Article Text

Abstract
Objective: To explore the monetary value of rheumatoid arthritis related loss of productivity in patients with early active disease.
Methods: In a prospective cohort substudy of the FIN-RACo Trial, 162 patients with recent onset rheumatoid arthritis, aged 18 to 65 years and available to the workforce, were followed up for five years. Loss of work productivity in euros 2002 was estimated by data on absence for sickness and on income (human capital approach) from official databases. Treatment responses were evaluated by area under the curve (AUC) of the ACR-N measure and by increase in number of erosions in radiographs of hands and feet. The health assessment questionnaire (HAQ) at six months was linked to the International Classification of Functioning, Disability and Health (ICF).
Results: In all, 120 (75%) patients, women more often (82%) than men (61%) (p = 0.002), lost work days. The mean lost productivity per patient-year was €7217 (95% confidence interval (CI), 5561 to 9148): for women, €6477 (4858 to 8536) and for men, €8443 (5389 to 12 898). There was an inverse correlation with improvement: €1101 (323 to 2156) and €14 952 (10 662 to 19 852) for the highest and lowest quartiles of AUC of ARC-N, respectively. Lost productivity was associated with increase in the number of erosions and with disability in “changing and maintaining body position” subcategory of the ICF.
Conclusions: Despite remission targeted treatment with disease modifying antirheumatic drugs, early rheumatoid arthritis results in substantial loss of productivity. A good improvement in the disease reduces the loss markedly.
- ACR, American College of Rheumatology
- AUC, area under the curve
- DMARD, disease modifying antirheumatic drug
- FCA, friction cost approach
- FIN-RACo, Finnish Rheumatoid Arthritis Combination-Therapy Trial
- HCA, human capital approach
- HAQ, Health Assessment Questionnaire
- ICF, International Classification of Functioning, Disability and Health
- rheumatoid arthritis
- lost productivity
- work disability
- human capital approach
- ICF
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- AUC, area under the curve
- DMARD, disease modifying antirheumatic drug
- FCA, friction cost approach
- FIN-RACo, Finnish Rheumatoid Arthritis Combination-Therapy Trial
- HCA, human capital approach
- HAQ, Health Assessment Questionnaire
- ICF, International Classification of Functioning, Disability and Health
Reduced work capacity and cessation of working life are common consequences of rheumatoid arthritis,1–,3 and work disability has appeared as its most expensive outcome.4–,7 With a few exceptions,4,8,9 estimates of loss of work productivity have included only permanent work disability. However, this reflects only a part of the impact of rheumatoid arthritis on working life. For a comprehensive description of a disease’s impact on human functioning, the WHO has recently developed the International Classification of Functioning, Disability and Health (ICF).10
We have reported the cumulative number of work disability days over a five year follow up of patients with recent onset rheumatoid arthritis, randomised to receive either a single disease modifying antirheumatic drug (DMARD) or a combination of three DMARDs for two years.11 In the present study, we estimate the monetary value of productivity lost by the days off work of the same patients by using official databases documenting days off work, as well as earnings assessed by the tax authorities. Further, we analyse associations of the losses with treatment response and patient’s condition. We link the Stanford Health Assessment Questionnaire (HAQ)12 at six months to ICF components to explore which of them are the best predictors of loss of productivity during the early years of rheumatoid arthritis.
