Article Text

Abstract
Objective: To evaluate the validity and reliability of the polymyalgia rheumatica (PMR) activity score (PMR-AS) for relapse diagnosis by general practitioners (GPs) who manage a large proportion of patients with PMR.
Methods: Seven clinical vignettes of PMR were used, for which 35 rheumatologists previously made a diagnosis of relapse or no relapse with greater than 80% agreement. These vignettes were submitted to 163 GPs, who were asked to assess disease activity using a visual analogue scale (VASph), this being the only physician-dependent component of the PMR-AS. The 1116 available vignette–GP combinations were used to assess differences in VASph assessed by GPs versus rheumatologists. Statistical associations linking a relapse diagnosis by the rheumatologists (the reference standard) to the value of the GP-assessed PMR-AS or its components (GP-assessed VASph, visual analogue scale pain score, C-reactive protein, morning stiffness and elevation of upper limbs) were evaluated.
Results: No significant differences were found between VASph scores by GPs versus rheumatologists for any of the vignettes. A relapse diagnosis was strongly associated with PMR-AS values of 7 or more (sensitivity 99.4%; specificity 93.3%; agreement 95.9% (95% CI 94.5% to 97.0%) with κ = 0.92). Of the 590 GP–vignette combinations with PMR-AS values lower than 7, all but three (0.5%) had no relapse diagnosis. Of 510 combinations with PMR-AS values of 7 or more, only 42 (8%) had no flare diagnosis.
Conclusions: This study supports the validity of the PMR-AS in primary care practice and provides evidence that a good scoring system can be useful to guide clinical and therapeutic decisions.
Statistics from Altmetric.com
Polymyalgia rheumatica (PMR) is an inflammatory joint disease of the elderly characterised by pain and morning stiffness in the neck and limb girdles, with elevation of laboratory markers for inflammation including the erythrocyte sedimentation rate (ESR) and serum C-reactive protein (CRP) level. Long-term corticosteroid therapy is the cornerstone of the treatment for PMR, and low dosages (10–20 mg prednisone/day) are often sufficient to correct the clinical symptoms and laboratory evidence of inflammation within a few days. The dosage is then tapered according to disease activity as assessed using a combination of clinical symptoms and ESR and/or CRP.1 Many patients can be tapered off glucocorticoid therapy after 1–2 years. However, relapses may occur, requiring glucocorticoid dosage increases, so that 50% of patients are still on treatment after 2–3 years or more.2 Long-term corticosteroid exposure in elderly patients, many of whom have co-morbid conditions, often generates adverse effects. In a database study, patients receiving treatment for PMR had a 2.5-fold increase in the risk of diabetes mellitus, vertebral fractures, femoral neck fractures and hip fractures, compared with the same-age general population.3 Furthermore, increases have been reported in the risk of myocardial infarction, heart failure, peripheral vascular disease and cerebrovascular disease. Although this increased cardiovascular risk may be related to long-term inflammation rather than to glucocorticoid therapy,4 carefully tailoring the glucocorticoid dosage to the patient’s needs is crucial in order to strike the best compromise between the risk of treatment-related adverse effects and the risks associated with uncontrolled inflammation.
Leeb and Bird5 developed a disease activity score for PMR (the PMR-AS), which is computed by summing five parameters: morning stiffness (MST, in minutes, multiplied by 0.1 for weighting purposes); ability to elevate the upper limbs (EUL, on a scale from 0 to 3); physician’s global assessment using a 10-point visual analogue scale (VASph); pain measured by the patient using a 10-point visual analogue scale (VASp); and the CRP level (in mg/dl). PMR-AS values lower than 7 indicate low disease activity, values between 7 and 17 moderate disease activity and values greater than 17 high disease activity (fig 1). The PMR-AS is well suited to everyday practice, and its usefulness has been further improved by the determination of cut-offs for disease remission and relapse. PMR-AS values between 0 and 1.5 thus suggest disease remission6 and values greater than 9.35 (in patients with previously controlled disease) or having increased by 6.6 or more between two visits suggest disease relapse.7 Studies consistently found that the PMR-AS was easy to use and valid when determined by rheumatologists,5–8 despite considerable interobserver variability in the VASph score, the only subjective component of the PMR-AS. However, general practitioners (GPs) play a major role in the management of patients with PMR. In a population-based cohort of PMR patients, the mean number of GP visits per person-year of follow-up was 7.0 during the first year (versus 2.2 for rheumatologist visits) and 3.8 during the second year (versus 0.8 for rheumatologist visits);9 39.6% of patients were managed only by GPs and 28% had a single rheumatologist visit. Therefore, the feasibility and validity of PMR-AS determination by GPs needed to be evaluated.
