Article Text

Abstract
Objective: To determine whether bone attrition (flattening or depression of the subchondral bone) was associated with the presence and severity of knee pain and to evaluate the coexistence of attrition and other MRI features likely associated with pain.
Methods: Participants in the Framingham Osteoarthritis Study, a community cohort unselected for OA, answered questions about knee pain and underwent knee x rays and MRI. Attrition, bone marrow lesions (BMLs) and effusions were scored on MRI using the WORMS scale. We assessed attrition in knees with and without pain, and using logistic regression examined its association with pain adjusting for age, gender, Kellgren–Lawrence (K–L) grade, BMI, BML and effusion. We also explored the relation between attrition, pain severity and nocturnal pain.
Results: Attrition (Grade ⩾2) was present in 28% (167/592) of painful knees and in 10% (106/1035) of non-painful knees (adjusted OR 1.6 (95% CI 1.1 to 2.2)). Of knees with OA (n = 368), 74% had pain if attrition was present and 58% if it was absent (adjusted OR 1.2 (95% CI 0.7 to 2.0)). Of knees without OA (n = 1222), pain was reported in 39% of knees with attrition and in 27% without it (adjusted OR 2.1 (95% CI 1.1 to 4.0)). We found no association between either attrition/pain severity or attrition/nocturnal pain. Attrition often co-occurred with other OA features associated with pain such as BMLs and effusions.
Conclusions: Attrition was associated independently with knee pain. Unlike knees without OA, the association was lost in OA knees where other pathological features that may cause pain also coexisted.
Statistics from Altmetric.com
Although traditionally considered a disease of hyaline articular cartilage, osteoarthritis (OA) is a process that involves all the joint tissues: subchrondral bone,fibrocartilage (such as menisci), ligaments, muscle, capsule and synovium.1
The sources of pain in OA remain unclear. Studies to date have indicated variable associations between knee pain and loss of hyaline articular cartilage, an aneural tissue.2–5 Other abnormalities such as effusions, synovitis and meniscal tears have been linked to pain in OA.6 7 Subchondral bone may also play an important role in pain generation. For example, pain relief is evident after osteotomy, likely secondary to a decrease in intraosseous pressure.8 Moreover, bone marrow lesions (BMLs) are associated with the occurrence of pain in some subjects with knee osteoarthritis.5 9 10
Bone attrition, the least studied change in subchondral bone, has been assessed either as a loss of bone on conventional radiographs11 12 or as flattening or depression of the articular cortex by MRI.13 Although Ahlback decades ago introduced a grading system that included an evaluation of attrition using conventional radiographs, attrition may be difficult to detect in the absence of a clear defect of cortical integrity.11 Traditionally, attrition has been described in advanced OA. Nagaosa et al found an association of bone attrition with osteophyte size.14 Conversely, in a cross-sectional study of selected OA knee patients awaiting total knee replacement, there was no significant correlation between attrition scores and the presence of joint space narrowing, osteophytes or Kellgren–Lawrence grade.12
The association of attrition with pain has not been studied as extensively as the relation of pain with other features.6 7 Data from a study by Dieppe and colleagues12 showed that night pain in patients awaiting a total knee replacement may be associated with radiographic attrition. Using MRI data, a cross-sectional study of 143 individuals with painful knee OA reported that knee pain severity was associated with bone attrition, BML, meniscal tears and synovitis/effusion.7 We are unaware of any examination of whether attrition differentiates painful from non-painful knees.
The purpose of this study was to evaluate in a large community cohort: (1) the overall prevalence of subchondral bone attrition; (2) whether bone attrition was associated with the presence and severity of knee pain as well as nocturnal pain; and (3) the co-occurrence of attrition with other features that are likely associated with knee pain.
METHODS
Subjects
Our study cohort consisted of two separate groups, (1) members of the Framingham Heart Study Offspring Cohort and (2) a newly recruited cohort from the town of Framingham, Massachusetts. Participants in this combined group, designated the Framingham OA Study Cohort, were examined between 2002 and 2005.
