Article Text

Abstract
Background Physical disability is a main outcome in rheumatoid arthritis (RA) which tends to increase with comorbidities. However, the extent to which comorbidities contribute to the multifactorial process of disability has not been investigated.
Objective To quantify the contribution of comorbidity to physical disability in patients with RA.
Methods In a prospective cohort study, age-adjusted Charlson comorbidity index (CCIA), serial measurements of disease activity and functional disability (evaluated by the Health Assessment Questionnaire Disability Index, HAQ) of 380 patients with established RA seen at an outpatient clinic over 1 year (June 2007 to July 2008) were ascertained. The association between comorbidity and physical disability was assessed using analysis of variance (ANOVA) and adjusted general linear regression models.
Results Four patient groups with increasing levels of comorbidity (CCIA 0, 1–2, 3–4 and 5–9; potential range 0–38) were defined. Mean HAQ scores were significantly different across these groups (0.67, 0.80, 1.24, 1.40, respectively; p<0.001) and also when adjusted for disease activity, gender and disease duration in the regression model (0.84, 0.88, 1.14, 1.48, respectively; p<0.001). The effects of CCIA on disability were similar within different strata of disease activity: namely, remission (0.26, 0.31, 0.48 and 0.88, p<0.01); low disease activity (0.83, 0.78, 0.98 and 1.36, p<0.01); and moderate to high disease activity (1.22, 1.33, 1.70 and 1.91, p<0.01), and thus were independent of disease activity. Several sensitivity analyses, including the use of the Short Form Health Survey (SF-36), confirmed these observations.
Conclusion Physical disability becomes worse with increasing levels of comorbidity, irrespective of disease activity.
Statistics from Altmetric.com
Introduction
Physical disability is a major outcome of many chronic diseases, especially rheumatoid arthritis (RA), and prevention of disability is therefore an important therapeutic target. Measurement of physical function at any point in time, however, constitutes only a cross-sectional snapshot of the underlying events and their complex interaction that together lead to disability. Functional disability in a chronic disease has many different aspects and causes, some of which are related to the chronic disease itself, while others are related to other factors in the context of the patient's life.
RA is a paradigmatic chronic inflammatory joint disease in which disease-related factors such as the active disease process and chronic joint damage have been well established as causes of functional disability.1,–,4 However, the influence of factors not directly related to RA have not been sufficiently addressed in the literature.5 Specifically, patients suffering from RA can develop extensive comorbidities.6,–,8 In parallel, advancing age over the long course of the disease may considerably contribute to increasing levels of comorbidity,9 10 while age itself is associated with a decrease in the capacity to function physically.11 12 Overall, the interplay of comorbidity and physical function is unclear,13 and the interpretation of physical disability in a typical patient with RA can be difficult.
Although interactions of physical disability and comorbidity have been suggested,9 14 these analyses are commonly based on circumstantial evidence and not on the usage of valid and broadly applicable instruments.
In the present study we have evaluated the contribution of comorbid conditions to physical disability in patients with RA, where a solid body of literature already exists on disease-related disability. Using well-established and valid measures of disability and a broadly applicable comorbidity index which allow comparisons with non-rheumatic diseases, we quantified the impact of comorbidity on disability and analysed whether such effects are independent of disease activity.
Methods
Patients
For entry into the study, patients had to fulfil three eligibility criteria: (1) RA according to the American College of Rheumatology (ACR) classification criteria15; (2) availability of complete documentations of the outcome measures detailed below from at least two visits between 1 June 2007 and 1 July 2008; and (3) a last visit to the clinic within 6 months preceding July 2008. At our outpatient clinic, patients with RA are seen regularly, usually every 3–4 months, and their clinical and laboratory variables are documented prospectively in a longitudinal observational database.16
Since there were no additional exclusion criteria, the study population (n=380) showed a wide range of disease activities, disease durations and comorbid conditions representative of the RA population visiting our clinic. All patients gave their informed consent for anonymous analysis of their data when they were enrolled into the database and the data collection was approved by the local ethics committee.
