Article Text

Abstract
Objectives: The aim of this study was to determine the recurrence risk of psoriatic arthritis (PsA) and uncomplicated psoriasis in first-degree relatives (FDRs) of patients with PsA.
Methods: All available FDRs (full siblings, parents and children) of 100 consecutive consenting patients attending a PsA clinic were evaluated for the presence of psoriasis and PsA using a standard protocol. The protocol included a screening questionnaire, physical examination by a rheumatologist, and radiographic and laboratory assessment. The prevalence of PsA and psoriasis in FDRs of the index cases was determined, and the recurrence risk ratio (λ) was calculated, assuming a population prevalence of PsA of 0.25%, and a population prevalence of psoriasis of 2%.
Results: The 100 probands had 533 relatives. Eighty-four of them were deceased and 53 were unavailable (age <16 years). Of the remaining 396 FDRs, 107 did not participate (living too far away/did not consent). Thus, 289/396 (73%) of the available FDRs participated in the study. There were 130 siblings, 108 parents and 51 children. The prevalence of PsA and psoriasis among FDRs was 7.6% and 15.2%, respectively. The λ1 was 30.4 for PsA and 7.6 for psoriasis. The prevalence of PsA and psoriasis in siblings was 7.7% and 17.7%, respectively. The λS was 30.8 for PsA and 8.8 for psoriasis.
Conclusions: The recurrence risk ratio for both PsA and psoriasis is high in FDRs and siblings of patients with PsA. These results confirm that both PsA and psoriasis have a strong heritable component.
Statistics from Altmetric.com
Psoriatic arthritis (PsA), defined as an inflammatory arthritis associated with psoriasis usually seronegative for rheumatoid factor, is now recognised as a specific inflammatory arthritis.1 Based on a telephone survey conducted recently by the National Psoriasis Foundation in North America, the prevalence of PsA is estimated to be about 0.25%.2 PsA is closely related to psoriasis, a chronic inflammatory skin disease that affects about 2% of the population in North America.3 Psoriasis is highly heritable, as evidenced by an increased rate of concordance in monozygotic versus dizygotic twins (35–72% vs 12–23%, respectively).4 The recurrence risk ratio for psoriasis is estimated to be between 4 and 10.5 About 30% of patients with psoriasis have PsA.1 Therefore, it is likely that PsA also has a significant genetic component. However, the magnitude of this risk is still uncertain as it is based only on a couple of small studies on familial aggregation.5 Another method to study the heritability and to dissect out genetic and environmental factors in disease susceptibility is to conduct twin studies.6 However, unlike psoriasis, in PsA there are no large twin cohorts available. There is only one twin study reported in PsA that could not demonstrate a genetic effect on PsA as it was underpowered.7 Thus, familial aggregation is the only measure of the genetic burden of PsA available.
A study on familial aggregation is the first step in pursuing a possible genetic aetiology to a disease.8 If the phenotype is a binary trait, familial aggregation is assessed by the recurrence risk ratio (λ). The recurrence risk ratio λR is defined as the prevalence of the disease in relatives of type R of affected cases divided by the prevalence in the general population.9 Its is important to have an accurate assessment of the relative risk as this has implications with respect to selection of sample size for case–control studies (including genome-wide association studies), modelling for potential linkage studies (multiplicative or additive model) and possibly genetic counselling.6 Interestingly, in a recently published genome-wide association study that looked at seven common diseases, the number of susceptibility loci determined correlated with the heritability of the disease studied.10
In a study conducted in the early 1970s, the prevalence of PsA among first-degree relatives (FDRs) of probands with PsA was 5.5% compared with the calculated prevalence in the UK population of 0.1%.11 The calculated λ1 was therefore 55. The prevalence of psoriasis in FDRs of probands with PsA was also increased compared with the population control. A recent UK study reported the prevalence of PsA in siblings to be 14.3% and that in the general population to be 0.3%.12 The calculated λS was therefore 47. Thus there have been only two studies on the familial aggregation of PsA, both conducted in the UK, that have demonstrated a high recurrence risk ratio of PsA in FDRs. However, these studies were conducted before broadly agreed upon or validated classification criteria for PsA were developed. The CASPAR criteria for the classification for PsA have recently been developed by a panel of international experts.13 This allows proper case definition for conducting genetic studies on PsA. The CASPAR criteria require the presence of inflammatory articular disease (joint, spine or entheseal) with at least three points from the following features: current psoriasis (assigned a score of 2; all other features are assigned a score of 1), a history of psoriasis (unless current psoriasis was present), a family history of psoriasis in a first- or second-degree relative (unless current psoriasis was present or there was a history of psoriasis), dactylitis, juxta-articular new bone formation, rheumatoid factor negativity and nail dystrophy.13
There are no studies that have determined the recurrence risk of PsA using the new CASPAR classification criteria for PsA. Moreover, the recurrence risk also depends on the environmental and ethnic background of the studied population.6 The objective of the present study was to determine the recurrence risk ratio of both PsA and uncomplicated psoriasis in FDRs of patients with PsA seen at the University of Toronto PsA clinic.
