Article Text

Abstract
OBJECTIVES To compare three therapeutic strategies using slow acting antirheumatic drugs (SAARDs) in early rheumatoid arthritis (RA), for their disease modifying properties, toxicity, and lag time until treatment effect.
METHODS Patients with recent onset RA from six hospitals were randomly assigned to immediate initiation of one of three treatment strategies: (I) a “mild SAARD with a long lag time” (hydroxychloroquine, if necessary replaced by auranofin); (II) a “potent SAARD with a long lag time” (intramuscular gold, if necessary replaced byd-penicillamine); (III) a “potent SAARD with a short lag time” (methotrexate, if necessary replaced by sulfasalazine). Comparisons included two years of follow up.
RESULTS All SAARD strategies reduced mean disease activity. A greater percentage of patients improved clinically with strategies II and III than with strategy I: percentages of patients improved on joint score with strategies II and III (79% and 82%, respectively), which was statistically different from strategy I (66%). The same was true for remission percentages: 31% and 24% v 16%, respectively). Longitudinal analysis showed significantly less disability with strategy III, and a lower erythrocyte sedimentation rate with strategy II than with strategy I. In addition, radiological damage after one and two years, was significantly lower in strategies II and III (at two years median scores were 11 and 10v 14 in strategy I, p<0.05). Toxicity was increased in strategy II compared with the other strategies.
CONCLUSION Strategy III, comprising methotrexate or sulfasalazine, produced the best results weighing effectiveness and toxicity. Strategy I (hydroxychloroquine or auranofin) was slightly less effective, and strategy II (intramuscular gold or d-penicillamine) was associated with increased toxicity.
- early rheumatoid arthritis
- rheumatoid arthritis
- disease modifying antirheumatic drugs
- slow acting antirheumatic drugs
Statistics from Altmetric.com
- early rheumatoid arthritis
- rheumatoid arthritis
- disease modifying antirheumatic drugs
- slow acting antirheumatic drugs
Rheumatoid arthritis (RA) is a chronic disease characterised by symmetrical polyarthritis. Pharmacotherapy consists of non-steroidal anti-inflammatory drugs (NSAIDs), slow acting antirheumatic drugs (SAARDs), and corticosteroids. Traditionally, RA treatment involved conservative management with NSAIDs given for long periods. If insufficiently effective, NSAIDs were supplemented with an SAARD. SAARDs are believed to influence the outcome of RA positively in contrast with NSAIDs, which are only symptom relieving. In the past decade the therapeutic management has changed towards more aggressive management. In line with other reports,1 ,2 our previous results from the Utrecht Rheumatoid Arthritis Cohort show that after one year early intervention with SAARDs is more effective than treatment with NSAIDs only.3
The SAARDs that are used to treat RA differ in their disease modifying properties, toxicity, and lag time until treatment effect. In general, the more potent SAARDs are also believed to be the more toxic. Antimalarial drugs (hydroxychloroquine) are thought to be the least effective and less toxic than the other SAARDs. The maximum beneficial effects of hydroxychloroquine are not seen until after three to six months.4 Oral gold (auranofin) has similar characteristics.5 ,6 Intramuscular gold andd-penicillamine are more potent but also more toxic,7-9 the lag time between the start and treatment effect is relatively long (more than three months). Many rheumatologists regard methotrexate as a potent and toxic drug, and therefore only prescribe methotrexate if other SAARDs are insufficiently effective. The effect of methotrexate has been shown to start within four to six weeks.10 Sulfasalazine is also regarded as an SAARD with a relatively short lag time.4 ,11
Thus the most commonly used SAARDs can be classified into three groups: mild with a relatively long lag time (hydroxychloroquine, auranofin), more potent with an expected long lag time (intramuscular gold,d-penicillamine), and potent with a relatively short lag time (methotrexate, sulfasalazine). It is not clear whether one of these SAARD groups is superior in the treatment of early RA. In this study the effectiveness, lag time, and side effects of the three different strategies according to the three groups described above are compared after one and two years of follow up.
Methods
PATIENTS
The study was designed as a prospective open label randomised controlled trial. Since 1990 all patients with recent onset RA (according to the American Rheumatism Association criteria),12 from all (six) rheumatological centres in the Utrecht region of the Netherlands, were asked to participate in a randomised prospective clinical trial. Disease duration had to be less than one year; most patients were enrolled shortly after the diagnosis was established. One university hospital and five general hospitals are included in this multicentre trial, covering a population of approximately one million people. The following exclusion criteria were applied: age <17 years; comorbid conditions that might interfere with one of the therapeutic strategies (such as malignancy, cardiac, respiratory, hepatic, and renal insufficiency); previous or current treatment with SAARDs, corticosteroids, cytotoxic or immunosuppressive drugs; possible pregnancy or breast feeding; psychiatric or mental disturbances that make adherence to study protocol unlikely. All patients signed informed consent; the ethical committees of all participating hospitals approved the study design. Baseline characteristics of patients eligible for the study but objecting to randomisation were compared with those of randomised patients to see if any selection bias had occurred.