Outcome measures
Health Assessment Questionnaire disability index (HAQ)
As a part of every routine visit, the Health Assessment Questionnaire disability index (HAQ) is collected as a measurement of functional disability and the results are entered into a database. The HAQ score reflects the mean of the highest values within each of eight domains (dressing, rising, eating, walking, hygiene, reach, grip and errands or chores, with a range of 0–3 where lower values represent better function.17 We calculated HAQ averaged over time (HAQT) of scores collected during the time period investigated (1 June 2007 to 1 July 2008) to eliminate short-term variability that is commonly seen with HAQ scores.18
Short Form-36 Health Survey (SF-36)
The SF-3619 20 constitutes a questionnaire comprised of 36 items organised into eight domains, each scaling between 0 and 100, with higher values representing better health states. Domains include physical function (PF; 10 items), physical role (RP; 4 items), bodily pain (BP; 2 items), general health perception (GHP; 5 items), vitality (VT; 4 items), social function (SF; 2 items), emotional role (RE; 3 items) and mental health (MH; 5 items). The domains can be further aggregated into two summary measures, the physical component score (PCS; including PF, RP, BP and GHP) and the mental component score (MCS; VT, SF, RE and MH).
Disease activity
The following documented core set variables of disease activity were retrieved from the database: visual analogue scale (0–10 cm) for pain (VAS-pain), patient global assessment of disease activity (PGA) and evaluator global assessment of disease activity (EGA); 28 swollen joint count (SJC28) and 28 tender joint count (TJC28); and the acute phase reactants C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). The Clinical Disease Activity Index (CDAI) and the Simplified Disease Activity Index (SDAI) were calculated based on these variables according to the following formulae:
CDAI = SJC28 + TJC28 + PGA (in cm) + EGA (in cm)21
SDAI = SJC28 + TJC28 + PGA (in cm) + EGA (in cm) + CRP (mg/dl)22
Cut-off points used to separate the states of remission, low, moderate and high disease activity were 2.8, 10 and 22, respectively, for the CDAI, and 3.3, 11 and 26, respectively, for the SDAI.23
Comorbidity
One of the most established and validated instruments to assess comorbidity is the Charlson comorbidity index (CCI).24 The index is based on medical chart review and assigns a weight of 1–6 to each of the comorbid conditions according to the risk of 1-year mortality. The CCI as a sum of the weights of each condition can range from 0 to 33. A modification of the CCI, which considers the effect of ageing on mortality, has been published.25 This index (CCIA) uses the original CCI plus one extra point for each decade of age above 50 years. Since in our study we are dealing with patients with an average age of 61 years, we deemed the CCIA to be more appropriate for the main analysis. However, we used the CCI as well as a simple enumeration of each patient's comorbidities without weighting (CCIN) in additional sensitivity analyses.
Chart review was performed by one of the authors (HR) for all patients. To ensure inter-rater reliability, chart review on a random sample of approximately 15% of patients from the cohort (n=54) was performed by a second physician less than 1 week apart and blinded to the results of the other. The intraclass correlation coefficient (ICC) of 0.89 (95% CI 0.82 to 0.93) indicated good inter-rater reliability.
Statistical analysis
We first determined the univariate relationship of laboratory and clinical findings at the baseline visit as well as of CCI, CCIA and CCIN with functional disability (by HAQT) by use of Spearman's correlation.
To investigate the potential association between comorbidities and physical function we used one-way analysis of variance (ANOVA) of CCIA on HAQT. We divided the independent variable into four groups (Group 1: CCIA = 0; Group 2: CCIA = 1 or 2; Group 3: CCIA = 3 or 4; Group 4: CCIA = 5 or more) and performed a test for a linear trend component. This grouping was arbitrary, but attempted to achieve sufficient numbers of individuals in the various subgroups.