METHODS
The data come from a randomised controlled trial (the Finnish Rheumatoid Arthritis Combination-Therapy Trial, FIN-RACo) comparing treatment with a combination of sulfasalazine, methotrexate, and hydroxychloroquine with that of a single DMARD (initially sulfasalazine) in the treatment of patients with recent onset, clinically active rheumatoid arthritis (for details see Möttönen et al13 and Korpela et al14). This substudy includes the 162 patients less than 65 of age who at baseline were gainfully employed or at least available for work (fig 1⇓). The study group has been described earlier.11
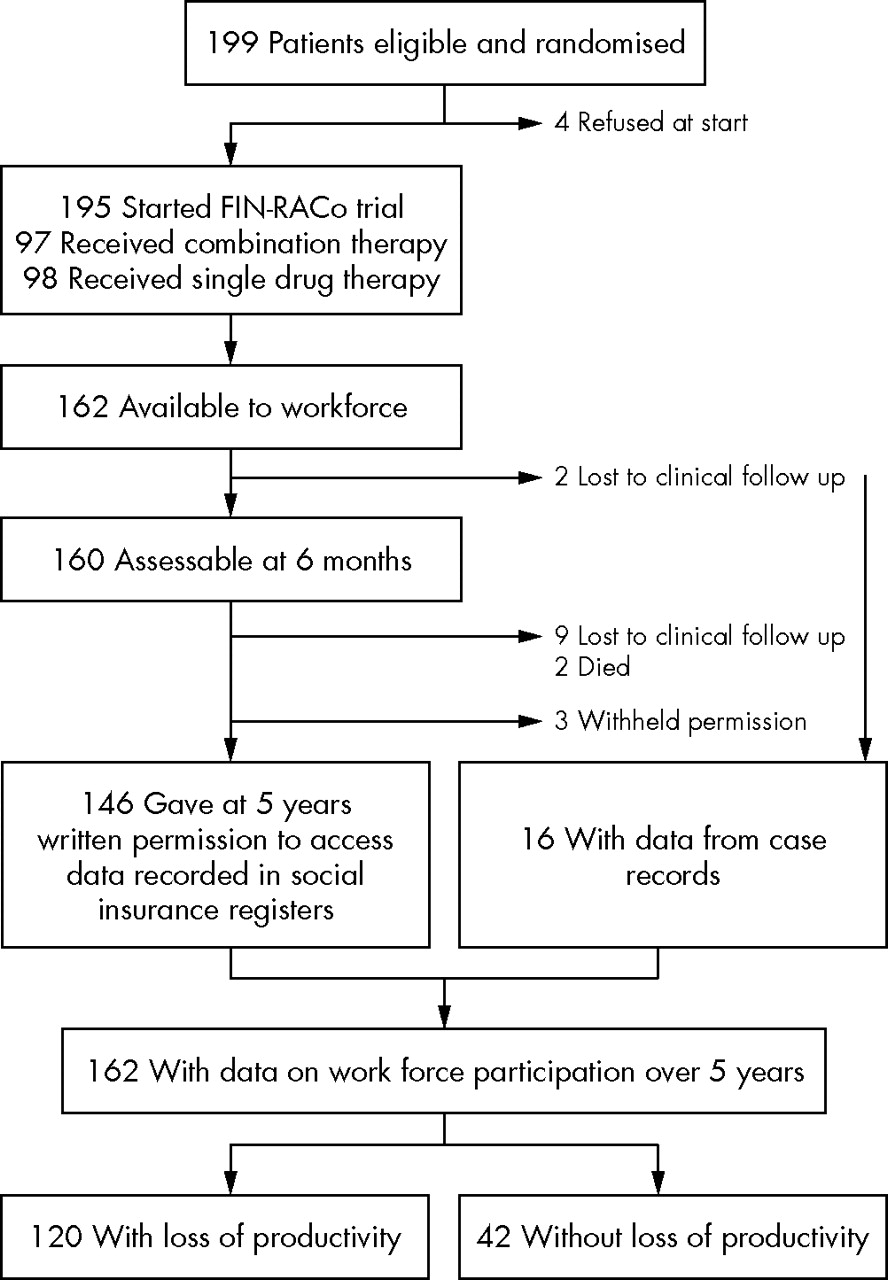
Study flow.