METHODS
The study was carried out at the University of Toronto PsA clinic where a longitudinal open dynamic cohort was established in 1978. Patients are followed at 6–12 month intervals according to a standard protocol.14 This study was approved by the Research Ethics Board of the University Health Network, Toronto, Canada. Consecutive patients with PsA were approached to participate in a family investigation. If a patient did not wish their family to participate or if there were no available family members, the next patient was approached until 100 probands were recruited. All available FDRs (full siblings, parents and children) of the 100 consecutive consenting probands were evaluated for the presence of psoriasis and inflammatory arthritis using a standard protocol which included a screening questionnaire, clinical examination by a rheumatologist, laboratory tests, and radiographs if clinically indicated. Probands and relatives were diagnosed on the basis of the presence of the Gladman modification of the Moll and Wright criteria and subsequently satisfied CASPAR criteria for classification of PsA.13 If an individual was not able to attend the clinic, they were either evaluated in their own home or were asked to complete a screening questionnaire that was validated in our clinic, and information was obtained from their primary care doctors and/or rheumatologist.15 Radiographs were obtained if clinically indicated for individual diagnosis.
Statistical analysis
The prevalence of PsA and psoriasis in FDRs was determined. The recurrence risk ratio in FDRs (λ1) and siblings (λS) was calculated assuming the population prevalence of PsA to be 0.25%, and that of psoriasis 2%.2 3
RESULTS
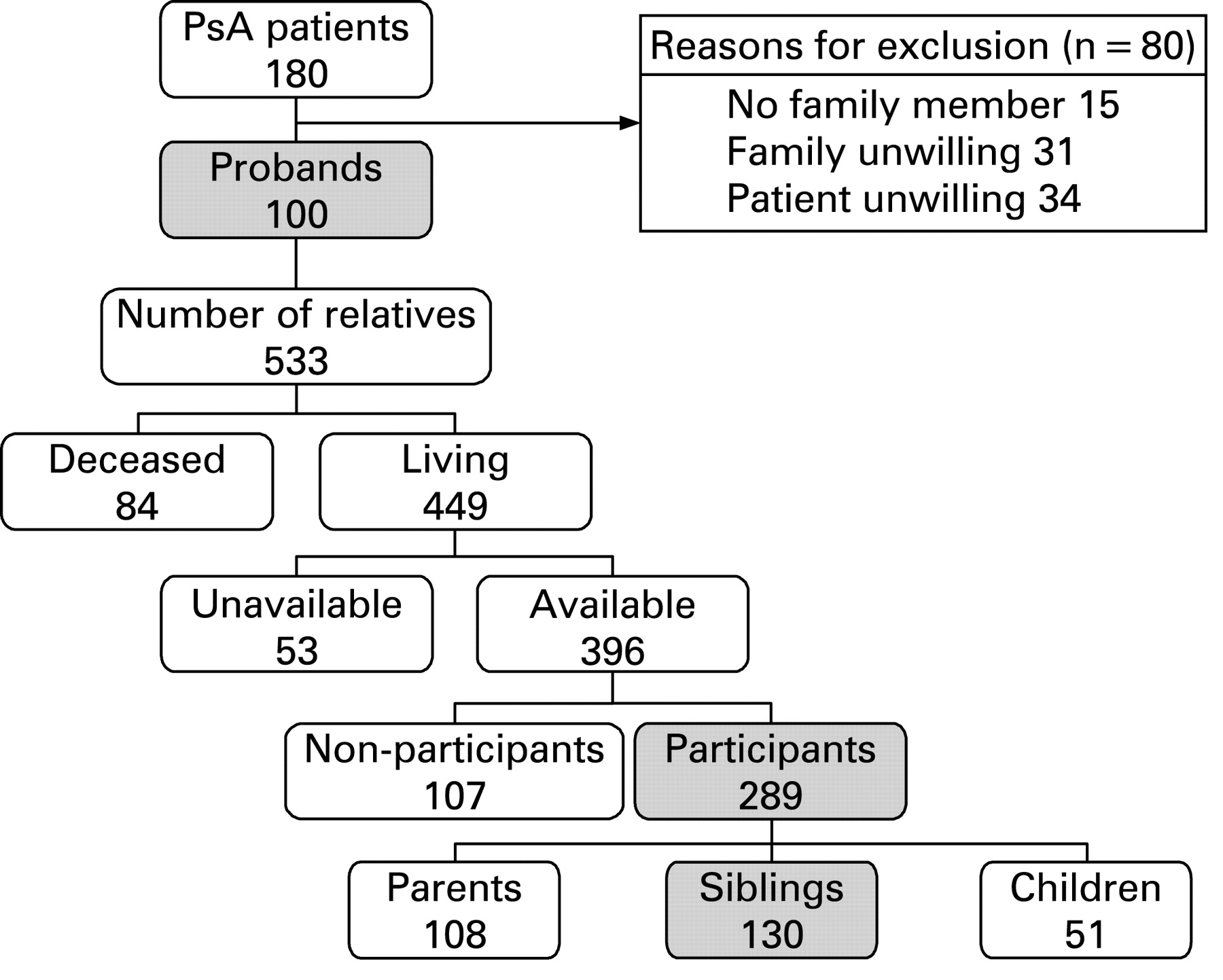
To recruit 100 probands, 180 consecutive patients attending the University of Toronto PsA clinic were approached. Eighty patients were excluded: 15 had no relatives, 31 had family members who were unwilling and 34 were unwilling to involve their families (fig 1). The demographic and disease characteristics of the participating probands (50 males) are given in table 1. Ninety-nine of the 100 probands were Caucasians of European ethnicity; the one remaining proband was a Caucasian of Egyptian ethnicity. Their mean age at first visit was 39 years, with PsA duration of 6 years, mean age at onset of psoriasis of 28 years and age at onset of PsA of 33 years. They had on average 12 actively inflamed (either tender or swollen) joints and 5 swollen joints, and a Psoriasis Area and Severity Index (PASI) score of 4, indicating mild to moderate psoriasis.16 Erosions were seen on radiographs of peripheral joints in 53% (using the