Article Text

Abstract
Objectives: Ankylosing spondylitis (AS) is associated with increased cardiovascular morbidity and mortality. Microvascular function has been linked to several risk factors for cardiovascular disease. Inflammation in AS may cause microvascular dysfunction. To test this, we assessed microvascular function in (a) patients with AS compared to healthy controls and (b) patients with AS before and after 1 month of anti-tumour necrosis factor (TNF)α treatment with etanercept.
Methods: A total of 15 consecutive patients with AS, who were scheduled for etanercept treatment according to the Assessment in Ankylosing Spondylitis (ASAS) group guidelines, and 12 healthy controls matched for age and sex, were recruited. Endothelium-dependent and independent vasodilatation in skin were evaluated with laser Doppler fluxmetry after iontophoresis of acetylcholine and sodium nitroprusside, respectively. Videomicroscopy was used to measure recruitment of skin capillaries after arterial occlusion.
Results: Compared to healthy controls, patients with AS had impaired endothelium-dependent vasodilatation and capillary recruitment. Following anti-TNFα treatment, microvascular function improved significantly for endothelium-dependent vasodilatation (p = 0.03) and capillary recruitment (p = 0.006). A significant correlation was observed between changes in endothelium-dependent vasodilatation and changes in erythrocyte sedimentation rate (ESR) (r = −0.56; p = 0.03).
Conclusion: Microvascular dysfunction is present in patients with AS with active disease, but improves as inflammation regresses after TNFα blockade.
Statistics from Altmetric.com
Ankylosing spondylitis (AS) is a chronic inflammatory disease of the sacroiliac joints and spine affecting up to 1% of the population.1 Patients with AS have an approximately twofold increased death rate compared to the general population, which is predominately caused by increased cardiovascular (CV) risk.2–4 Although specific cardiovascular disorders (valvular disease and conduction disturbances) occur more frequently in AS,4 5 accelerated atherosclerotic disease probably contributes to the increased CV risk as well.6 7 Accelerated atherosclerosis in AS may partly be due to traditional CV risk factors (ie, an atherogenic lipid profile and hypertension).8 9 In addition, the generalised inflammatory state that characterises active AS renders these patients more prone to develop cardiovascular, atherosclerotic, disease (CVD), as many parallels exist between the inflammatory mechanisms in the pathogenesis of atherosclerosis and in the pathogenesis of autoimmune diseases.10 Therefore, AS could be an independent cardiovascular risk factor.6 7 The association between inflammation and atherogenesis is most extensively described for rheumatoid arthritis (RA) and systemic lupus erythaematosus11–14 but appears to apply to AS as well.6 7
Analogous to RA,15 inflammation in AS may cause (microvascular) endothelial dysfunction. Endothelial dysfunction precedes and initiates atherosclerosis and is a predictor of long-term cardiovascular risk.16 A pivotal proinflammatory cytokine is tumour necrosis factor α (TNFα). Circulating TNFα levels are increased in patients with AS and important in the pathogenesis of AS.17 18 Increased TNFα levels may have an important role in the pathogenesis of endothelial dysfunction in inflammatory diseases.19–21
A particularly interesting type of vascular dysfunction occurs in the microvasculature. Microvascular dysfunction is closely, and presumably causally, linked to CV risk factors, particularly insulin resistance and hypertension.22 23 Preliminary evidence suggests that inflammation may also cause dysfunction of the microvasculature. Impaired coronary microvascular function was recently found in patients with AS, and correlated well with serum C-reactive protein (CRP) and TNFα levels.19 Interestingly, circulating levels of CRP and TNFα are associated with skin microvascular dysfunction even in normal subjects.24 25
Considering this, we hypothesised that patients with active AS have impaired microvascular function. In addition, we anticipate that blocking TNFα in these patients not only reduces disease activity,26–29 but also improves microvascular function. To test this, we assessed capillary density and recruitment as well as endothelium-(in)dependent vasodilatation of skin microcirculation in (a) patients with AS compared to healthy controls and (b) patients with AS before and after 1 month of anti-TNFα treatment with etanercept.