Measures
Patients were assessed at baseline and at regular doctor visits for five years or until lost to follow up. The overall treatment response of each patient (American College of Rheumatology ACR-N15) was determined by the smallest degree of improvement in percentage terms from baseline in three criteria: the number of tender joints, the number of swollen joints, and the median of five other measures (patient’s and physician’s global assessment of rheumatoid arthritis severity, patient’s assessment of pain, erythrocyte sedimentation rate, and HAQ). Time weighted area under the curve (AUC) over the five years was calculated. One radiologist blinded for treatment strategy assessed radiographs of the hands and feet.
At the five year visit, the patients were asked for permission to collect data on their sick leave (∼work disability up to one year in Finnish legislation) and work disability periods from the social insurance registers. Thirteen of the patients (8%) were lost to follow up because of death or other reasons, and permission was withheld by three (fig 1⇑). In such patients, on the basis of their written informed consent at baseline, information about work disability was obtained from case records. The principles of the Finnish social insurance system have been described elsewhere.11
Calculation of lost productivity
For each patient, cumulative duration was calculated for periods of sick leave and rheumatoid arthritis related (according to diagnosis code in doctors’ statements) longer work disability periods. The number of work disability days was divided by the duration (in years) of follow up during which the patient had not retired because of other diseases or because of age—that is, was available to the work force. The mean number of days per patient-year was 78 in the combination therapy group and 128 in the single drug group. In all, 40 patients became permanently work disabled because of rheumatoid arthritis. We reported these results earlier.11 The register data included allowances and pensions paid as compensation for lost income. The amount of sickness allowance is calculated on the basis of the preceding year’s earnings assessed by the tax authorities. Thus, income before contracting rheumatoid arthritis can be calculated on the basis of the allowance paid over the first sick leave period by applying the formula backwards. For those patients with only case record data about days off work, the average income from jobs came from Statistics Finland (www.stat.fi).
An employee’s productivity was defined as equalling his or her total costs to an employer (salary plus supplementary social welfare expenses), and a self employed person’s productivity was defined as equalling personal income plus statutory health and pension insurance expenses. These supplementary expenses are enacted yearly as a certain proportion of income, and have ranged 32.2% to 38.0% for wage and salary earners, 11.50% to13.02% for self employed farmers, and 21.80% to 22.55% for other self employed persons. Income after the first year was calculated by the annual indices of each branch of the economy, and supplementary expenses were added in each year; these sums were converted to prices in 2002 by the general index of wages and salaries. The human capital approach16 was applied: for each patient, mean productivity per day was multiplied by the cumulative number of days off work to yield loss of productivity. One patient received rheumatoid arthritis related disability pension for part time (50%) work; her number of days on pension was divided by 2. Without overt connection to rheumatoid arthritis, two patients were working part time at study entry and three other patients at five years. Their reduced working hours were not included in lost productivity.
Linking of items of HAQ to ICF categories
The 20 items of HAQ at six months were linked to activity limitations of the ICF9 (table 1⇓). The linking principles of Cieza et al were applied17 with a two level classification procedure. The HAQ yielded three ICF categories: mobility, self care, and domestic life. “Mobility” was divided into four subcategories: changing and maintaining body position, handling, walking and moving, and moving using transportation. The last two were combined so that each category and subcategory included at least two questions scored from 0 to 3, and the highest score in each (sub)category separately defined each patient’s score.
Questions of the Stanford Health Assessment Questionnaire disability index linked to (sub)categories of the International Classification of Functioning, Disability and Health*
Statistical analyses
Descriptive values of variables are expressed as means with standard deviations and with 95% confidence interval (CI), and as medians with interquartile range (IQR). Confidence intervals for means of lost productivity were obtained by bias corrected and accelerated bootstrapping18 (5000 replications) because the variables were skewed. Statistical comparisons between groups were made by χ2 test, by permutation test, and by analysis of variance (ANOVA) with general score (Monte Carlo p values). The multiple imputation (Markov-chain Monte Carlo) method was used to fill in missing values for individual HAQ questions. A continuation ratio model for ordinal outcomes was used to analyse relations between loss of productivity and restrictions of functioning by the items of HAQ linked in ICF (sub)categories at six months19; the patients were divided according to loss of productivity per patient-year into four groups of almost the same size: 0 (n = 42), €1–1200 (n = 37), €1201–10 000 (n = 42), and over €10 000 (n = 41).