TREATMENT
Patients entering the study were randomly assigned to one of three therapeutic strategies:
Strategy I: Treatment was started with hydroxychloroquine (400 mg daily): a mild SAARD with an expected long lag time until treatment effect; if necessary replaced by auranofin (6–9 mg daily), an SAARD with the same characteristics.
Strategy II: Treatment with intramuscular gold (aurothioglucose, IM gold, 50 mg weekly): a more potent and toxic SAARD with an expected long lag time; if necessary replaced byd-penicillamine (500–750 mg daily), an SAARD with the same characteristics.
Strategy III: Treatment with oral methotrexate (7.5–15 mg weekly): a relatively fast acting, potent SAARD; if necessary replaced by sulfasalazine (2–3 g daily), an SAARD with the same characteristics.
Randomisation was performed by an independent person, in blocks of 100 patients per hospital. The initial SAARD (hydroxychloroquine, IM gold, or methotrexate) was continued unless adverse reactions or ineffectiveness made discontinuation inevitable in the view of the attending doctor, in which case the second SAARD of that particular strategy was given. Treatment with an SAARD other than the initial or the second SAARD was regarded as discontinuation of the therapeutic strategy. Patients who could stop taking drugs owing to remission were not considered as having discontinued the strategy.
Use of NSAIDs and analgesics was allowed in all strategies. Oral corticosteroids and intra-articular injections with corticosteroids were avoided. Criteria for dose adjustment due to adverse reactions were described in detail in the study protocol. After one year of treatment responses were assessed for each patient. When improvement of at least 50% from the start of the drug was seen in at least three of four variables (pain, joint score, morning stiffness, erythrocyte sedimentation rate (ESR)) the SAARD was continued. The initial SAARD was stopped in patients who did not meet these criteria, and treatment with the second SAARD from the strategy was started. If a patient fulfilled the remission criteria at three subsequent visits (six months), the dosage of the SAARD was reduced to half—that is, halved dosages of hydroxychloroquine, auranofin, d-penicillamine, sulfasalazine were continued daily and halved dosages of IM gold, methotrexate were continued weekly. Patients were considered to be in remission when the duration of morning stiffness was ⩽15 minutes, the pain score was ⩽10 mm, the Thompson joint score was ⩽10, and the ESR was ⩽ 30 mm/1st h.13
PRIMARY END POINTS
Primary end points were pain, functional disability, joint score, ESR, and radiological damage.14 Assessments were performed at the start of the trial and repeated every three months, except for radiological damage, which was assessed annually. The same doctor or research nurse assessed clinical variables on each occasion. Functional disability was assessed with a validated Dutch version of the Health Assessment Questionnaire, range 0–3: zero representing the best (no problems) and three the worst score.15 ,16 Pain was measured separately for night and morning on two horizontal visual analogue scales of 100 mm; the mean of the scores was calculated. The joint score according to Thompson assessed the simultaneous presence of joint tenderness and swelling in a selection of joints weighted for joint size; range 0–534.17 ,18 Joints that received an injection within two months before an evaluation were not included in the score. ESR in mm after one hour was measured by the Westergren method. A modified method of Sharp was used to score radiological abnormalities.19 ,20 Erosions and joint space narrowing in hand and foot joints were scored and added to obtain a total score (range 0–448). Two investigators, unaware of the therapeutic strategy, evaluated all radiographs. Investigators evaluated the three consecutive radiographs for each patient in line and were aware of the sequence of radiographs. The scores of the first investigator were used in the analyses; the scores of the second were used to validate the scores of the first. Differences in total scores in individual cases of 25% or more were discussed until agreement was reached.
SECONDARY END POINTS
Additional end points were duration of morning stiffness (maximum 720 min); general wellbeing (horizontal visual analogue scale of 100 mm); grip strength (mean of three measurements of each hand with a Martin vigorimeter in kPa); serum concentration of C reactive protein (mg/l), haemoglobin concentration (mmol/l), and platelet count (×109/l). Rheumatoid factor status was considered positive if the qualitative Latex fixation test at a dilution of 1:1 was positive or the Rose-Waaler test was positive (that is, titre ⩾40 IU/ml), or both. These cut off points result in a positive test in fewer than 5% of the general population.
