Article Text

Abstract
Objective: Survival analysis of a series of 366 consecutive patients with systemic sclerosis (SSc).
Methods: Clinical and laboratory data were evaluated from 1983 until 2005 using a standard protocol. The female/male ratio was 315/51. The mean (SD) age of the patients was 56.8 (12.2) years. The duration of disease was 12 (5–19) years with a median follow-up of 6 (3–12) years.
Results: Kaplan–Meier univariate analysis showed that renal, cardiac involvement, pigmentation disturbances, malabsorption, a forced vital capacity <50%, diffuse scleroderma, presence of early malignancy, anaemia, and increased erythrocyte sedimentation rate (ESR) were signs of unfavourable prognosis, whereas anti-centromere antibodies were indicators of a good survival. In the multivariate Cox proportional hazards model the presence of diffuse scleroderma, renal involvement, coexistence of a malignant disease, and increased ESR were poor independent prognostic signs. Elderly age at the onset of disease also caused an unfavourable outcome. A total of 86 SSc-related deaths were recorded during the follow-up. Of them, 65% were attributed to cardiorespiratory manifestation of disease. Tumour associated early death was found in 12 cases (14%).
Conclusions: In addition to the well-known factors influencing the outcome (diffuse subset, internal organ involvements, and inflammatory signs), the coexistence of scleroderma with a malignancy also causes a poor outcome.
Statistics from Altmetric.com
Systemic sclerosis (SSc) is characterised by vascular abnormalities, fibrosis, inflammation, and atrophy affecting the skin and internal organs. Previous univariate survival analysis studies indicated that the presence of diffuse skin involvement,1–9 male sex,4 6 8 11 older age at the onset of the SSc,1–3 5–7 12–14 internal organ manifestations including the heart,1–7 10–13 15–17 kidney,2–4 6 7 13–15 17 18 gastrointestinal tract,2 15 18 lung involvements,1–7 10 11 14 15 18 pericarditis,3 4 14 clinical signs of right heart failure,7 11 pigmentation disturbances,2 nailfold capillary loss seen on capillaroscopy,14 joint contractures,10 and decreased oral aperture1 were associated with poor survival. Anti-topoisomerase antibody,1 5 7 anaemia,1–3 13 14 18 increased erythrocyte sedimentation rate (ESR),1–3 5 10 13 increased C-reactive protein (CRP) level,4 abnormal urine sediment,1 16 proteinuria without scleroderma renal crisis1 13 were also associated with a bad prognosis of the disease, while anti-centromore (ACA) positivity6 was a favourable prognostic factor.
The Cox proportional-hazards model showed that older age,3 6 11 12 14 19 renal involvement,3 6 14 19 severe lung involvement,2 5 13 18 clinical signs of right heart failure,7 11 the presence of diffuse SSc,3 6 and a greater extent of skin involvement2 were unfavourable independent prognostic signs.
Stepwise Cox proportional-hazard models are widely used to identify the minimum set of clinical-laboratory prognostic factors. By this method, older age,5 6 diffuse cutaneous involvement,3–7 heart,3 6 16 severe lung3 5–7 16 and kidney3 6 7 involvements were factors indicating a poor survival.
The aim of the study was to determine predictors of survival in a large series of 366 consecutive patients with SSc.
PATIENTS AND METHODS
A total of 366 patients with SSc were enrolled in the study between 1983–2005 using identical, simple standard investigations.2–4 20 The median disease duration was 12 years with the lower-upper quartiles of 5–19. The female/male ratio was 315/51. The mean (SD) age of the patients was 56.8 (12.2) years. The median follow-up was 6 (3–12) years (lower-upper quartiles), the mean disease duration was 13.5 (10.8) years.
Patients were first enrolled at the University Centre in Debrecen (3rd Department of Internal Medicine) until August 1995. Then, the same investigators (LC, ZN) moved to another tertiary university reference centre (University of Pécs, Medical School), and continued the enrolment.
Cases followed up for at least 6 months or dying within the first 6 months were included. A total of 38 patients were lost after a follow-up of at least 6 months. Another 27 cases were not included in the study because of the insufficiency of the available clinical data. These latter patients did not substantially differ in their clinical characteristics compared to the cases included in the study. Based on the detailed description of the extent of skin involvement and clinical-laboratory data, we used the two subset classification model similar to our previous studies.2–4
Out of the 171 patients enrolled in Debrecen, 23 patients continued his/her follow-up in Pécs. In August 1995, another 20 patients neither continued visiting Debrecen nor moved to Pécs for regular check up. In Pécs, 194 patients were enrolled and followed up from 1995.
With regard to the evaluation of the cause of death, symptoms that might be loosely associated to the SSc were not excluded, and only those events that showed absolutely no relationship to the SSc were taken as censored data.