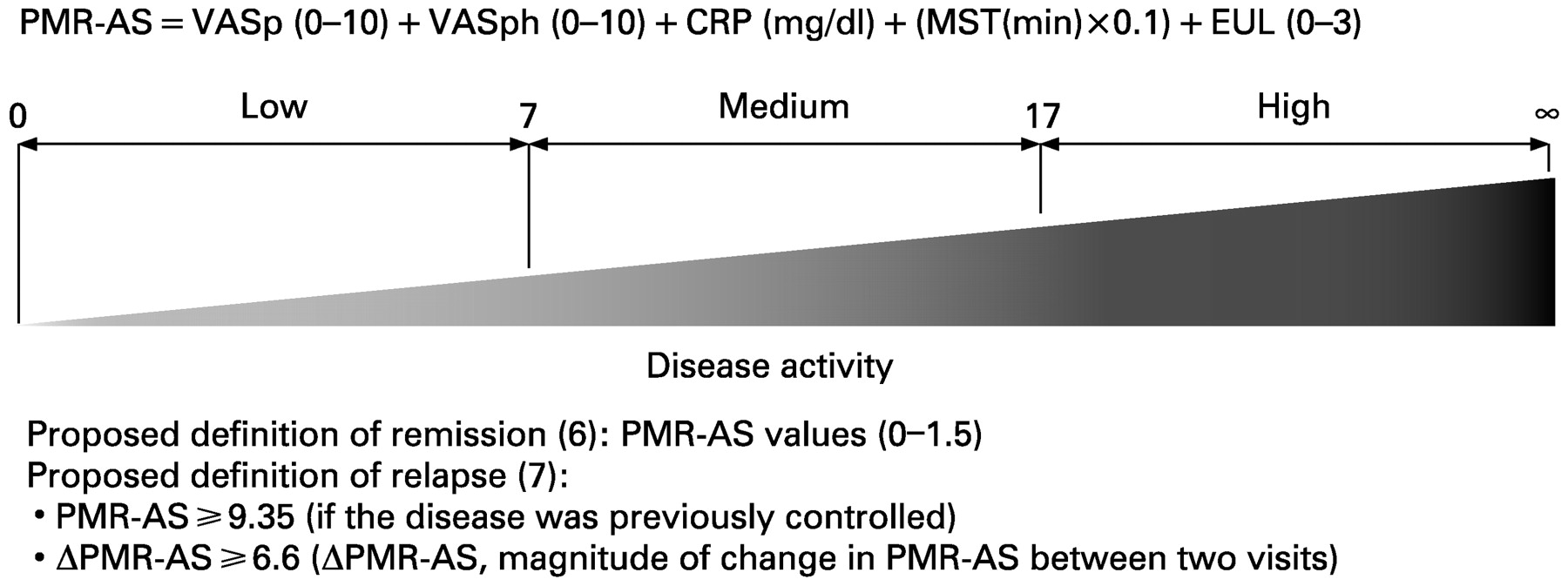
The polymyalgia rheumatica activity score (PMR-AS) in everyday practice. CRP, serum C-reactive protein level; EUL, elevation of upper limbs; MST, morning stiffness duration; VASp, pain severity on a 0–10 visual analogue scale; VASph, physician’s global assessment on a 0–10 visual analogue scale.
In an earlier study8 based on a previously established methodology,10 11 we asked a panel of rheumatologists to assess nine fictional scenarios, with the goal of assessing the impact of VASph interobserver variability on PMR-AS values and the effectiveness of the PMR-AS in predicting glucocorticoid dosage changes and relapse diagnosis. For seven of the nine clinical vignettes, at least 80% of the rheumatologists agreed on a diagnosis of relapse or no relapse. Furthermore, despite interobserver variability in VASph scores, a PMR-AS value greater than 7 was 98.1% sensitive and 94.3% specific for a diagnosis of relapse requiring a glucocorticoid dosage increase.
The objective of this study was to evaluate the feasibility and validity of PMR-AS determination by GPs. More specifically, we sought to determine whether VASph scores determined by GPs were equivalent to those determined by rheumatologists. We also evaluated whether the PMR-AS score computed using the GP-assessed VASph correlated with a diagnosis of relapse or no relapse by the rheumatologists, which served as the reference standard. To this end, we used the seven clinical vignettes that generated strong agreement among rheumatologists about a diagnosis of relapse or no relapse in our previous study.8 These vignettes were evaluated by 163 GPs.
