribute to the large range of motion of the shoulder joint. In patients with SSc, however, biomechanical properties of shoulder skin were substantially impaired, even in patients with lcSSc, despite a clinically normal skin appearance in this area. Significant reduction of skin deformation and high resistance to stress of the back skin in patients with dcSSc correlated with higher total and local clinical skin score. A reduction in viscoelasticity was seen in all areas measured in patients with dcSSc compared with healthy controls and patients with lcSSc; this may reflect continuing skin inflammation and oedema, although these were not prominent features macroscopically in our patients with dcSSc, many of whom had late stage disease. Reduced viscoelasticity was not a feature of patients with lcSSc, which in turn may reflect longer disease duration in patients with limited disease and a likely tendency to fibrotic rather than inflammatory processes.
We have shown that impaired biomechanical skin properties, such as reduced extensibility (ED, VED) and increased resistance to stress (PDR), are features of affected skin in scleroderma. The degree of impairment correlated with the severity of skin changes. Finding impaired skin extensibility on the shoulders in patients with lcSSc may be explained by subtle morphological skin changes and, possibly, skin abnormalities are more extensive in this subset of patients than is generally perceived, as has been shown for microvascular alterations in clinically unaffected skin in SSc.24
Analysis of biomechanical variables related to the sclerosis score at individual sites in the dcSSc cohort confirms that these properties are significantly altered between sites with different skin scores. Interestingly the same trend was observed for VED and UD, which decreased, and for PDR, which increased, with higher skin score. The BTC-2000 has the advantage of generating continuous rather than categorical data and so may be more effective for assessing change in skin sclerosis over time, although this will need to be examined further in longitudinal studies. Future studies might include biochemical analysis of skin biopsy specimens taken from sites at or near those sampled non-invasively to allow formal assessment of the potential biochemical correlates with altered biomechanical variables. In this way it is possible that non-invasive testing may provide a clue to the nature of sequential biochemical changes within the skin in SSc.
In summary, our results confirm that SSc has a significant effect on biomechanical skin properties. The BTC-2000 suction device has the advantage of providing non-invasive in vivo skin assessment in patients with scleroderma and may prove to be a useful tool for identifying subtle skin changes which cannot be judged by generally used clinical methods. Further longitudinal studies are necessary to define fully its place in disease assessment and its potential role in evaluation of the effectiveness of treatments for this intractable disease.
Acknowledgments
The authors are grateful to Professor Rodney Grahame for valuable discussions about biomechanical skin properties, to Larry Perry, of Surgical Research Laboratories Inc, for advice about use of the BTC-2000, and the Arthritis Research Campaign (UK) and Raynaud's and Scleroderma Association (UK) for financial support.