STATISTICAL ANALYSIS
The intention to treat principle was applied; in addition on-protocol or complier analyses were performed including only those patients who continued to be treated according to the randomised strategy. Differences in mean changes from baseline for all end points between the strategies were tested for statistical significance with analysis of variance (ANOVA) or the Kruskal-Wallis test, where appropriate. Radiological damage, morning stiffness, C reactive protein, and platelet count showed a skewed distribution. Therefore, median scores were presented for these variables. ANOVA for repeated measurements was used to study differences between the strategies using all the nine three-monthly measurements in analysis. Both the “between-subject” or strategy effects and the “within-subject” or longitudinal time/overall treatment effects were tested. ANOVA for repeated measurements required variables to show a normal distribution.
Clinically relevant improvement in a single primary end point for individual patients was defined as an improvement of 33% or more compared with baseline.21 Patients were considered to have a clinical response when they improved by 20% or more compared with baseline on at least three of four primary end points (radiological damage excluded).22 ,23 Differences between the strategies were tested for significance with the χ2 test. The definition of remission by Scott et al was used, as mentioned earlier.13
No adjustments were made for multiple comparisons.24 Power calculations for functional disability as one of the primary end points indicated group sizes of 100 to be sufficient for detecting 20% difference between groups at α = 0.05 and 1−β = 0.80. Statistical analyses were performed with the SPSS for Windows statistical package, version 6.1.25
Toxicity was studied in each strategy. As it is notoriously difficult to relate an adverse event to specific drug treatment, all possible adverse events are included in the analysis.26 ,26a For effectiveness analysis the intention to treat principle was followed. The same applied for toxicity analysis. As a consequence, all adverse events, even if patients discontinued the assigned treatment strategy, were included in this analysis. Most patients (99%) also took NSAIDs; therefore, the reported events might also be the result of NSAID use. However, both the rate of events unrelated to antirheumatic drug treatment and NSAID related toxicity are expected to be equally distributed across the three strategies, and consequently not considered to bias the results.
Results
PATIENT CHARACTERISTICS
In April 1998 313 patients had been randomised and had completed at least two years of follow up. Data on 31 randomised patients who were lost to follow up (dropouts) and on 52 patients who did not agree to be randomised were not included in analyses, but baseline characteristics were compared with those of the other groups. Eleven patients (9%) in strategy I, 12 (11%) in strategy II, and eight (7%) in strategy III were lost to follow up, after a mean period of 7.5 months, which was not significantly different between the strategies. Nine of these 31 dropouts died of causes unrelated to RA or its treatment (cardiac (six patients), respiratory insufficiency (one), malignancy (one), sepsis (one)); four patients were excluded because of other serious disease processes (coronary heart disease, malignancy, lung disease, immobility due to car accident); in three cases the diagnosis of RA turned out to be incorrect (systemic lupus erythematosus (two), no chronic rheumatic disease (one)); one patient moved out of the study region; 14 patients refused to be treated following the protocol despite initial consent (two from strategy I, six from II, and six from III).
Table 1 shows baseline characteristics of all the patients. The male/female ratio is typical for an RA population. Mean age was rather high for patients with recent onset RA, but in line with recent epidemiological data in the Netherlands.27 Disease duration of all patients was less than one year. Baseline disease status for the randomised groups was comparable and indicated a relatively active disease. Baseline characteristics of the 31 patients lost to follow up were in general comparable with those of the therapeutic groups, except that these patients were older. Death was one of the main reasons for dropout, which might explain the higher age. The 52 patients who did not agree to be randomised had slightly better baseline values (table 1).
Baseline characteristics1-150
STRATEGY SURVIVAL
Discontinuation of the strategy implies treatment with an SAARD other than the first or the second assigned SAARD. In the first year 27 patients (9%) discontinued the randomised strategy, and during the second year 53 (17%), giving a total of 80 patients (26%) in two years (table 2). Discontinuation rates did not differ statistically significantly between the three strategies. However, strategies I and II showed slightly higher rates (27%, 30%) than strategy III (20%). The main reason for discontinuation was insufficient effectiveness in strategies I and III and adverse reactions in strategy II. Additional reasons were refusal of gold injections, refusal to take oral drugs, and refusal of further treatment with any SAARD. In total, 86% of the patients at one year and 47% at two years were still treated with the initial randomised SAARD (hydroxychloroquine, IM gold, or methotrexate). In strategy III the maximum weekly dose of methotrexate was 7.5 mg in 51% of the patients, 10–15 mg in 43%, and in 6% the study protocol was violated and the dose was increased to 17.5–25 mg. Folic acid (0.5 mg six days a week; not on the day of methotrexate intake) was used by 33% of patients. Folic acid was used more in patients receiving higher doses of methotrexate: 45% of patients using 10 mg/week methotrexate, or higher doses, compared with 21% of patients receiving methotrexate 7.5 mg/weekly.