PATIENTS AND METHODS
Subjects
A total of 15 consecutive patients with AS (10 males), scheduled for etanercept treatment according to the Assessment in Ankylosing Spondylitis (ASAS) group guidelines for anti-TNFα treatment30 were studied. All patients fulfilled the modified New York diagnostic criteria of AS31 and were recruited from the Jan van Breemen Institute and VU University Medical Center and treated with twice weekly 25 mg etanercept subcutaneously. Exclusion criteria were (self-reported) diabetes mellitus, Raynaud phenomenon, thyroid dysfunction, previous cardiovascular events, hypertension (systolic blood pressure >140 mmHg and/or diastolic blood pressure >90 mmHg) or the use of antihypertensive agents. A total of 12 age-matched and sex-matched healthy volunteers (8 males) served as controls. One patient and one control subject used a statin. No alterations in (concomitant) medication use, including non-steroidal anti-inflammatory drugs (NSAIDs), which all patients used, were allowed during the treatment period. All participants gave written informed consent and the study protocol was approved by the Institutional Ethics Committee of both hospitals.
Study design
Microvascular measurements were conducted in a quiet, temperature-controlled room (T = 23.4±0.4°C) after 20–30 min of acclimatisation, with the subjects in the sitting position and the investigated, non-dominant hand at heart level. Nailfold capillary studies and iontophoresis studies were performed on the same day. Subjects were asked to refrain from beverages other than water (especially no caffeine or alcohol), smoking, medication, except paracetamol if necessary, and meals from midnight on the testing day. During the tests, skin temperature was monitored and all subjects were studied between 8.00 am and 12.00 am.
Nailfold capillaries in the dorsal skin of the third finger were visualised by a capillary microscope (Nikon, Amstelveen, The Netherlands), linked to a television camera (Philips LDH 0702/20; Eindhoven, The Netherlands), a video recorder (Panasonic NV-HS930, S-VHS; 's-Hertogenbosch, The Netherlands) and a monitor (Sony SSM-125CE; Badhoevedorp, The Netherlands).32 Incident illumination was achieved by light from a 100-W vapour mercury lamp (which passes through a heat-absorption and heat-reflection filter), a polariser and a 50% mirror to illuminate the object. To visualise the capillaries, a 5× objective (Nikon 5/0.13) was used with a total system magnification of 115×. Nailfold capillaries in finger skin were recorded on videotape before and after 4 min of arterial occlusion with a digital cuff. This procedure was performed twice, and the mean of both measurements was used for analyses. Counting was performed using monitor (Sony PVM-1443MD) and video recorder (Sony S-VO-9500MDP). Capillaries were counted by a single observer using the naked eye from a freeze-framed reproduction of the videotape, and from the running videotape when it was uncertain whether a capillary was present or not. We estimated baseline capillary density by counting the number of continuously erythrocyte-perfused capillaries during a 15-s period. Other capillaries can be seen to be intermittently perfused, and these may represent an important functional reserve. We used postocclusive reactive hyperemia to estimate this functional reserve. Postocclusive capillary recruitment was calculated by dividing the increase in density by the baseline density. The day-to-day coefficient of variation (CoV) of the capillary density in resting state was 2.3 (1.8)%. The CoV of the percentage capillary recruitment and absolute capillary recruitment during postocclusive hyperaemia were 8.3 (4.9)% and 6.2 (4.3)%, respectively.
Endothelium-(in)dependent vasodilatation of finger skin microcirculation was evaluated by iontophoresis of acetylcholine (ACh) and sodium nitroprusside in combination with laser Doppler fluxmetry as previously described in more detail.22 33 Laser Doppler fluxmetry measures microvascular perfusion, the product of red blood cell velocity and concentration.34 A protocol of multiple fixed doses (current intensity × delivery time) was employed resulting in an incremental dose-response curve. Acetylcholine (1%, Miochol-E, Théa Pharma NV, Zoetemeer, The Netherlands) was delivered with an anodal current; seven doses (0.1 mA for 20 s) were delivered, with a 60-s interval between each dose. A 60-s interval between each iontophoresis period was required to achieve the plateau of the response following each delivery of acetylcholine.35 Sodium nitroprusside (0.01%, VU University Medical Center (VUmc)) was delivered with a cathodal current; nine doses (0.2 mA for 20 s) were delivered, with a 90-s interval between each dose. A 90-s interval between each iontophoresis period was required to achieve the plateau of the response after each delivery of sodium nitroprusside.35 Acetylcholine-dependent laser Doppler flux was measured on the middle phalanx of the third finger, whereas nitroprusside-dependent laser Doppler flux was measured at the same spot on the opposite hand, with approximately 15 min elapsed between the two measurements. The day-to-day CoV of the percentage increase from baseline to the final 2 min of the plateau phase was 9.8 (5.6)% for acetylcholine and 8.3 (5.4)% for sodium nitroprusside.