The Framingham Heart Study Offspring Cohort participants included surviving descendants (and spouses of descendants) of the Original Framingham Heart Study cohort subjects.15 As part of a study of the inheritance of OA, selected participants were originally examined from 1992 to 1995. All surviving members of this group and those not lost to follow-up were contacted by telephone and invited to participate. A validated survey instrument16 supplemented by questions about medication use was used to exclude patients with rheumatoid arthritis.
The newly recruited participants to the Framingham OA Study Cohort were drawn from a random sample of the Framingham community. Participants were recruited using random digit dialling and census tract data to ensure inclusion of a representative sample of the community. Fliers were hung in public areas to increase awareness of the study, which was focused on bone health, foot health and arthritis. To be included, subjects had to be at least 50 years old and ambulatory (the use of assistive devices such as canes and walkers was allowed). Exclusion criteria were the presence of bilateral total knee replacements and a positive screen for rheumatoid arthritis as above.16 In neither group was participant selection based on the presence or absence of knee OA or knee pain.
Approval for the study was obtained from the Boston University Medical Center Institutional Review Board.
Pain assessments
Participants were asked about knee symptoms with the following questions:
In the past 30 days, have you had pain, aching or stiffness on most days in either of your knees?
Was the pain, aching or stiffness in your right knee, left knee or both knees?
Was the pain, aching or stiffness in your knee (right or left) mild, moderate or severe?
They also filled out the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire, a validated instrument to assess knee pain and disability.17
-
Pain definition. Knee pain was defined as being present when the subject reported pain, aching or stiffness on most days in the past 30 days. All other knees were classified as having no knee pain.
-
Pain severity. All subjects with knee pain were asked to quantify their pain in each painful knee as mild, moderate or severe.
-
Nocturnal pain. Nocturnal pain was defined as being present when the subject reported any response greater than “none” to the WOMAC question: “How much pain do you have at night while in bed?” Those who reported none to this question were categorised as having no nocturnal pain.
Radiographic assessments
All subjects underwent bilateral weight-bearing radiography using a PA-fixed flexion approach with a Synaflex frame.18 Radiographs were scored on a modified Kellgren–Lawrence (K–L) scale.19 A knee was considered to have radiographic OA if its K–L grade was ⩾2.
MRI assessments
Based on an agreement with the parent Framingham Heart Study to limit the respondent burden of the Framingham Offspring subgroup, only those who had knee pain underwent MRI of the knee(s), and both knee MRIs were read when acquired. For the community sample, all subjects had bilateral knee MRIs whether or not they had knee symptoms, and because of monetary constraints, only their right knee was read. Participants with MRI contraindications were not scanned, and those with one total knee replacement had only their native knees scanned.
All studies were performed with a 1.5-T MRI system (Siemens, Mountain View, CA) using a phased array knee coil. A positioning device was used to ensure uniform placement of the knee among subjects. T2-weighted fat-suppressed images in the sagittal and coronal planes were acquired, using the following pulse sequence parameters: repetition time (TR) 3610 ms, echo time (TE) 40 ms, slice thickness 3.5 mm and field of view (FOV) 14 cm. T1-weighted spin images in the sagittal plane were acquired, using the following pulse sequence parameters: TR 480 ms, TE 24 ms, slice thickness 3.5 mm and FOV 14 cm.