METHODS
Clinical vignettes
Nine clinical vignettes (table 1) describing fictional patients with PMR were written by a panel of rheumatologist experts who were members of the Inflammatory Joint Disease Working Group of the French Society for Rheumatology (Club “Rhumatismes et Inflammation”). The vignettes spanned the full spectrum of disease-activity levels. They shared common features: a definitive diagnosis of PMR; initial symptoms consisting of asthenia, anorexia, weight loss, limited active range of motion of the shoulders and aching and morning stiffness in the neck and limb girdles; elevated ESR and CRP; a rapid response to prednisone therapy, with complete resolution of clinical symptoms and normal ESR and CRP; and initial prednisone therapy in a dosage of 0.3 mg/kg per day for 15 days and 0.25 mg/kg per day for the next 15 days, then 0.2 mg/kg per day followed by tapering every week or 2 weeks for approximately 6 months. The recurrence of clinical symptoms or ESR or CRP elevation was described in the vignettes as suggestive of a relapse.
Reference standard for the diagnosis of relapse
In a previous study,8 the nine vignettes were submitted to 35 office and hospital-based rheumatologists who were asked to decide whether the disease was relapsing. For the present study, we used the vignettes for which at least 28 (80%) rheumatologists agreed that the disease was or was not relapsing, in keeping with the methodology used in previous studies based on questionnaires or clinical vignettes.10 11 Seven of the nine vignettes met this criterion. (For the remaining two vignettes, 43% and 60% of the rheumatologists, respectively, felt that there was no relapse.)
Study design
The seven vignettes were submitted to 163 GPs, who were asked to determine the VASph score and to decide whether the disease was relapsing and whether a prednisone dosage increase was in order. The GPs also completed a questionnaire designed to evaluate their experience with managing PMR patients (based on the number of patients followed up for PMR over the past year) and their opinions about the need for rheumatologist visits for the diagnosis of PMR and/or the follow-up of PMR patients, most notably in the event of glucocorticoid dependency or side effects. Data on relapse diagnosis were obtained for 1116 vignette–GP combinations (158 for vignettes 1 and 4; 159 for vignette 2; 160 for vignettes 3, 5 and 7; and 161 for vignette 6). Among them, the GPs’ opinions about the glucocorticoid dosage were available for 1106 combinations, 1100 had VASph values assessed by the GPs. The PMR-AS was computed for these 1100 combinations with complete data and its performance for relapse diagnosis was evaluated.
Statistical analysis
Results for the quantitative variable VASph are reported as the means (SD) and those for the qualitative variables (diagnosis of relapse and decision to increase the prednisone dosage) as percentages and as number of “yes” answers for each vignette.
We computed the PMR-AS as indicated by Leeb and Bird:5 PMR-AS = CRP (mg/dl) + VASp (0–10) + VASph (0–10) + (MST(min) × 0.1) + EUL (0–3). The four levels on the semiquantitative EUL scale are as follows: 3, no upper limb elevation; 2, elevation below the shoulder girdle (<90°); 1, elevation up to the shoulder girdle (90°); and 0, elevation above the shoulder girdle (>90°) (fig 1). Patient groups were compared using the χ2 test for qualitative variables and the Mann–Whitney U test for quantitative variables. p Values smaller than 0.05 were considered statistically significant.
We studied the associations linking a diagnosis of relapse by the panel of rheumatologists (the reference standard) with the values of the PMR-AS based on the GP-assessed VASph and with each of its five components (MST, EUL, GP-assessed VASph, VASp and CRP). Receiver-operating characteristic (ROC) curves were plotted. Sensitivities and specificities were calculated at different cut-off values. The optimal cut-off for a variable was defined as the value nearest the northwest point of the ROC curve. When two similar cut-off values were found, the one with the best sensitivity was chosen. Statistical tests were performed using the statistical package for the social sciences (version 13.0).
RESULTS
Experience and opinions of GPs regarding the management of PMR
The mean number of patients with PMR followed in 2006 was 2.52 (SD 2.48) (0–20) per GP. Only 35.8% (57/159) of the GPs routinely referred patients to a rheumatologist to confirm the diagnosis and only 19.9% (32/161) felt that routine follow-up by a rheumatologist was required. Conversely, in the event of a relapse or glucocorticoid dependency, 41.3% (66/160) and 63.1% (101/160) of GPs, respectively, felt that prompt rheumatologist referral was appropriate. Side effects of glucocorticoid therapy were felt to indicate a need for rheumatologist referral by only 31% (49/158) of the GPs. Finally, 41.7% (58/139) of the GPs reported that some of their patients with PMR had no rheumatologist visits throughout the course of their disease (from diagnosis to full recovery).