The following items were recorded at the time of enrolment: age at the onset; duration of disease at entry, sex, calcinosis, teleangiectasia, extent of skin involvement according to body areas, skin hypo/hyperpigmentation, Raynaud phenomenon, and hand contractures. Patients with azotemia and/or malignant hypertension were considered as having scleroderma renal crisis. Cardiac involvement was encoded in case of pericarditis, conduction disturbances; myocardial ischemia on ECG; recurrent arrhythmia. Dysmotility and stricture/dilatation of the lower part of oesophagus were investigated by barium swallowing. Lung manifestation of SSc was diagnosed in the presence of bibasilar lung fibrosis in the chest roentgenogram and/or a forced vital capacity between 50–80%. Severe lung involvement was indicated in the presence of diffuse lung fibrosis on chest roentgenogram, and/or forced vital capacity was below 50%. Paraneoplastic syndrome (tumour associated scleroderma) was diagnosed if the onset of the malignancy and SSc was detected within four years.
Anti-centromere antibodies were detected on HEp-2 cells by the indirect immunofluorescence method. Anti-topoisomerase 70 autoantibody was detected using a commercial ELISA kit. Anaemia was recorded in a haematocrit level less than 33%, increased ESR was established, in a value above 40 mm/hr.
The therapy of patients included Ca channel blockers (81%), angiotensin-converting enzyme (ACE) inhibitors (37%), pentoxyfyllin (67%), proton pump inhibitors/H2 blockers (75%), low-dose corticosteroids (23%) during the entire follow-up period. d-Penicillamin (23%), and colchicin (10%) were used exclusively in the first period. In the second period cyclophosphamid (17%), other cytostatic agents, predominantly azathioprin and metotrexat (14%), and prostanoids (13%) were also administered.
Statistical methods
Kaplan–Meier survival curves and log rank tests were performed.21 Items with significant effects on survival with univariate method were entered into the Cox proportional hazards model. We also added the age/gender of the patient, the location of the centre (Pécs–Debrecen).22 The minimum set of predictive variables was determined by backward stepwise selection.
RESULTS
Clinical findings
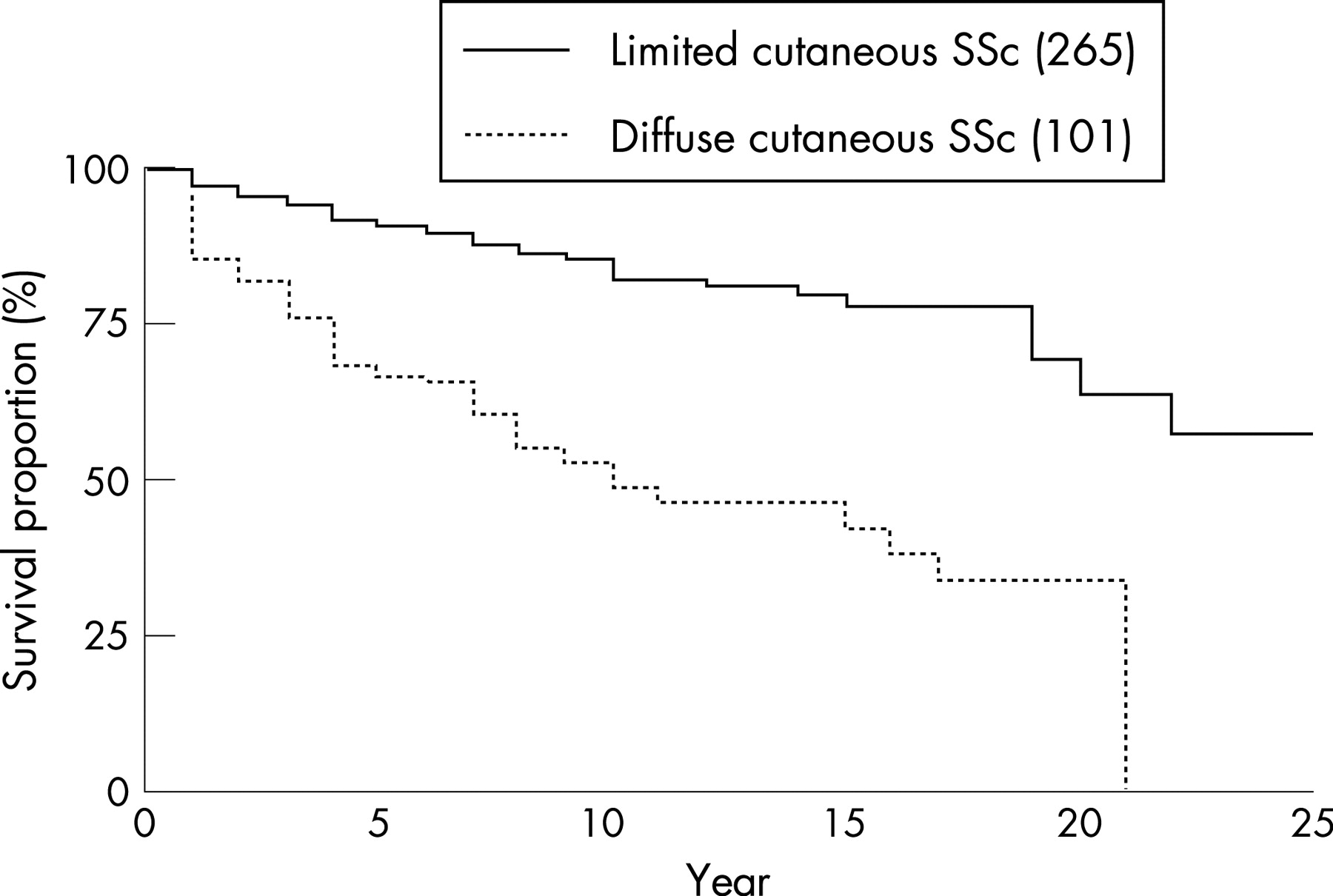
The major clinical findings are depicted in table 1. The Kaplan–Meier cumulative 5-year overall survival rate was 84%, and the 10-year survival was 72.6% (table 2). In diffuse cutaneous (dc)SSc, the 5- and 10-year survival rate was 67% and 48.6%, respectively. In limited cutaneous (lc)SSC we found 90.5% and 81.8% 5- and 10-year survival rates, respectively (p<0.001). Male patients had 78.3% and 66% while females showed 84.9% and 73.6% 5- and 10-year survival rates, respectively (NS). Patients followed-up in Debrecen had 83.1% and 71.7%, the ones followed-up in Pécs had 85.9% and 75.2% 5- and 10-year survival rates, respectively (NS).