modified Steinbrocker technique validated in our clinic), and 36% had at least unilateral grade 2 sacroiliitis (according to New York criteria) on pelvic radiographs.17 18 Forty-three probands were currently on non-steroidal anti-inflammatory drugs (NSAIDs) and 34 were currently on disease-modifying antirheumatic drugs (DMARDs): methotrexate 20, sulfasalazine 9, prednisone 7, (hydroxy)choloroquine 5, others 5. Forty-five had received DMARDs in the past. When compared with the 80 patients who had declined to participate in the study, the 100 study participants were more likely to be males (50 vs 66, p = 0.02), have a family history of psoriasis (46 vs 29, p = 0.02), a lower age at first visit to the clinic (39 years vs 43 years, p = 0.01) and a lower PASI score at first visit (4 vs 7, p = 0.02). When compared with other patients attending our clinic, the study participants were more likely to have an earlier age at onset of PsA (33 years vs 37 years, p = 0.003), shorter disease duration at first visit (6 years vs 8 years, p = 0.03), shorter duration of psoriasis (11 years vs 16 years, p<0.0001), higher swollen joint count (5 vs 3, p = 0.004) and lower PASI score (4 vs 6, p = 0.003) at first clinic visit
{kind=link}
Flow chart showing recruitment of study subjects. PsA, psoriatic arthritis.
The 100 probands had 533 relatives. After excluding 84 deceased and 53 who were <16 years of age, 396 FDRs were potentially available. Of these, 289 (73%) agreed to participate and were evaluated for the presence of PsA and psoriasis. There were 108 parents, 130 siblings and 51 children (fig 1). Of those who participated, 206 (71%) were assessed by clinical examination and the remaining 83 (29%) were evaluated by a screening questionnaire and radiographs, if indicated.
Of the 289 FDRs, 22 (13 males) had PsA (mean age at diagnosis 39 years) and 44 (20 males) had psoriasis only (mean age at diagnosis 27 years). Two FDRs were on DMARDs (methotrexate 1, prednisone 1) and 14 were treated with NSAIDs. Three FDRs were diagnosed with PsA and 6 with psoriasis based on the screening questionnaires, notes from family doctor/rheumatologist and radiographs. The prevalence of PsA and psoriasis without arthritis was therefore 7.6% and 15.2%, respectively. The λ1 was calculated at 30.4 and 7.6, respectively. If only those patients who underwent a clinical evaluation are considered, the λ1 is calculated at 36.9 for PsA and 9.5 for psoriasis alone. Ten of the 130 siblings had PsA and 23 had psoriasis alone. The prevalence of PsA and psoriasis without arthritis was therefore 7.7% and 17.7%, respectively. The λS was calculated at 30.8 and 8.8, respectively (table 2).