Statistical analyses
Data are expressed as mean (SD) or median (interquartile range) as appropriate. The distribution of variables was tested for normality and transformed if necessary. Variables were tested (a) unpaired for comparing patients and controls and (b) paired for comparing the patients with AS at baseline and at 1 month. The Student t test was used to compare continuous normally distributed variables. We used non-parametric tests (Wilcoxon signed-rank test or Mann–Whitney U test) when appropriate. Linear regression analysis was used to investigate confounding by body mass index (BMI; as calculated using the formula weight (kg)/length (m)2×100). A two-tailed probability value of p<0.05 was considered statistically significant. Correlations between variables were analysed by using Pearson correlation or Spearman rho tests when appropriate.
RESULTS
Characteristics
Baseline characteristics of patients and controls are shown in tables 1 and 2. Age, sex, blood pressure and smoking status were similar in both groups. BMI was higher in patients compared to controls, 26.9 (24.2–28.4) vs 23.2 (22.2–24.9) respectively (p = 0.06). Within patients, BMI and blood pressure remained stable between the two time points. During treatment, CRP and erythrocyte sedimentation rate (ESR) levels, as well as Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) decreased significantly.
Microvascular function is disturbed in AS
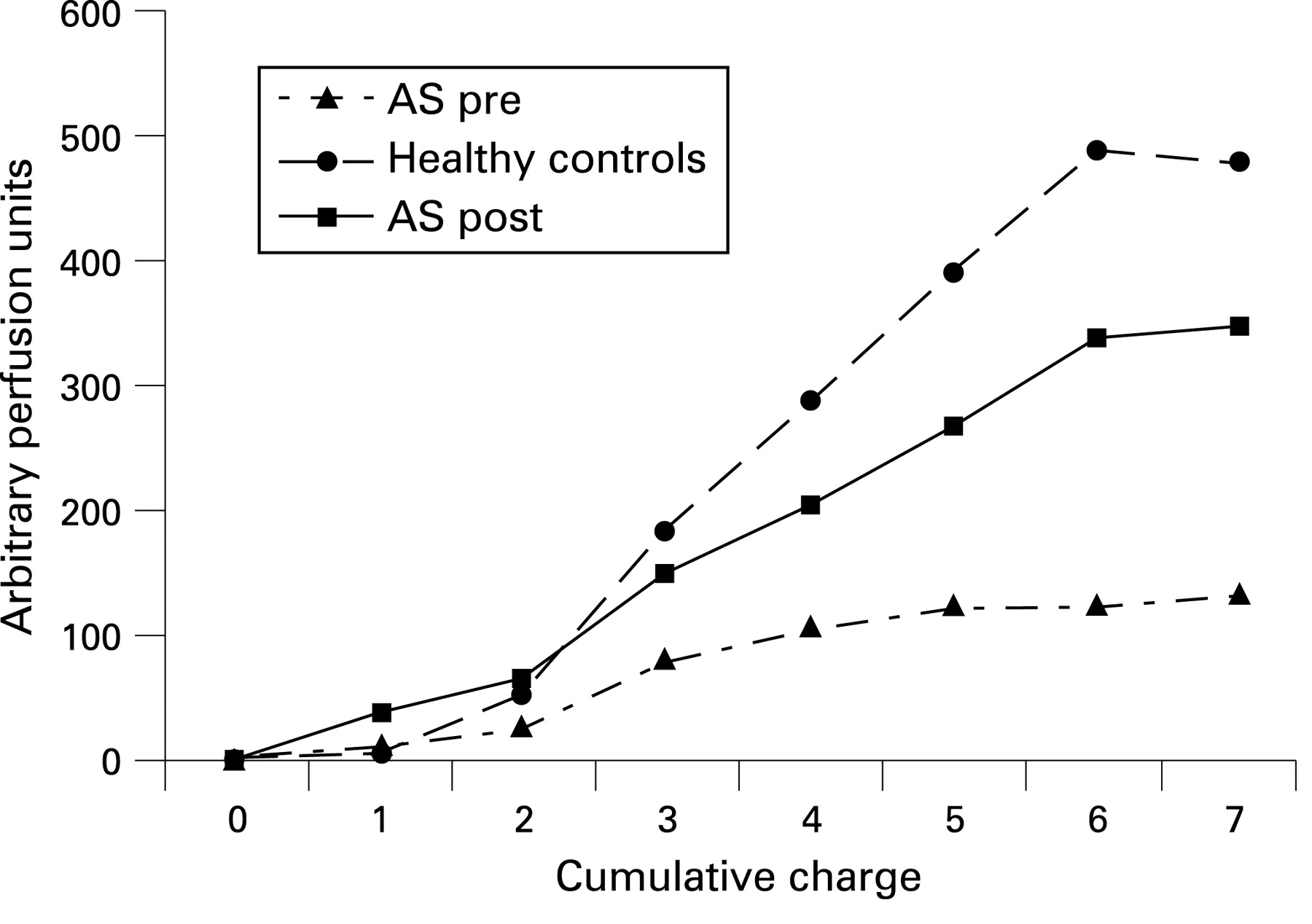
At baseline, patients with AS showed a markedly lower vasodilatation in response to acetylcholine compared to controls (118% vs 469%, respectively, p = 0.02; table 3 and fig 1). The response to sodium nitroprusside did not differ significantly between patients at baseline and 1 month and controls.