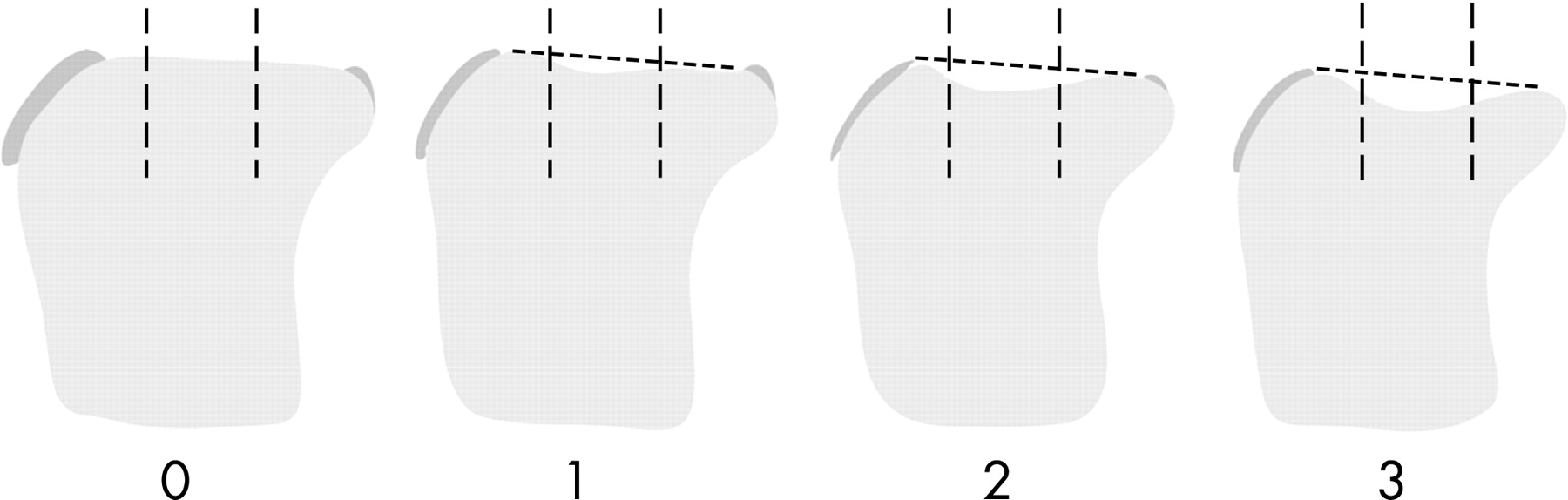
MR images were analysed with the semiquantitative whole-organ scoring method (WORMS).13 WORMS evaluates attrition in 14 regions of the knee: anterior, central and posterior segments of the medial and lateral femur and tibia, respectively, and the medial and lateral patella. Attrition is scored from 0 to 3, based on the subjective degree of deviation from the normal contour: 0 = normal, 1 = mild, 2 = moderate and 3 = severe (fig 1). Bone marrow lesions were read in these same regions, and defined as irregular areas of increased signal in the T2w sequences adjacent to the subcortical bone scored from 0 to 3, based on the regional involvement: 0, none; 1, <25% of the region; 2, 25–50% of the region; 3, >50% of the region. Effusions were scored on a scale of 0–3, based on effusion volume.
Two radiologists blinded to subject pain status performed a single assessment of the MRIs (each radiologist read roughly 50% of the total population). A random sample of 16 knees was selected, each with 14 regions to assess reproducibility of reading (224 regions per feature). The inter-rater agreement for bone attrition was a weighted Κ value of 0.56 (95% CI 0.40 to 0.72), and for BMLs 0.83 (95% CI 0.75 to 0.91).
A knee was categorised as having attrition if any region had a minimum score of 2; we chose this cut-off to improve the specificity of the MRI attrition finding. Second, we defined maximal bone attrition score as the maximal attrition grade recorded in any of the 14 regions of the knee.
Like attrition, we considered BMLs as being present if a knee had at least one BML grade ⩾2, as suggested by previous work.9 The maximal BML score for a knee was also defined as being the maximal grade recorded in any of the 14 regions of the knee. Effusions were considered as being present within any score from 1 to 3.