We then extended the ANOVA to a generalised linear model (GLM) to adjust the association of CCIA and HAQT for the effects of additional variables such as gender, disease activity and disease duration. The adjusted effects of CCIA on HAQT were calculated using estimated marginal means (EMM), setting the covariate levels to the cohort means in all comorbidity groups.
To test whether the association of CCIA with HAQT was consistent in patients with different levels of disease activity, we performed two analyses: first, we stratified the analysis for patients in remission (time-averaged CDAI, CDAIT, ≤ 2.8), patients in low disease activity (LDA) (2.8<CDAIT≤10), patients in moderate disease activity (10<CDAIT<22) and patients in high disease activity (CDAIT >22). Since the numbers in the group of patients in high disease activity were too small for the subgroup analysis, we combined this group with the patients in moderate disease activity. We then reassessed the GLM described above (without CDAIT as covariate as disease activity was stratified). Second, we calculated EMM of HAQT in the complete patient cohort and set the covariate level of CDAIT to 2.5 for remission, to 5 for LDA, to 16 for moderate disease activity and to 30 for high disease activity (adjusted analysis).
For the purpose of sensitivity analyses we recalculated ANOVA in three ways. First we used the CCI (Group 1: CCI=0; Group 2: CCI=1; Group 3: CCI=2; Group 4: CCI=3 or more) or the number of comorbid conditions, the CCIN (Group 1: CCIN=0; Group 2: CCIN=1; Group 3: CCIN=2; Group 4: CCIN=3 or more) as independent variables in the model instead of the age-adjusted version (CCIA), and then we used the generic SF-36 as a dependent variable in the model.
All analyses were carried out using SPSS Version 16.
Results
Study population
Our dataset contained 1605 visits of 380 patients whose demographic and baseline clinical characteristics are shown in table 1. The HAQ at first study visit ranged from 0 to 3 with a mean±SD of 0.94±0.82. This considerable impairment of physical function is in line with the established disease in most patients.
Characteristics of 380 patients at first study visit (80.5% female; 58.4% rheumatoid factor positive)
A CCI of 1–6 was found in 112 patients (29.5%), while the remainder had a CCI of 0. For these 112 patients with at least one comorbidity, mean±SD values of CCI were 1.61±0.9 with a median (quartiles) of 1 (1; 2). Comorbidities and the numbers of patients affected are shown in table 2. The age-adjusted CCIA of the 112 patients with comorbid conditions ranged from 1 to 9 with a mean score of 3.82±1.6; the CCIN was 1 in 68.8% of these patients, 2 in 25% and ≥3 in 6.3%.
Comorbid conditions of the Charlson comorbidity index (CCI) and their weights, as well as number of patients affected by the comorbidity
Correlation of core set variables and comorbidities with HAQ
Spearman correlation analyses showed low to moderate but significant correlations of CCIA, CCI and CCIN with HAQT (r=0.3; r=0.24; r=0.24, respectively; p<0.001, table 3). These values were in the range observed for correlations of evaluator global assessment, CRP and age with HAQT, and were higher than those for SJC. We found no significant correlation of body mass index with functional disability (r=0.1; p=0.07).
Bivariate Spearman correlation of time-averaged values of Health Assessment Questionnaire (HAQT) with baseline variables of disease activity and measures of comorbidity
Crude and adjusted effects of comorbidities on physical function
As shown in figure 1A, using ANOVA, a consistent increase in physical disability from Group 1 to Group 4 of CCIA (p<0.01) was observed. When we adjusted the effect of CCIA on HAQT for other variables associated with the dependent variable such as CDAIT, gender and disease duration (table 3), the model still showed a high level of significance (R2=0.48, p<0.001; figure 1B). Interestingly, across the CCIA groups the adjusted scores of HAQT (EMM) increased from 0.84 in group 1 to 0.88, 1.14 and 1.48 in groups 2, 3 and 4, respectively, further supporting an independent effect of comorbidity levels on physical disability. In a sensitivity analysis we replaced CDAI with SDAI, another measure of disease activity comprising a laboratory variable (CRP) revealed very similar results (0.84, 0.86, 1.16 and 1.48 for groups 1–4; p<0.001).