Baseline capillary density did not differ between groups. However, absolute and relative postischaemic capillary recruitment were lower in AS at baseline compared to controls (14.8 vs 19.5, respectively for absolute increase, p = 0.04 and 29.6% vs 39.2%, respectively for relative increase, p = 0.01). These results remained after separately adjusting for the difference in BMI and the difference in smoking status between the two groups (data not shown).
Etanercept improves microvascular dysfunction
After 1 month of treatment with etanercept, endothelium-dependent vasodilatation improved significantly in the patients with AS (from 118% to 318%, p = 0.03; table 3 and fig 1) and approached values observed in the healthy controls (p = 0.5). Capillary recruitment improved significantly in patients with AS during treatment (from 29.6% to 38.9%, p = 0.006; table 3) to a level comparable to controls (38.9% vs 39.2%, respectively, p = 1.0).
Etanercept-induced changes in endothelium-dependent vasodilatation correlated inversely with changes in ESR levels (r = −0.56 p = 0.03, fig 2). We did not find any significant correlations between pretreatment and post-treatment differences in endothelium-dependent vasodilatation relative to CRP (r = −0.24 p = 0.4, fig 2) or BASDAI (r = −0.16 p = 0.6). Changes in capillary recruitment (percentage) were not significantly correlated with changes in ESR, CRP or BASDAI (r = −0.15 p = 0.6, r = 0.014 p = 1.0, r = 0.50 p = 0.06 respectively), although there was a trend for BASDAI.

{kind=link}
{kind=link}
DISCUSSION
The present study demonstrates that patients with active AS have impaired microvascular endothelium-dependent vasodilatation and capillary recruitment in skin, which improves after TNFα-blocking therapy with etanercept.