Number of patients whose assigned strategies were discontinued and reasons for discontinuation
CORTICOSTEROIDS
Restricted use of oral corticosteroids as adjuvant treatment appeared to be unavoidable in comparable percentages of patients in each of the three strategies: 8% during the first year and 12% during both years. Intra-articular injections were given at least once to 28% of the patients during the first year and to 44% during both years. No significant difference in this respect between the three strategies was found.
EFFECTIVENESS
Changes from baseline
Changes from baseline were significant for all primary end points in each strategy, indicated by the 95% confidence intervals of the mean changes (table 3). Improvement seemed slightly less in strategy I than in the other strategies. However, no significant differences in change scores were observed between the three strategies, except for radiological damage. Although radiological progression was rather small, median scores after one and two years were significantly worse for strategy I than for strategies II or III. Complier analyses also showed no significant differences between the three strategies, except for radiological damage at one year, which was again high in strategy I (data not shown). All secondary end points also improved significantly from baseline in each strategy. Differences between the strategies were small and statistically not significant, except for improvement in grip strength after the first year which was significantly less in strategy I than in III (table 4).
Changes from baseline in primary end points
Changes from baseline in secondary end points
Longitudinal trends
Figures 1 to 5 show longitudinal trends in the primary end points. Analysis for repeated measurements included only those subjects with complete data at all measurements during the two years: disability (150 patients), pain score (243), joint score (247), ESR (237), and radiological damage (312). Disability over time was favourable in strategy III compared with I (fig 1, p = 0.04). There was no significant difference between the three strategies for pain (fig 2) and joint scores (fig 3). The ESR over time was significantly higher in strategy I than in II (fig 4, p = 0.01). Results showed significant decreases in disability, pain, joint