RESULTS
As figs 1⇑ and 2⇓ illustrate, 120 of the 162 patients (101 female, 61 male) used sick leave and experienced work disability which led to lost productivity—women (83; 82%) more often than men (37; 61%) (p = 0.002). For 101 patients (87 employed, 14 self employed) register data yielded personal income before the onset of rheumatoid arthritis. When these calculated incomes were compared with average annual incomes of respective jobs from Statistics Finland, the difference was not statistically significant. Incomes obtained from statistics for the remaining 19 patients can be regarded as valid. The annual productivity for the 120 patients averaged €29 501 (95% CI, 26 854 to 32 148). For comparison, the mean annual income of all gainfully employed and self employed people in Finland in 1993 was €25 055 and in 2000 €25 917, converted to prices in 2002 without supplementary social insurance expenses. The women’s productivity was 80.3% of the men’s productivity which corresponds to the general difference in income between sexes in the Finnish labour market. This in turn results mainly from the different occupational profiles of women and men, both in our study and in general.

Loss of productivity of 162 patients with recent onset rheumatoid arthritis over a five year follow up.
The computed mean (95% CI) loss of productivity was €33 198 (25 563 to 43 104) over the five year follow up (fig 2⇑) and €7217 (5561 to 9148) per patient-year: for women, €6477 (4858 to 8536) and for men, €8443 (5389 to 12 898) (p = 0.26 for sex difference). In the group initially treated with a single DMARD, age and sex adjusted mean (95% CI) loss of productivity per year was €8410 (6015 to 11365) and in the combination therapy group, €5994 (3956 to 8639); the difference was −€2416 (95% CI, −5966 to 1091) (p = 0.17). Personal income before contracting rheumatoid arthritis had no predictive value for loss of productivity.
The loss was highest in the first year and was mostly (89%) because of sick leave (that is, work disability up to one year) (fig 3⇓); 113 patients fell into the sick leave category and 27 had permanent work disability. The proportion of patients with permanent work disability grew progressively with time, to 94% in the fifth year. The numbers of patients on sick leave compared with the numbers with permanent rheumatoid arthritis related disability pension were 33 v 37, 16 v 36, 16 v 33, and 15 v 36 in the second to fifth year, respectively. After the second year, productivity losses began to rise, but slowly, and the range was €6400 to €8320 per patient-year over the entire five year follow up. Loss of productivity was associated with poor clinical improvement and with an increase in the number of radiological erosions of the joints in hands and feet (table 2⇓).