DISCUSSION
Our study shows that the recurrence risk ratio for PsA and psoriasis among FDRs of patients with PsA in a Canadian cohort is 30.4 and 7.6, respectively. This study confirms two previous observations of high familial recurrence risk of PsA, made in the UK. In a study of consecutive families of probands with PsA, the hereditability was measured by the Kellgren factor at 48.11 Applying Risch’s method, the calculated λ1 was 55,9 while the λS was 27. Likewise in a sibling study the λS was calculated as either 47, if a prevalence of 14% among the siblings is considered, which includes enthesitis as the only feature of PsA, or as 30, if only those with synovitis are considered.12 The present study also confirms previous observation of the close association of PsA with psoriasis, since the λ for psoriasis was high in probands with PsA. Due to the fact that the study was restricted to 100 consecutive probands, and only a relatively small number of family members were affected, the study was underpowered to look at the concordance with respect to degree of psoriasis, pattern of arthritis and parent of origin effect.
The strength of our study is that consecutive patients were recruited, thus minimising bias in recruiting patients with a family history of psoriasis or PsA, and a large number of relatives were evaluated in detail. Patients and relatives were evaluated according to a standard protocol and classified according to the most recently developed classification criteria.13 Radiographs of relatives were performed for individual clinical diagnosis. The results of our study prove the high genetic susceptibility to PsA, and are consistent with the results from the previous studies.11 12 However, the recurrence risk ratio obtained is lower. This could be due to the fact that unselected consecutive consenting probands were recruited for the study. Moreover, we did not classify patients with enthesitis alone as having PsA as was done by Myers et al in their study.12 In fact, if those siblings with enthesitis alone are excluded the λS in their study would be 30, which is almost identical to the value obtained in the current study. One possible reason could also be the lack of sensitivity of the CASPAR criteria for detecting early PsA. However, this is unlikely as we have previously shown that the CASPAR criteria are sensitive in classifying patients with early PsA and established PsA.19
One limitation of our study was that only 71% of FDRs who had agreed to participate in our study were clinically evaluated by us. In the 29% of FDRs who were not available to be examined by us directly, we based our diagnosis of being affected or unaffected on the screening questionnaire, reports from their family doctor or treating rheumatologists, and by radiographic evaluation, where indicated. Of the 83 FDRs thus evaluated, we diagnosed PsA in three and psoriasis in six. Since only a few subjects were thus diagnosed, our estimated λ may still be an underestimate. In fact, if we exclude patients evaluated using the screening questionnaire, the calculated λ1 for PsA is 36.9.
Numerous studies have shown that the greatest variability in calculating λ is due to the value one uses as the population prevalence. We have used the most recent estimate of the prevalence of PsA (0.25%) from North America for calculating the λ values.2 However, the prevalence of PsA in patients with psoriasis is estimated to be 30%,1 and the prevalence of psoriasis in the general population, 2%.3 These figures indicate that the true population prevalence of PsA may be higher than 0.25% and, consequently, the “true” recurrence risk ratio may be lower. In fact, a recent population-based study in Italy estimated a prevalence of 0.42%.20 On the other hand, several other studies suggest a lower estimated population prevalence of 0.14–0.2%.21–23 Therefore, the relative risk ratios may be higher. This underscores the need for studies on the prevalence of PsA in the general population, and the prevalence of PsA in patients with psoriasis. Another significant problem with studies determining recurrence risk ratios is that ascertainment bias and over-reporting can inflate the recurrence risk ratio.24 25 We have tried to minimise this inflation of risk by designing the study to include 100 consecutive consenting patients with PsA as probands, and by detailed evaluation of the relatives to determine phenotype. However, since we ascertained probands from a clinic and not from the general population, ascertainment bias could still persist.
As with all studies on familial aggregation, the effect of shared environmental risk factors cannot be discounted. Environmental risk factors such as trauma and immunological triggers (such as rubella vaccination) have been shown to be risk factors for onset of PsA.26 Additional studies are clearly needed to delineate further the environmental risk factors for PsA susceptibility.
Thus, the recurrence risk ratio for PsA is high, and we may conclude that PsA has a significant heritable component, although a large environmental influence cannot be ruled out. Further studies on the genetic and environmental risk factors for the susceptibility to and the expression of PsA are required, and are in progress. Indeed, using candidate gene-based association studies, a few susceptibility genes have been discovered.5 A recent genome-wide association study has confirmed previously reported loci and has identified new loci for both psoriasis and PsA.27
REFERENCES
Footnotes
Competing interests: None.
Funding: This study was supported by the Krembil Foundation. VC is supported by a Krembil Psoriatic Arthritis fellowship, and Post-Doctoral Fellowship Awards from the Canadian Arthritis Network and the Arthritis and Autoimmunity Research Centre Foundation, Toronto, Ontario, Canada. JEB was supported by an Arthritis Centre of Excellence and Krembil Psoriatic Arthritis Fellowship.
Ethics approval: This study was approved by the Research Ethics Board of the University Health Network, Toronto, Canada.