Effects of comorbidity on functional disability. (A) ANOVA showing increase in mean time-averaged Health Assessment Questionnaire (HAQT) including the respective 95% CI (error bars) across groups with increasing comorbidity levels in the age-adjusted Charlson comorbidity index (p<0.001); (B) General linear model adjusted for duration of rheumatoid arthritis, time-averaged Clinical Disease Activity Index Area (CDAIT) and gender showing estimated marginal means of HAQT in a female patient with rheumatoid arthritis for 11.7 years and a CDAIT of 8.7 (respective cohort means) which follow the course trend as in the crude analysis and are also highly significant (p<0.001).
To test whether there is an interaction of different comorbidities which aggravate each other's effect on HAQ, we assessed the most prevalent comorbidities in our cohort: diabetes (dm), chronic pulmonary disease (cpd) and peripheral vascular disease (pvd) for pairwise interaction. We found no significant interaction term (dm*cpd, p=0.556; cpd*pvd, p=0.806; dm*pvd, p=0.452).
Adjusted effects of comorbidities on physical function in patients with different disease activity states
First we stratified our sample into patients in remission, LDA or moderate/high disease activity (MDA/HDA) and then quantified the effects of CCIA on HAQT in different states of disease activity. Interestingly, even for the subgroup of patients in remission, EMM adjusted for duration and gender again showed significant differences of HAQT values across the four groups of CCIA (mean values 0.26, 0.31, 0.48 and 0.88, respectively; p<0.01). For the subsets of patients with LDA and MDA/HDA, the EMM of HAQT were higher than those of patients in remission as a consequence of the well-known contribution of disease activity to impairment of physical function. However, the HAQT increased to a similar extent across all four comorbidity groups in patients with LDA (0.83, 0.78, 0.98 and 1.36) or MDA/HDA (1.22, 1.33, 1.70 and 1.91; figure 2A). When comparing the results of HAQT among patients in different disease activity states, the increases of HAQT across the respective CCIA groups 1–4 were very similar in all disease activity states, amounting to an increase of 0.62 for patients in remission and 0.69 for those with MDA/HDA, while for patients with LDA this increase was only slightly lower (0.53 increase between groups 1 and 4).

Effects of comorbidity on functional disability according to different levels of disease activity. The estimated marginal means (EMM) of the time-averaged Health Assessment Questionnaire (HAQT) show the expected results in a female patient with rheumatoid arthritis for 11.7 years (cohort mean). (A) Stratified analysis: patients were analysed into subgroups defined by the time-averaged Clinical Disease Activity Index (CDAIT); (B) Adjusted analysis: EMM were estimated for a CDAIT of 2.5 (remission), 5 (low disease activity), 16 (moderate disease activity) or 30 (high disease activity). The increase in HAQT is independent of disease activity levels.
In adjusted analyses based on the whole patient sample, we reassessed GLM and calculated EMM of HAQT by setting levels for CDAIT to 2.5 (remission), 5 (LDA), 16 (MDA) or 30 (HDA). The EMM of HAQT in the four groups of CCIA showed similar trends to those found in the stratified analysis (figure 2B): remission 0.49, 0.54, 0.80 and 1.14; LDA 0.63, 0.67, 0.94 and 1.27; MDA 1.23, 1.27, 1.54 and 1.87; and HDA 1.99, 2.04, 2.3 and 2.64, respectively, for groups 1–4.