score, and ESR over time in all three strategies. Figure 5 shows the radiological progression. Owing to the skewed distribution of radiological damage, median scores are presented instead of means. Square root transformed data, which showed a normal distribution, were used in repeated measurement analysis. A significant increase in the radiological damage score over time was seen in each strategy with significant interaction between longitudinal treatment effect and strategy effect, showing a faster increase in strategy I than in strategies II (p = 0.03) or III (p = 0.01). Progression in strategies II and III was comparable (p = 0.67).
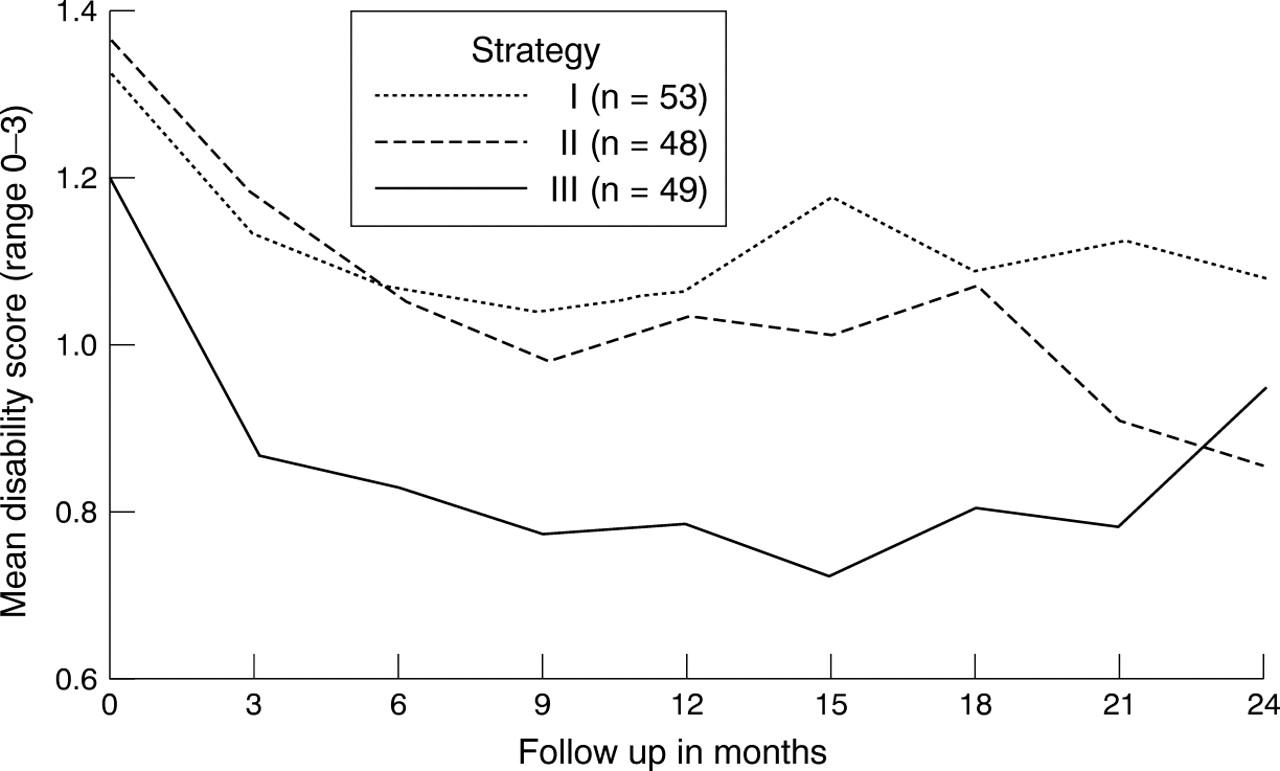
Mean disability score in 150 patients with available data on disability for all nine measurements in each therapeutic strategy. There was a significant difference between strategies I and III (p = 0.04), and a significant decrease in disability over time in each strategy (analysis of variance for repeated measurements).

Radiological progression in the three strategies. Significant increase over time in each strategy with significant interaction between overall time-treatment effect and strategy effect, showing a faster increase in strategy I than in strategy II (p = 0.03) and strategy III (p = 0.01). No significant difference between the three strategies (p = 0.23) (analysis of variance for repeated measurements).

Mean pain score in 243 patients with available data on pain for all nine measurements in each therapeutic strategy. Significant decrease in pain score over time in each strategy, no significant difference between the strategies (p = 0.23) (analysis of variance for repeated measurements).

Mean joint score in 247 patients with available data on joint score for all nine measurements in each therapeutic strategy. Significant decrease in joint score over time in each strategy, no significant difference between the strategies (p = 0.30) (analysis of variance for repeated measurements).
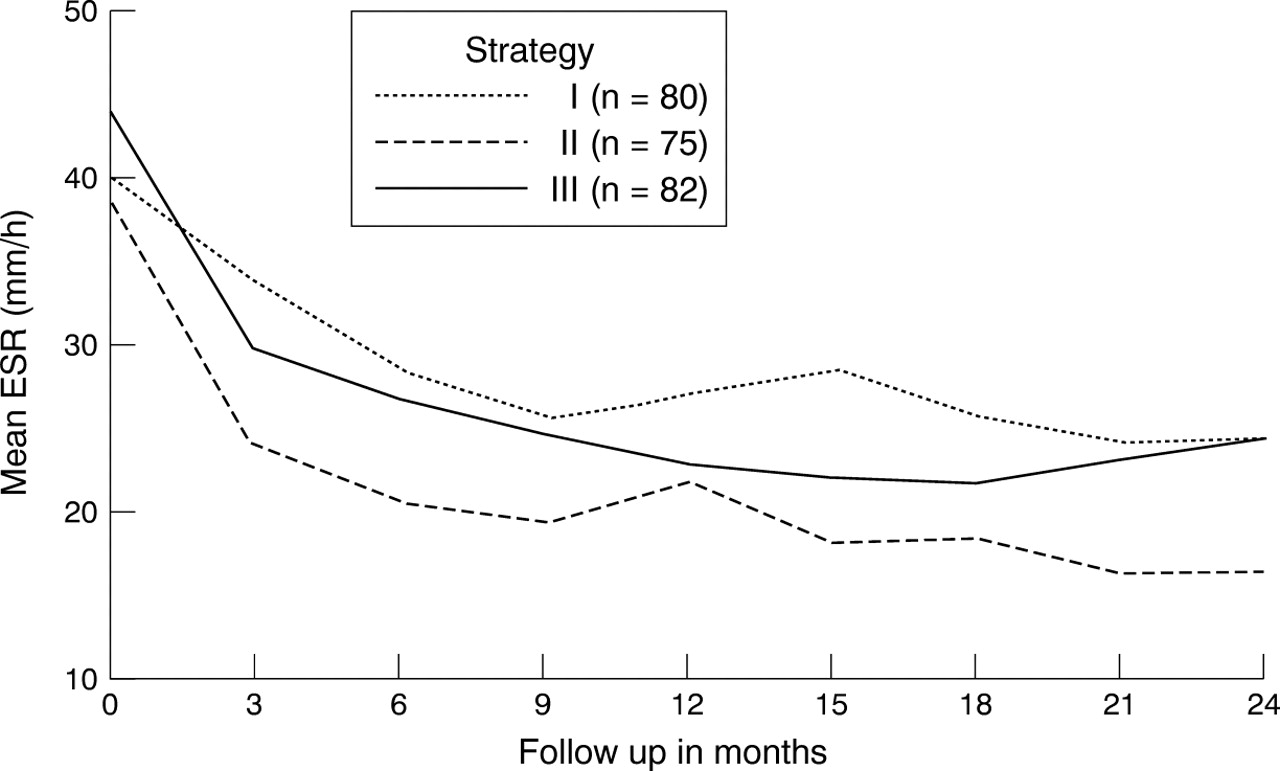
Mean ESR score in 237 patients with available data on ESR for all nine measurements, in each therapeutic strategy. Significant difference between strategies I and II (p = 0.01), and significant decrease in ESR over time in each strategy (analysis of variance for repeated measurements).