STATISTICAL ANALYSIS
We first computed the overall prevalence of all grades of attrition in the study sample. To evaluate the association of bone attrition with knee pain, we compared the crude prevalence of attrition (grade ⩾2) among knees with and without pain using a χ2 test. We then evaluated this association using logistic regression with generalised estimating equations to account for correlation between knees, adjusted for age, gender, radiographic severity (K–L grade), BMI, presence of BMLs and effusions. In addition, we performed the same analysis separately, each in the subgroups of knees with and without radiographic OA.
We also carried out the same adjusted models to evaluate the association between bone attrition and pain severity (mild, moderate and severe) as well as attrition and nocturnal pain. Finally, we assessed the co-occurrence of bone attrition and other MRI features such as BML and effusion, and tested for trend (unadjusted and adjusting for age, gender, K–L grade, BMI and effusion), the proportion of painful knees among different bone attrition and BML scores.
RESULTS
Bone attrition and pain
A total of 1627 knees (1273 subjects) from the Framingham OA cohort were included. Among all knees, 592 (36%) had pain. The characteristics of the participants according to their knee pain status are shown in table 1. Subjects with knee pain were more frequently older, females and with a greater BMI. The prevalence of radiographic OA was 40% in the group of knees with pain and 13% in the knees without pain.
Table 2 presents the prevalence of different grades of bone attrition among the study population.
Bone attrition (Grade ⩾2) was present in 28% of the knees with pain and in 10% of knees without pain (p<0.0001). In regression analysis, we found that attrition was associated with the presence of knee pain (OR 3.3 (95% CI 2.5 to 4.5)). This association persisted but was attenuated after adjustment for age, gender, BMI, BMLs, effusions and K–L grade (OR 1.6 (95% CI 1.1 to 2.2)).
Further, of 1222 knees without radiographic OA, 39% of those with attrition (40/103) had pain, whereas 27% of those without attrition (298/1119) had pain (OR 2.4 (95% CI 1.4 to 4.1); adjusted OR 2.1 (95% CI 1.1 to 4.0)). Similarly, of 368 knees with radiographic OA, 74% of those with attrition (124/167) had pain, whereas 58% of those without attrition (116/201) had pain (OR 2.1 (95% CI 1.4 to 3.4), adjusted OR 1.2 (95% CI 0.7 to 2.0). Thus, attrition was clearly related to pain in knees without radiographic OA, whereas in the group with OA, the association was diluted after adjusting for confounders. The major confounder affecting the odds ratio was the K–L grade.
Bone attrition and pain severity
Of all knees with pain, moderate and severe pain combined were more common if attrition was present (64% of knees) than if it was absent (51% of knees). An association of pain severity with the presence of attrition was significant in the crude model (OR 1.6 (95% CI 1.1 to 2.3)). Nevertheless, after adjusting for confounders, it became non-significant (OR 0.9 (95% CI 0.6 to 1.4)).
Bone attrition and nocturnal pain
We found no association of attrition presence with nocturnal pain (OR 1.1, 95% CI 0.5 to 2.1; adjusted OR 1.0, 95% CI 0.5 to 2.1).
Co-occurrence of MRI features
We found that in 73% of all knees, both maximal bone attrition score and maximal BML score coexisted in the same knee region (fig 2).

{kind=link}
{kind=link}
We assessed and tested for trend the proportion of painful knees among different levels of maximal attrition and maximal BML scores in the same knee (see table 3).
The proportion of knees with pain tended to be greater in the presence of both attrition and BML. For example, a higher proportion of knees with both grade ⩾2 attrition and grade ⩾2 BML were painful (65%) than knees without attrition (grade 0) and BML (grade 0) (24%). Also, higher grades of attrition were associated with pain, for instance, in knees with BMLs of grade 1, percentages of knees with pain increased from 32% to 53% with increasing attrition grades. However, this trend was driven by radiographic severity in the adjusted model, and adjusted tests for trend were non-significant.
Further, we found that independent of knee pain status, effusions coexisted in knees with attrition and BMLs. For instance, of painful knees, the proportion with effusion was 20% in the group without BML and without attrition, 62% if only attrition was present and 77% if both BML and attrition coexisted.