Sensitivity analyses
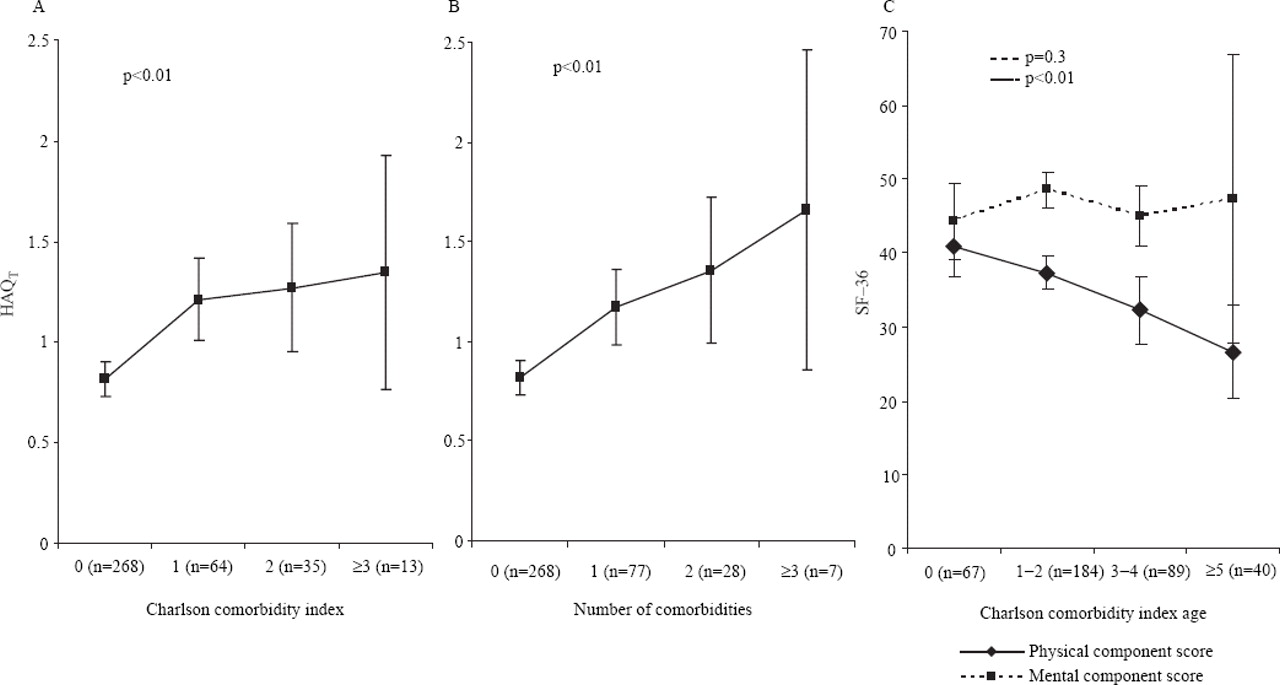
We performed several sensitivity analyses. First, we obtained SF-36 results from 185 random patients of the total cohort (48.7%) and again calculated the crude effect of comorbidities on physical function by ANOVA using the SF-36 summary indices (PCS and MCS) as dependent variables. There was an almost linear decrease in PCS within the four groups of CCIA whereas the MCS showed no association with comorbidity (figure 3C). This observation critically supports the theoretical background of our analyses—namely, that comorbidity influences physical function.
{kind=link}
{kind=link}
{kind=link}
Sensitivity analyses showing an increase in the mean area time-averaged values of the Health Assessment Questionnaire (HAQT) within different groups. (A) Original Charlson comorbidity index (CCI); (B) number of comorbidities without weighting (CCIN). These associations were significant in both analyses (ANOVA for linear trend, p<0.01); (C) the Short-Form Health Survey (SF-36) was used instead of HAQT and showed a significant (p=0.003) decrease in the physical component score (PCS) in the respective groups of age-adjusted CCI whereas differences in the mental component score (MCS) in these groups were not significant (p=0.31).
Second, we calculated ANOVA for the original CCI and the CCIN (each divided into four groups) instead of CCIA. The results of these analyses likewise revealed significant differences (p<0.01) across comorbidity groups (figure 3A,B).
Discussion
This study shows a close association between physical disability and comorbid conditions by three major findings: (1) physical disability increases significantly with higher levels of comorbidity; (2) this effect is independent of disease activity; and (3) this effect can be quantified. These data expand our understanding of disability and its causes.