Lag time until treatment effect
The lag time until treatment effect was deduced from the slopes of the lines during the first months. Figures 1, 2, and 3 show no clear differences in lag time between the three strategies, whereas the change in ESR occurred faster in strategies II and III than in I (fig4). During the first months the slope was steeper in strategies II and III, and levelled off after about three months, whereas the slope in strategy I was less steep and levelled off after about nine months. These numerical differences did not reach statistical significance.
Clinical improvement
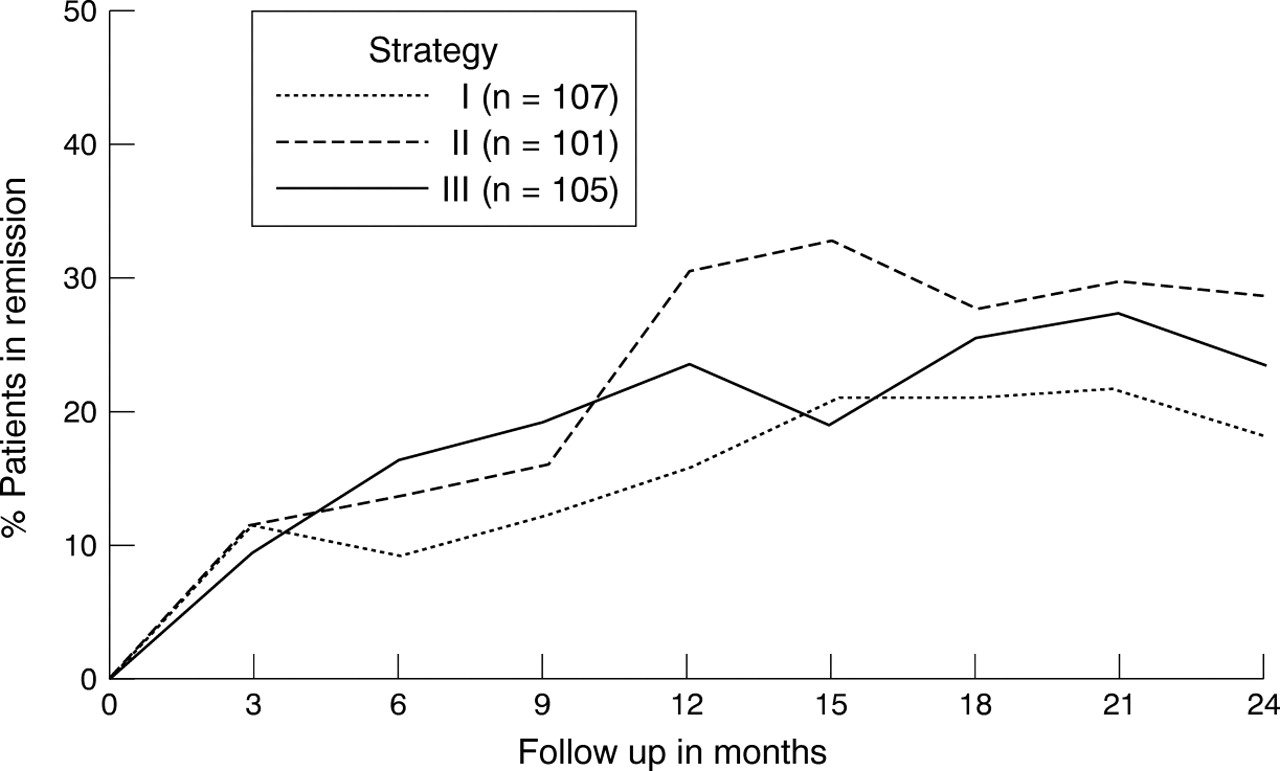
Table 5 shows the percentage of patients exhibiting clinical improvement. At one year the percentage of patients whose joint score had improved was 79 in strategy II and 82 in III, which is better than in strategy I (66%) (p = 0.02). Remission rates at one year were also higher in strategies II (31%) and III (24%) than in strategy I (16%, p = 0.04), but no obvious differences were seen at two years. Complier analysis showed higher clinical improvement and remission rates in strategy III at one year compared with strategies I or II (not statistically significant). At year two, clinical response rate was high in strategy II (80%) compared with strategies I (61%) or III (63%) (p=0.03) (data not shown). Figure 6 shows the percentage of patients fulfilling remission criteria at a single measurement (intention to treat analysis). Remission rates were slightly higher in the complier analysis (27%) at two years than in the intention to treat analysis (24%).