Age and sex adjusted loss of productivity by improvement in rheumatoid arthritis* and by increase in the number of erosions in radiographs of the hands and the feet over a five year follow up
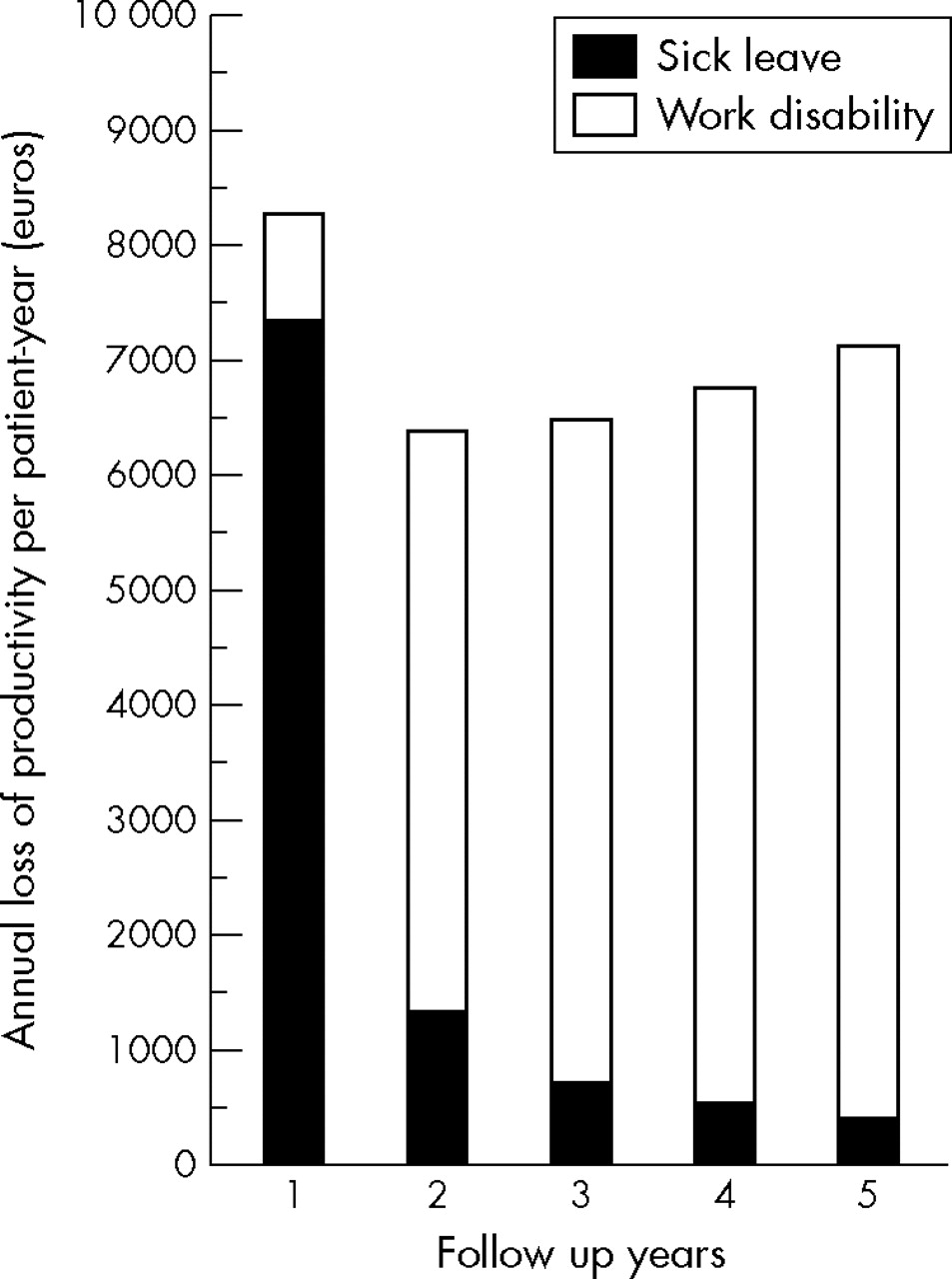
Loss of productivity per patient-year in each year of the five year follow up.
Mean (SD) HAQ score at six months was 0.30 (0.39) for women and 0.24 (0.36) for men. We divided the patients into two groups: those with score 0 and those with score >0, separately by the HAQ and by each ICF (sub)category to which the HAQ items were linked. As fig 4⇓ shows, this slight HAQ disability (78 patients with score >0) or restriction of function in any ICF (sub)category (39, 62, 46, 53, and 36 patients with score >0 in A, B, C, self care, and domestic life, respectively) translated into significantly higher productivity costs (p<0.001). In multivariate analysis, only disability in “changing and maintaining body position” increased the age and sex adjusted risk of higher losses (odds ratio (OR) = 4.4 (95% CI, 1.6 to 12.2); p = 0.005). Older age was a risk factor as well (OR = 1.1 (95% CI, 1.0 to 1.1); p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Loss of productivity per patient-year over a five year follow up by six month disability: total HAQ (Health Assessment Questionnaire) and HAQ items linked to ICF categories. Means (empty circles, patients with score 0; filled circles, patients with score >0) with 95% confidence intervals. Subcategories of mobility: A, Body position; B, Handling; C, Moving.