Univariate analysis
Poor outcome of the disease was demonstrated the dcSSc subgroup (fig 1), in the presence of skin pigmentation disturbances, renal, heart involvements, malabsorption, anaemia, forced vital capacity (FVC)<50%, anti-topoisomerase and coexistence of a malignancy, increased ESR, and diffuse subset (table 2, fig 2). Anti-centromere antibodies caused a favourable outcome (fig 3). The most lethal association was the combination of cardiac and kidney involvement with a 5-year survival of 14% (data not shown).



{kind=link}
{kind=link}
{kind=link}
Multivariate analysis
Diffuse SSc, age at onset of the disease, renal involvement, increased ESR and paraneoplastic syndrome (coexistence of SSc and a malignancy) were independent prognostic factors. The stepwise selection procedure showed that dcSSc, age at the onset of the disease, kidney involvement, increased ESR and early coexistence of a malignancy (paraneoplastic syndrome) are the minimum set of prognostic factors of poor survival (table 3).
Cause of death
A total of 93 patients died during the follow-up; 86 deaths were caused by SSc. In eight cases more than one organ insufficiency was the cause of death. Pulmonary and/or cardiac manifestation of disease was attributed to 65% of the deaths. The cause of death was interstitial lung involvement in 20 cases, pulmonary arterial hypertension in 7 cases, heart involvement in 26 cases, and cardio-respiratory involvement in 3 cases (clear-cut distinction was not possible, this category probably includes cases with pulmonary arterial hypertension). Scleroderma renal crisis was the cause of death in 16 patients. Middle dose corticosteroid treatment administered in primary/secondary care (6 cases), a decreased renal blood flow caused by either GI bleeding (2 cases) or infection-related loss of body fluid (2 cases) were the major causes of the relatively high number scleroderma renal crisis. SSc cases with coexistent tumour caused a fatal outcome in 12 cases (14%). Gastrointestinal tract-related death (malabsoption/dysmotility, bleeding from watermelon stomach) was found in 8 cases. Severe bleeding due to watermelon stomach was related to the fatal outcome in 4 patients. In 2 cases, severe infection was detected as the cause of death.
DISCUSSION
Our survival analysis findings are in accordance with studies coming from other centres.1–18 20 We also confirmed our previous Cox proportional hazards model investigation showing that heart, kidney manifestations, diffuse SSc, elderly age, and increased ESR were among the poor prognostic factors.3 One of our new observations is that the coexistence of scleroderma and a malignant disease also causes a poor outcome (tables 1–3). In previous clinical studies the overall prevalence of scleroderma-related malignant tumours varied between 2.6–11.3%,1 2 11–13 15 and the rate of early malignancies appearing within 4 years following the onset of SSc was 1.5–4.5%.23–26 These values coincide with our 4.4% early malignancy rate.
The gastrointestinal bleeding caused by watermelon stomach may also have some increasing importance in the outcome of SSc (table 2).27 28 Of the 8 GI tract related deaths, 3 were attributed to the presence of gastric vascular ectasia (watermelon stomach). All these cases have been identified in the last few years of our follow-up, therefore we assume that the proportion of this abnormality may increase.
We are not able to evaluate properly the importance of pulmonary arterial hypertension, because of the lack of appropriate investigations in the first phase of the study. Seven patients died due to PAH indicating the increasing importance of this abnormality.
REFERENCES
Footnotes
-
Competing interests: This work was supported by the Hungarian NKFP grant (1/026/2001), the Hungarian Ministry of Health and Social Welfare grant (ETT 643/2003), and by the National Foundation for Scientific Research grants (OTKA T26429, OTKA T043017).
-
Competing interests: None declared