Patients with clinically relevant improvement5-150, clinical response5-151, and remission5-152 after one and two years

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of patients in remission at each measurement in time. Remission is defined as morning stiffness ≤15 min, pain score ≤10 mm, joint score ≤10, and ESR ≤30 mm/ 1st h.
TOXICITY
Investigation of toxicity included three-monthly clinical reports and laboratory abnormalities. All reported or observed symptoms were included (table 6). Most patients (99%) also took NSAIDs. Therefore, the reported events might also have been the result of NSAID use. In strategy I most events were subjective gastrointestinal complaints (52), followed by anaemia (21), and rash (17). Mucocutaneous reactions occurred most commonly in strategy II (62); subjective gastrointestinal complaints and hepatotoxicity were most commonly seen in strategy III, and renal toxicity was more commonly seen in strategies II (24) and III (17) than in strategy I (11). These observations are in line with other published reports.28
Clinical symptoms and laboratory abnormalities in each treatment strategy
Most patients reported toxicity (240, 77%): at least one “adverse” event was reported by 76 patients (71%) in strategy I, 81 (77%) in strategy III, and in 83 (82%) in strategy II. The mean number of events for each patient was high in strategy II: 2.1, compared with 1.6 in strategy I and 1.7 in strategy III. Most events were mild, not leading to any change in dose or type of SAARD (432 of 563 events, 77%). Fifty two events led to dose adjustments of SAARD (18 in strategy I, 17 in II, and 17 in III). A total of 79 events led to permanent discontinuation of an SAARD, which occurred more often in strategy II (46 events) than in strategies I (17) or III (16). In strategy II (46 events) the drugs discontinued were IM gold in 30 cases, d-penicillamine in 11 cases, and other SAARDs in five. The drugs discontinued permanently owing to toxicity in strategy I were hydroxychloroquine in 10 cases and auranofin in five cases and in strategy III were methotrexate in 11 and sulfasalazine in four cases, and other SAARDs for the remaining cases.
All events were reversible, apart from four reported malignancies (breast, skin, nasopharyngeal, and oesophagus carcinoma) and one pulmonary disorder (other than pneumonitis). The malignancies were probably unrelated to treatment. One case of pneumonitis occurred in strategy II during IM gold treatment and one in strategy III during methotrexate treatment. A more detailed description of toxicity related to the initial randomised drugs has been performed.26a
Discussion
In this randomised study a comparison of three therapeutic strategies was made for patients with recently diagnosed RA. This study is considered representative for patients with RA referred to hospital, as all patients with recent onset RA attending six rheumatological centres, who fulfilled the inclusion criteria, were asked to participate. The study is not community based as the population base referred to patients with RA attending a rheumatological centre (specialised setting). The results are applicable to patients with early RA presenting to a rheumatologist (that is, hospital based). To enrol the majority of the patients and obtain an unselected sample of patients, from whom results are applicable to clinical practice, only a small number of exclusion criteria were used. Although the open label design applied in this study might enhance bias in effectiveness and toxicity assessments, its protocol is closely connected to clinical practice. Consequently, the effectiveness (effects under ordinary circumstances—that is, the pragmatic approach) rather than efficacy (effects under ideal conditions) of treatment was studied.29 ,30
This study showed significant improvements on all primary and secondary end points (except for radiological damage) for all three strategies. The differences between the strategies favoured strategies II and III rather than strategy I; however, this was only statistically significant for improvement in joint score and remission at one year. Longitudinal analysis showed less functional disability in strategy III, and lower ESR in strategy II than in strategy I. In addition, radiological damage after one and two years was significantly lower in strategies II and III than in strategy I. Radiological progression during the first two years of disease was small in all strategies, which might be the result of the early introduction of SAARD treatment. Consequently, the differences found at two years are not of major clinical importance. However, if linear progression proceeds at the same rate in subsequent years, differences between the strategies may become clinically significant.