DISCUSSION
Results from this cross-sectional study suggest that bone attrition is associated with knee pain. This relationship persisted after adjustment for other factors that also have been linked to knee pain, suggesting an independent association of attrition with pain. This association was more evident in knees without x ray OA. Additionally, we found a coexistence of attrition with BML and effusion among painful knees. These findings support the notion that the occurrence of knee pain is multifactorial, with contributions by numerous features in the entire joint organ.
The sources of knee pain are not clearly understood. Subchondral bone, a richly innervated tissue, is thought to be involved in pain generation.8 20 In addition to BMLs, an important subchondral bone abnormality strongly associated with pain,5 9 10 most studies have focused on other bone changes such as osteophytes and eburnation, and findings on their association with pain have been conflicting.21
We found that bone attrition was more frequent among painful knees than among knees without pain. However, in contrast to the finding that attrition is just a late-stage feature in OA, we showed that attrition was associated with pain in the absence of radiographic OA, suggesting that it may participate in the generation of pain in early or mild stages of the disease. Attrition may represent bone remodelling changes in response to mechanical stresses.
In the subgroup with x ray OA, many structural abnormalities also linked to pain coexisted. In this subgroup, the relation of pain with attrition became non-significant when we adjusted for K–L grade, a measure of x ray severity. When we adjust for OA severity, we may be controlling for a variable on the causal pathway linking attrition to pain (OA→attrition→pain). Adjusting for this variable makes results difficult to interpret, because bone attrition is related to OA severity. When we looked for the association in the absence of OA severity (group without OA), we found an independent relation of attrition with pain.
Unlike Torres et al,7 who reported an association between attrition and higher median scores of pain on a visual analogue scale, we did not find any link between bone attrition and pain severity, as measured by an ordinal scale. Nor could we confirm the suggestion that BMLs relate to pain by way of attrition; BMLs in our data related to pain independent of attrition. We did not find any association between bone attrition and night pain, as was previously reported. Nevertheless, that previous association was described in a selected OA population.12
A major finding of our study that is particularly noteworthy is the co-occurrence of multiple MRI abnormalities (BML, attrition and effusion) among painful knees. Furthermore, attrition and BML coexisted in the same knee region. Pain was more prevalent among knees that had both features, in comparison with knees that had signs of only attrition or BML. The prevalence of pain was also higher with progressive increments in the grade of attrition scores, but this trend was driven by radiographic severity.
This study takes advantage of a large community cohort unselected for OA. Because we studied large number of knees both with and without knee pain and with and without OA, we were able to better describe the association of bone attrition and pain, an association that would have otherwise been difficult to do in a study with a smaller and/or selected sample.
However, there are potential limitations to the current study. First, the reliability of attrition readings was only moderate. Despite this, we were still able to detect an association of attrition with pain. Second, our study did not compare the MRI vs the x ray bone findings. It is probable that what some authors called attrition by x rays are later bone changes than those detected by MRI. However, we selected grade ⩾2 as the cut-off for defining “true” attrition. Future studies to address this issue are required. Third, this was a cross-sectional study. Longitudinal studies may be necessary for a better understanding of pain causality. Nevertheless, we anticipate that the coexistence of several features will continue to make this a complex problem to study.
In summary, bone attrition is associated independently of other MRI features with the presence of knee pain. However, attrition usually coexists with multiple other pathological features, many of them associated with pain, suggesting that complex and multiple relationships between different features of OA are involved in OA-related knee pain.
Acknowledgments
This study was supported by the NIH (grants AR47785 and AG18393) and the NHLBI (contract NO1-HC-25195). Dr Reichenbach is the recipient of a Research Fellowship from the Swiss National Science Foundation (PBBEB-115067).
REFERENCES
Footnotes
-
Funding: None declared.
-
Competing interests: None declared.