Agreement between relapse diagnosis by GPs and by rheumatologists
Relapse diagnosis by GPs correlated closely with relapse diagnosis by rheumatologists, which was used as the reference standard. Agreement was 90.3% (95% CI 88.4% to 91.9%) with κ = 0.80. Of the 504 relapse diagnoses made by GPs, 67 (13.3%) cases had no relapse diagnosis by rheumatologists, and of 612 diagnoses of non-relapsing disease made by GPs, 41 (6.7%) had a relapse diagnosis by rheumatologists.
Diagnosis of relapse and decision to increase prednisone
As expected, we found a significant (p<0.001) association between diagnosing a relapse and deciding to increase the prednisone dosage, with an agreement of 95.1% (95% CI 93.6% to 96.3%). Of 1106 vignette–GP combinations, 1052 were concordant for the GP diagnosis of relapse and the decision to increase prednisone, including 416 assigned to both the “relapse” group and the “increase prednisone dosage” group and 576 to both the “no relapse” group and the “do not increase prednisone dosage” group. Thirty-two patients assigned to the “no relapse” group were assigned to the “increase prednisone dosage” group and the opposite occurred for 22 patients.
Diagnostic impact of clinical and laboratory parameters
As expected, interobserver variability was noted in physicians’ assessments of disease activity (the VASph component of the PMR-AS). The mean (SD) and ranges for GP-determined VASph scores for vignettes 1 to 7 were 1.95 (SD 1.40) (0–10), 1.66 (SD 1.00) (0–6), 3.88 (SD 1.65) (1–10), 4.48 (SD 1.88) (0–10), 2.03 (SD 1.17) (0–8), 1.81 (SD 1.22) (0–8) and 4.23 (SD 1.87) (0–10), respectively (fig 2). Nevertheless, no significant difference was found between GP and rheumatologist VASph scores (table 1).

Box-and-whisker plots of global assessments (physician’s global assessment on a 0–10 visual analogue scale; VASph) by general practitioners (GPs) for each of the seven vignettes. VASph was evaluated on a 0–10 visual analogue scale.
Figure 3 shows the ROC curves of associations linking relapse diagnosis by the rheumatologists (the reference standard) to the PMR-AS and each of its components (MST, EUL, GP-assessed VASph, VASp and CRP) for the seven vignettes used in the study. Table 2 shows the best cut-off values for the better-performing parameters, together with their sensitivities and specificities. MST longer than 10 minutes was 100% sensitive and 100% specific. Relapse diagnosis was strongly associated with a PMR-AS of 7 or greater, which was 99.4% sensitive and 93.3% specific. Performance was somewhat lower for VASph of 2.5 or greater (88.5% sensitive and 78.9% specific) and CRP of 14.5 mg/l or greater (66.5% sensitive and 100% specific). EUL and VASp showed weaker associations with relapse diagnosis (VASp ⩾1.5, 100% sensitive and 59.1 specific; EUL ⩾1, 66.5% sensitive and 75.0% specific).

{kind=link}
{kind=link}
{kind=link}
Receiver-operating characteristic curves of associations linking relapse diagnosis to the polymyalgia rheumatica activity score (PMR-AS) and each of its components (morning stiffness (MST), ability to elevate upper limbs (EUL), global assessment by general practitioners (VASph), visual analogue scale for pain (VASp) and C-reactive protein (CRP) level).
Agreement between relapse diagnosis by rheumatologists and relapse diagnosis defined as GP-based PMR-AS of 7 or greater
PMR-AS values correlated closely with relapse diagnosis: agreement was 95.9% (95% CI 94.5% to 97.0%) for κ = 0.92. Of the 590 combinations with PMR-AS values lower than 7, all but three (0.5%) had no relapse diagnosis. Of 510 combinations with PMR-AS values greater than or equal to 7 (8%), 42 had no flare diagnosis.
DISCUSSION
The PMR-AS, which was developed based on the European League Against Rheumatism (EULAR) response criteria for PMR defined by the European Collaborating Polymyalgia Rheumatica Group,12 is a composite index that appears well suited to everyday practice and useful for tailoring glucocorticoid dosages to the changing needs of individual patients over time, thereby limiting unnecessary exposure to both glucocorticoids and inflammation. Reports of proposed PMR-AS thresholds for defining remission and relapse6 7 may further increase the usefulness of the score in determining when disease control is adequate and when the glucocorticoid dosage should be increased or decreased.