The two-year analyses showed few statistically significant differences between the strategies apart from the significantly greater radiological progression in strategy I. However, trends in the other primary end points all favour strategies II or III. Therefore, we conclude that effectiveness in strategies II and III was superior to that of strategy I. No significant differences were observed between strategies II and III, though this study is too small to dissociate clearly between these strategies. Strategy II has minor disadvantages—namely, slightly more radiological progression and toxicity. Strategy III comprised methotrexate with a maximum dose of 15 mg weekly; 43% of patients treated with methotrexate exceeded a weekly dose of 7.5 mg and another 6% exceeded 15 mg. Recently, higher doses are being used, even in early RA. The effectiveness and toxicity of higher doses are to be evaluated.
After two years, 80% of the patients in strategy III were still treated according to the randomised strategy, which was slightly higher than the 73% in strategy I and 70% in II. Complier analysis showed similar results to those of the intention to treat analysis, with slightly better effectiveness for strategy II, suggesting that if IM gold (followed by d-penicillamine) had not been discontinued owing to side effects, strategy II would have been as effective as strategy III or even a little better. The higher rate of toxicity in strategy II is an obvious disadvantage.
This study focuses on treatment strategies rather than on specific drugs, which increases the number of patients continuing treatment. The characterisation of strategy I as being mild seems justified. Effectiveness was less than for the other strategies and toxicity was less than in strategy II. The characterisation of strategy II and III as including more potent SAARDs also seems correct in terms of effectiveness, which was better than that of strategy I. The toxicity rate in strategy II was high compared with strategy III, indicating that SAARDs used in strategy II are more toxic than the SAARDs in strategy III, in the prescribed dosages. As for the characterisation of the strategies according to the length of the lag time until treatment effect, it is concluded that strategy I is associated with a long lag time and III with a relatively short lag time. The assumption that strategy II was also associated with a long lag time was shown to be incorrect; similar slopes were seen for strategies II and III. Since our first measurement was after three months, no conclusions can be drawn for the preceding months.
Although we did not compare single drugs, we believe that the effectiveness measured after one year is mainly the effect of the initial randomised drug. This is less true at two years, since the initial randomised SAARD was still used by 86% after one year but by only 47% after two years of follow up. Other studies on the effectiveness of SAARDs were often of shorter duration, or included fewer patients. Summarising these studies, moderate effectiveness of hydroxychloroquine and auranofin has been reported,5 ,31while better effectiveness for other SAARDs has been found, without clear differences between these SAARDs.11 ,32-34 As for radiological damage, patients treated with IM gold, methotrexate, or sulfasalazine had a slower progression than those treated with hydroxychloroquine, auranofin, or azathioprine when three different trials were compared.20 ,35-37 At five years, greater progression was found for d-penicillamine than for methotrexate.38
SAARDs have been shown to reduce disease activity, but remission occurs in a minority of patients. Although the definitions of remission differ between studies, the reported remission rates are concordant, and never exceed 25%.7 ,8 ,39 ,40 Remission rates of 24% after two years for patients treated with IM gold and 12% in patients treated with methotrexate have been reported.8 ,41 In 257 patients with early RA, followed up for four years only 15% fulfilled remission criteria for at least two consecutive visits.42In our study remission rates at one year varied from 16 to 31% and at two years from 19 to 29%. Although these rates are in concordance with earlier studies, we believe that the ultimate goal in treating RA—that is, a lasting clinical remission, is achieved in too few cases. Other treatment options are to be searched for to increase remission rates. Combination treatment, including more than one SAARD at the same time or new biological agents, has not been shown to be clearly superior, but may be of interest and needs further evaluation.43 As this and our previous study show, the early start of an SAARD is probably more important than the choice of the SAARD.3 In addition intensive, individualised treatment might increase treatment effectiveness, which might need a paradigm shift from aiming for improvement to aiming for remission.
References
Footnotes
The authors wish to acknowledge C Cornelis, R Huisman, A Jacobs-van Bree, van Mourik, and S van Wijk for the collection of data and their contributions to the Utrecht Rheumatoid Arthritis Cohort. Grant support: The Dutch League against Rheumatism (Het Nationaal Reumafonds).