DISCUSSION
In this five year follow up study, we used more valid data—that is, work incapacity assessed by a physician and recorded in social insurance registers plus earnings assessed by the tax authorities—than the previous studies and could estimate the monetary value of lost productivity associated with recent onset active rheumatoid arthritis with greater accuracy than before. The losses because of sick leaves and because of rheumatoid arthritis related disability pension were computed separately, including time related changes over the follow up period.
Previous studies have not included sick leave, with a few exceptions.4,8,9 Two studies have followed up patients with early rheumatoid arthritis—for three years and one year, respectively—and used patient reported days off work and the gross income of all gainfully employed workers to estimate lost productivity using the human capital approach. Patient reported data, however, carry risk of recall bias, although data derived every three months correlated well with official data in a recent study.20 The mean (SD) annual loss in the German study, $11 750 (1120),8 was somewhat higher than in ours at the current exchange rate (€1 = $1.22). An explanation may be disparity of treatment: half of our patients initially received treatment with a combination of DMARDs, and the rate of permanent work disability was lower (25% in five years v 26% in three years) despite more active rheumatoid arthritis and fewer white collar workers. The change in components of lost productivity over time was parallel to our results. In the Swedish study, the average first year’s loss of productivity, €8726,4 is comparable to our €8320, although the Swedish patients had less active rheumatoid arthritis and only 70% of them were receiving DMARDs one year after inclusion, compared with 100% in our study. In addition, few of our patients were working part time. The effect of a single variable, however, cannot be analysed reliably. Another study from Germany used retrospective health care payer data over one year on patients with a mean rheumatoid arthritis duration of 8.4 years.9 The mean annual sick leave costs of the gainfully employed patients were €2835, and the mean annual work disability costs of the retired patients were €8358. The costs, however, did not include contributions by employers to social insurance and so on, and rheumatoid arthritis related disability could not be discriminated from other disability.
The outcome for our individual patients varied considerably (fig 2⇑). Not unexpectedly, the productivity losses were inversely related to improvement in rheumatoid arthritis (AUC of ACR-N15) over the five year follow up. We have shown earlier that aggressive initial treatment with a combination of DMARDs, compared with single DMARD treatment, reduces work disability days,11 and the six month treatment response strongly predicts future working capacity.21 Increase in radiological damage had a relation to productivity loss, although it was weaker than clinical improvement. Increased joint damage has been associated with a lower employment rate,22 but in early rheumatoid arthritis disease activity has been found to affect disability more than structural damage.23–,25
Despite the difference in work disability days in favour of the combination treatment strategy,11 no statistically significant difference appeared in loss of productivity. This is because we used the patients’ real incomes in computation of lost productivity, instead of mean income of all gainfully employed people.
The HAQ has been related to permanent work disability in almost all studies,26 with improvement in HAQ scores associated with increase in employment.22 In the present study, of the items of HAQ at six months, only the group of questions (table 2⇑) linked to the ICF subcategory “changing and maintaining body position” was independently associated with loss of productivity over five years. Thus, with regard to work capacity, the explanatory powers of the items of HAQ diverge.