Recent advances have highlighted the crucial involvement of the microcirculation in many cardiovascular conditions, not only in the development of target organ damage in the heart and kidney, but also in the development of cardiovascular risk factors such as hypertension and insulin resistance.23 36 37 Impaired microvascular endothelium-dependent vasodilatation and capillary recruitment, as measured in the present study, have been linked to several conditions associated with CVD, such as hypertension, insulin resistance and (visceral) obesity.22 23 25 33 Furthermore, impaired endothelium-dependent vasodilatation and capillary recruitment can be detected in individuals at increased coronary heart disease (CHD) risk according to the Framingham Heart Study risk score.38 The cutaneous microcirculation is a representative vascular bed to examine the mechanisms of microvascular dysfunction, which may mirror generalised systemic vascular dysfunction in magnitude and underlying mechanisms.39
The finding of impaired microvascular function in patients with AS is concordant with a previous study demonstrating impaired coronary microvascular function in patients with AS without any overt cardiovascular disease.19 Interestingly, in the latter study, impaired coronary microvascular function correlated well with CRP and TNFα levels, suggesting a detrimental effect of inflammation on the microcirculation.19 Our findings support this hypothesis by showing, for the first time, that blocking TNFα with etanercept, results in improvement of microvascular endothelium-dependent vasodilatation and even a normalisation of capillary recruitment in patients with AS compared to healthy controls. In patients with RA, the ability of TNFα-blocking therapies to improve endothelial function has already been demonstrated, predominately at the macrovascular level, as measured by brachial artery ultrasonography20 21 or plethysmography.40 Again, in patients with RA, a case of diffusely impaired myocardial perfusion in the absence of any significant coronary atheroma in active systemic RA was described, which improved following intensive immunosuppression.41 Moreover, impaired endothelium-dependent vasodilatation has been shown at the microvascular level during active disease (“flare”), which improved after inflammatory suppression with disease-modifying antirheumatic drugs (DMARDs) or TNFα-blocking therapy.42
In this regard, the observation of a lower incidence of first cardiovascular events in patients with RA treated with TNFα-blocking therapy43 is interesting, as improvement of microvascular function after TNFα blockade may play a causative role.
There is evidence that TNFα contributes to microvascular dysfunction. TNFα levels negatively correlate with skin capillary recruitment even in healthy individuals24 25 and increased production of TNFα is associated with obesity-related insulin resistance, as well as obesity-related hypertension.25 44 A possible mechanism involved in these microvascular disturbances is impaired activation of endothelial nitric oxide synthase (eNOS). TNFα blocks the activation of eNOS, by interfering with Akt phosphorylation, which is essential for flow-dependent and ACh-dependent vasodilatation.45 In addition, TNFα directly degrades eNOS mRNA.46 47
In addition to specific TNFα effects on microvasculature, it is conceivable that, in line with inflammatory driven atherogenesis, improvement of microvascular function was the result of a generally decreased inflammatory “burden”. Indeed, ESR and CRP levels, as markers of inflammation, declined significantly during treatment. In this regard, in 50 patients with psoriatic arthritis (another inflammatory disease included within the group of spondyloarthropathies) without clinically evident cardiovascular disease, a significant correlation between CRP level and ESR at the time of disease diagnosis and flow-mediated endothelial dependent vasodilatation was observed.48 Correlation analyses revealed a significant correlation for pretreatment and post-treatment ESR levels and endothelium-dependent vasodilatation, but not for CRP. The absence of a significant correlation between changes in CRP and vascular function was also reported in previous studies on vascular function in RA and AS.42 49 In our study, this may be due to small patient numbers or indicate that, in addition to inflammatory suppression, TNFα specific features determining endothelial function, are important. The latter is supported by a study showing improvement of endothelial function in patients with RA after intravascular administration of a TNFα-blocking agent, without concurrently affecting circulating CRP levels.50 It is likely both mechanisms (ie, general dampening of inflammation and (other) TNFα specific effects) intertwine. The present study design, however, is not suited to clearly differentiate between these mechanisms.
In conclusion, we showed that patients with active AS have vascular dysfunction at the microcirculatory level. This finding supports the idea that AS represents a CHD risk factor. TNFα-blocking therapy with etanercept improved microvascular function. Further research in larger patient groups should elucidate if this effect translates into a decrease in cardiovascular morbidity and mortality in patients with AS.
REFERENCES
Footnotes
Competing interests: None declared.
Ethics approval: All participants gave written informed consent and the study protocol was approved by the Institutional Ethics Committee of both hospitals.