In general, physical disability in RA is a consequence of the active disease process, which is usually reversible, and the joint damage accrued, which is usually irreversible.1 This inherent duality needs consideration when disability states are interpreted. Importantly, while under ideal circumstances and in the absence of severe organ damage physical disability should fully reverse with appropriate treatment, contextual factors not primarily related to the disease lead to an apparent resistance of functional disability to respond to treatment. The observation that the effects of comorbidity on functional impairment are not only independent of disease activity but may even constitute a relatively constant value across all disease activity states indicates that comorbid conditions increase physical disability substantially across the whole disease spectrum. This irreversible functional component becomes increasingly important in patients close to remission. In fact, based on our analyses, the average HAQ in a group of patients with several comorbid conditions would be somewhere around 0.6, even if the best possible treatment was used. This floor effect of functional improvement is an important aspect when evidence of therapeutic efficacy needs to be provided, such as for reimbursement of interventions. Importantly, our findings did not depend on the instrument employed. While they were initially derived using the HAQ, similar observations were made when evaluating the SF-36. Our data therefore support the view that measures of physical function do not reflect only the disease process but rather a combination of process, outcome and patients' health. As a consequence, inclusion of measures of function in disease activity indices, such as in the current ACR response criteria, might not be ideal.
The implications of our findings are therefore fundamentally related to the fact that impairment of physical function is the most important outcome in RA since it affects the patient's well-being at any point in time as well as long-term consequences, inability to work and mortality.26,–,32 Thus, disability constitutes a significant burden for the individual and for society. One reason for the association of HAQ with mortality in RA could in fact be its association with comorbidities, as shown in the present study.
With our findings, we are now able to provide a rational background and numerical estimation of the effects of comorbidity on function. In this respect, the four groups formed by the values of the comorbidity indices used here can be approximated to reflect a patient with no, little, moderate and considerable comorbidity. As our abilities to treat chronic diseases improve over time, the issue of irreversible functional disability becomes increasingly relevant since many patients can be relieved from most of their disability related to disease activity, but not from disability related to other causes.33 34
The strength of our study includes the use of a large sample of patients from daily practice rather than typical trial data which may be misleading given the typical exclusion criteria. Trial patients are usually excluded on the basis of comorbidities and are selected for high disease activity; neither was the case for our patients. One limitation of our study might be that we used the CCI, which was developed primarily to predict mortality and not functional disability as reflected in part by the weights assigned to each of a number of comorbidities. However, when we analysed the (unweighted) number of comorbidities (CCIN) we found similar results, indicating that the mortality-based weights are not decisive. Nevertheless, our analyses were not able to overcome the fact that the CCI incorporates only a limited number of comorbid conditions, excluding others such as depression or osteoporosis which might be more prevalent in patients with RA and could be relevant to physical disability. This might also reflect the low prevalence of comorbidities in our population. Second, radiographic data were not available for the patients analysed in this study. However, several studies have shown a close relationship between radiographic progression and increasing disease duration2 35 and therefore, as a surrogate for the effect of structural damage, we adjusted our results for the effects of disease duration. Third, our analyses are model-based and will have potential constraints when directly applied to the individual patient. Our results cannot therefore be used to quantify exactly the impact of given comorbidities on a single patient but can estimate their impact on function in patients with RA.
In summary, adequate physical functioning is a central process and outcome measure for patients with RA. Based on our data, it might be relevant to expand our current knowledge on disability, encompassing the context of a patient as a whole, including the comorbidity status. This can have a large impact on the interpretation of disability in health economic studies and policy decisions, similar to daily life practice when physical function often withstands improvement despite intensive and effective treatment.32 36 37
Acknowledgments
We are indebted to our colleagues at the Division of Rheumatology, Department of Internal Medicine 3, Medical University of Vienna for their continuous and precise input of data into the observational database. We thank Dr Anna Floymayr for performing a chart review on comorbid conditions of a subset of patients which enabled us to ascertain inter-rater reliability.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the local ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.