We sought to include only rheumatoid arthritis related sick leave episodes in our study despite limitations of the register data. Our sick leave data did not include diagnoses requiring sick leave, some of which could have been conditions other than rheumatoid arthritis. However, all our patients with few exceptions were followed up strictly according to the study protocol, with all adverse events documented. Medical records of the patients with severe events and concomitant diseases (altogether 18) were reviewed, and only sick leave resulting from rheumatoid arthritis was included. Only sick leave lasting at least 10 days is registered if a new disease causes sickness absence. Consequently, our data did not capture all days off work, for instance those caused by ordinary infections, whereas repeated sick leave—as for those due to rheumatoid arthritis—were included in their entirety.11 Sick leave for rheumatoid arthritis is not usually short. The number of sick leave periods of less than 10 days was only nine (contributing 59 days) out of 264 (23 634 days) eligible for sickness allowance. We had no social insurance register data for 16 patients. However, they had visited a study centre regularly at least every six months until five years or until lost to follow up, and we could obtain data on their sick leave and longer work disability periods from case records which included duplicate copies of doctors’ statements with the diagnoses made for claiming work disability benefits. On the whole, we believe that very nearly all rheumatoid arthritis related work disability days were included in our analyses. The income data from statistics used in computing of lost productivity for 19 patients were valid.
As in most studies, we estimated the cost of lost productivity by the human capital approach (HCA).27,28 Another method, the friction cost approach (FCA), assumes that someone currently unemployed will replace the disabled worker after a friction period.16,27 Friction costs include costs of hiring, replacing, and training new employees, as well as lost productivity prior to absent workers’ being replaced, and the decreased productivity output associated with these new employees. The FCA yields estimates that in most cases are lower than the HCA estimates, but the validity of the FCA approach has been questioned.28
We estimated only the loss of productivity caused by days off gainful work. In a recent study on common pain conditions suffered by the US workforce, however, most of all lost productive time was explained by reduced performance while at work rather than by work absence.29 In chronic diseases such as rheumatoid arthritis, this “presenteeism” may be smaller.30 In addition, the HCA gives a zero value to productivity of individuals who are not paid for work, such as people working in their own household. In this sense, our results are underestimates of the entire real losses of work contribution.
Our results come from a study comparing two treatment strategies for rheumatoid arthritis, and are linked to the study protocol. The Finnish social security system may influence the occurrence of sickness absence. The rates of work disability have been in general higher in European countries than in the USA,3 where the welfare facilities are more limited but the labour force market more flexible. The monetary value of lost productivity is determined by income level. With these restrictions, our results may be generalised to patients with recent onset active rheumatoid arthritis.
In summary, the loss of productivity of patients with recent onset active rheumatoid arthritis was substantial, although all our patients received DMARD therapy and half underwent aggressive initial treatment with a combination of DMARDs. Good improvement in rheumatoid arthritis, however, can reduce the economic burden markedly. Consequently, all patients with early rheumatoid arthritis should receive aggressive treatment with DMARDs from the start. None of our patients was given biological agents during the five year follow up, and the role of these expensive drugs in early rheumatoid arthritis needs more research.31 However, as the average loss from one year’s work disability was €29 500, even a costly drug results in savings to society if it maintains a patient’s working ability. The ICF provides new insights into the assessment of work capability32 and can aid in the choice of patients suitable for vocational rehabilitation before loss of employment.33
Acknowledgments
The authors wish to thank the other members of the FIN-RACo Trial group, as follows: Leena Laasonen, MD, PhD; Martti Nissilä, MD, PhD; Heikki Julkunen, MD, PhD; Kaisa Vuori, MD; Leena Paimela, MD, PhD; Harri Blåfield, MD; Kirsti Ilva, MD; Urpo Yli-Kerttula, MD, PhD; Pentti Järvinen, MD, PhD; Jari Ahonen, MD; Mikko Hakola MD; Ilppo Pälvimäki MD; Sinikka Forsberg, MD; Oili Kaipiainen-Seppänen, MD, PhD; Tapani Helve, MD, PhD; Juhani Koski, MD, PhD; Marianne Gripenberg-Gahmberg, MD, PhD; Riitta Luosujärvi, MD, PhD; and Anna Karjalainen, MD, PhD.
REFERENCES
Footnotes
Published Online First 16 November 2005