We found excellent agreement (90.3%) between relapse diagnosis by GPs and relapse diagnosis by rheumatologists, as well as between relapse diagnosis by GPs and a decision by GPs to increase the glucocorticoid dosage (95.1% of agreement). Our results on the contribution of GPs to the management of patients with PMR in Brittany, France, are consistent with those obtained in Minnesota, USA;9 thus less than 40% of GPs routinely referred their patients to the rheumatologist to confirm the diagnosis or to assist in monitoring the treatment. The main reasons for rheumatologist referrals were atypical PMR with glucocorticoid dependency and difficulty in ruling out differentials such as late-onset rheumatoid arthritis and chondrocalcinosis.
The physician’s overall assessment of disease activity on a subjective VAS (VASph) varied widely among the 163 GPs for a given vignette (table 1). Nevertheless, for none of the vignettes was a significant difference found between the mean VASph values determined by the GPs and by the rheumatologists. Moreover, PMR-AS values computed using GP-assessed VASph scores were highly sensitive and specific for a relapse diagnosis by rheumatologists (our reference standard). The best cut-off was also 7 points in our previous study using the same vignettes evaluated by rheumatologists.8 Therefore, as reported previously, a global estimate by the physician should not be the sole basis for making treatment decisions.8
The PMR-AS determined by GPs is a valid tool that would probably help GPs monitor and adjust glucocorticoid regimens in patients with PMR. Both the shortage of rheumatologists and the predominant contribution of GPs to the management of PMR patients lend considerable importance to these findings. Of 590 GP–vignette combinations with PMR-AS values lower than 7, all but three had no relapse diagnosis. However, of 510 combinations with PMR-AS values of 7 or more, 42 had no relapse diagnosis. Therefore, referral to a rheumatologist appears unnecessary when the PMR-AS value does not indicate a relapse but may be in order to confirm a relapse when the PMR-AS suggested disease flare. Nevertheless, the percentage of patients managed by GPs or rheumatologists differs from one country to another and propositions for the referral of patients to rheumatologists should be made in this respect.
Our study has several limitations. First, although the vignettes were written by rheumatologists who had extensive experience with PMR, and the use of clinical vignettes was validated previously,8 11 13 they did not describe real patients. Indeed, the VASph scores assessed by GPs in this study, and compared with specialists’ scores, were based on hard data only instead of seeing and assessing real patients, in which the subjective impression and experience is very important and may influence physicians’ judgement of VASph parameters. This fact supports the necessity to complete the validation of the PMR-AS used by GPs in real life, all the more in that the number of patients managed by GPs is quite low, to know whether PMR patients could be well managed by GPs and do not need further specialist referral. Second, changes in the parameters from one visit to the next were small, except for MST. This may explain partly why MST was the best variable for diagnosing a relapse. Indeed, in our experience medical practitioners mainly rely on girdle pain and inflammatory markers rather than on MST to assess disease activity and diagnose a relapse. MST appears less important than the other parameters for appreciating disease activity. Moreover, early MST shorter than 30 minutes could not discriminate relapses from stable disease in real cases and short-lived MST is not relevant. The diagnosis value and the cut-off of 10 minutes found for MST is likely to be an artefact due to the way the vignettes were designed. A set of vignettes describing larger variations in other parameters might produce slightly different results from those reported here.
The aim of this study was not to define a PRM-AS cut-off indicating a relapse, which was done previously in a prospective study,7 but to establish that the PMR-AS remains valid when used by GPs, ie, performs as well for diagnosing a relapse when used by GPs as when used by rheumatologists. The external validation of relapse diagnosis by rheumatologists obtained from our study of GP-assessed VASph values strongly supports the usefulness of the PMR-AS in primary care practice. Nevertheless, the agreement between rheumatologists and GPs could be lower in untypical cases of PMR and it is unclear how well the scoring system would perform in a situation characterised by pitting oedema or by synovitis as the only manifestations of relapse. It is probably a weakness of the scoring system.
To establish definitively the usefulness of the PMR-AS for managing glucocorticoid tapering by GPs in patients with PMR, a prospective cohort study with the relapse rate and total glucocorticoid dosage as the main evaluation criteria is needed. The PMR-AS may be a useful reference standard in future clinical trials to ensure uniformity across study centres or physicians and is simple enough to be used on an everyday basis by GPs.
REFERENCES
Footnotes
Competing interests: None.
Contributors: Study design: AB, MDB, AS. Acquisition of data: BL, AB, MDB, J-MB, AS. Analysis and interpretation of data: AB, BL, AS. Manuscript preparation: AB, BL, MDB, J-MB, AS. Statistical analysis: AB, BL, AS. Club “Rhumatismes et Inflammation”: Inflammatory Joint Disease Working Group of the French Society for Rheumatology.