Article Text

Abstract
Objective: To study prescription patterns of biological treatment in rheumatoid arthritis (RA) patients in southern Sweden, a region with no formal or economic restrictions for the use of biological treatment in rheumatological diseases. Specifically, we studied conformity with the national Swedish guidelines for biologics in RA.
Methods: Rheumatologists in southern Sweden contribute to a voluntary register on the use of biologics in treating arthritis patients (the South Swedish Arthritis Treatment Group (SSATG)). This register covers >90% of all the prescriptions of biologics for arthritis patients in the region. The treatment of 1839 patients (2704 treatment occasions) was recorded in the SSATG register during 1999–2006. Baseline characteristics were analysed.
Results: Baseline Health Assessment Questionnaire (HAQ) scores and Disease Activity Scores (DASs) decreased significantly between 1999 and 2006, but disease activity remained high in RA patients. RA patients were treated with biologics earlier, but only 16% of the patients received biologics within 2 years of disease onset in 2006. The percentage of RA patients who were prescribed biologics after only one previous non-biological DMARD (disease-modifying anti-inflammatory rheumatic drug) was 27% in 2006. Thirty-five per cent of all RA patients changed from one biological treatment to another.
Conclusions: Baseline DASs in RA patients remained high at the start of biological treatment. The national Swedish guidelines for the prescription of biologics in RA were followed. More patients with early RA were treated with biologics. The proportion of RA patients changing from one biological drug to another increased.
Statistics from Altmetric.com
Etanercept, infliximab and adalimumab (antitumour necrosis factor antagonists, anti-TNF-drugs), anakinra (an interleukin-1 receptor antagonist) and rituximab (a monoclonal antibody against CD-20 positive B cells) have all demonstrated good efficacy in patients with inflammatory rheumatological diseases.1–5 The term “biologics” and “biological treatment” in rheumatology refers to these drugs. The international consensus on the introduction of biologics in rheumatoid arthritis (RA) is that patients should have active disease and tried at least one non-biological DMARD (disease-modifying anti-inflammatory rheumatic drug), and that cost considerations should be taken into account.6
In Sweden, rheumatologists initiate treatment with biologics and monitor the progress of rheumatological patients. The latest Swedish Society for Rheumatology guidelines from March 2004 recommend that biologics should be prescribed for rheumatoid arthritis (RA) patients showing high disease activity, or intermediate disease activity with negative prognostic factors, who have shown intolerance to or an unsatisfactory response to methotrexate. In RA patients with intermediate disease activity, combination therapy with methotrexate, sulfasalazine and chloroquine (or methotrexate and ciclosporin) is recommended as an alternative to biologics for patients showing an unsatisfactory response or intolerance to methotrexate. The guidelines are the same for both early and established RA. No specific level of disease activity, for example no minimum limit of Disease Activity Score (DAS) or number of swollen and tender joints, is required for initiating biologics in the Swedish guidelines (http://www.srfonline.org; http://www.das-score.nl). The first Swedish national guidelines in 2002 also stipulated that at least two DMARDs should have been tried, one of which should be methotrexate.
In southern Sweden, a voluntary professional rheumatological network has been in operation since 1999, with the aim of including all cases of biological treatment of patients with arthritic conditions. In this region, there are no formal, economical or practical restrictions on prescribing biologics in rheumatological diseases. The information is gathered in the register of the South Swedish Arthritis Treatment Group (SSATG).7
Our aim was to study the prescription practice and pattern of biologics in the SSATG register regarding baseline characteristics in RA patients. We wanted to describe some background trends required for health economic modelling and resource allocation. This also included information on switching between biologics. Specifically, we wanted to study conformity with international and national Swedish guidelines for the use of biologics in RA. We hypothesised that: (1) biologics would be prescribed to patients with shorter disease duration, and thereby also to younger patients, (2) biologics would be prescribed to patients with less severe disease, (3) the number of RA patients treated with biologics would level off and (4) compliance with national guidelines would decrease, as suggested in another report.8 Finally, we also wanted to study (5) baseline characteristics in biologically naïve compared with biologically non-naïve RA patients.
MATERIAL AND METHODS
Data on all patients included in the SSATG register from 1 March 1999 to 31 December 2006 were analysed. Rheumatologists in 12 hospitals and 5 private practices in southern Sweden contribute to this voluntary register. The aim is to register all rheumatological patients prescribed biologics regardless of diagnosis. In the region of Skåne in southern Sweden (total population 1.1 million, 7 hospital departments, 5 private practices), the SSATG register covers >90% of all of biologics prescriptions as compared with pharmaceutical sales.9 The patients are monitored locally by rheumatologists according to a structured protocol.7 The decision to initiate and cease treatment with biologics is made by the local rheumatologists and is not subject to any strict protocol or regulations. The reporting takes place on paper, with central data entry to ensure uniform interpretation and completeness of data. Missing clinical data are requested twice a year.
The SSATG protocol includes demographics, information on previous and ongoing DMARDs, prednisolone dosage, measures of disease severity (Health Assessment Questionnaire, HAQ10), disease activity (28 tender and swollen joint counts), patient’s pain and global health visual analogue scales (VAS), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and evaluators’ global assessment of disease activity (5-degree Likert scale). These measures are used to calculate the Disease Activity Score using the 28 joint count (DAS28) (http://www.das-score.nl). Previous validation has shown that 1987 American College of Rheumatology classification criteria for RA were fulfilled by >98% of patients assigned this diagnosis.9 11 No formal approval of the ethics committee was necessary, as the protocol was designed to meet the legislative requirements on patient documentation in Sweden.
Statistics
The Statistical Package for Social Sciences (SPSS, Chicago) version 14.0 was used for the statistical analyses. Spearman’s rho test was used to test trends over time for the continuous variables. The SigmPlot version 10 was used for the figures.
RESULTS
Patient characteristics
Altogether, 2704 biological treatment episodes in 1839 RA patients were included in the SSATG register from 1999 to 2006. Baseline characteristics are given in table 1. In summary, these RA patients had longstanding and disabling disease, had high disease activity and were therapy refractory. In this observational setting, the mean number of swollen and tender joints was nearly equal. A comparison of baseline demographics in different RA patient cohorts on biologics in different countries is shown in table 2.
Biologically naïve RA patients
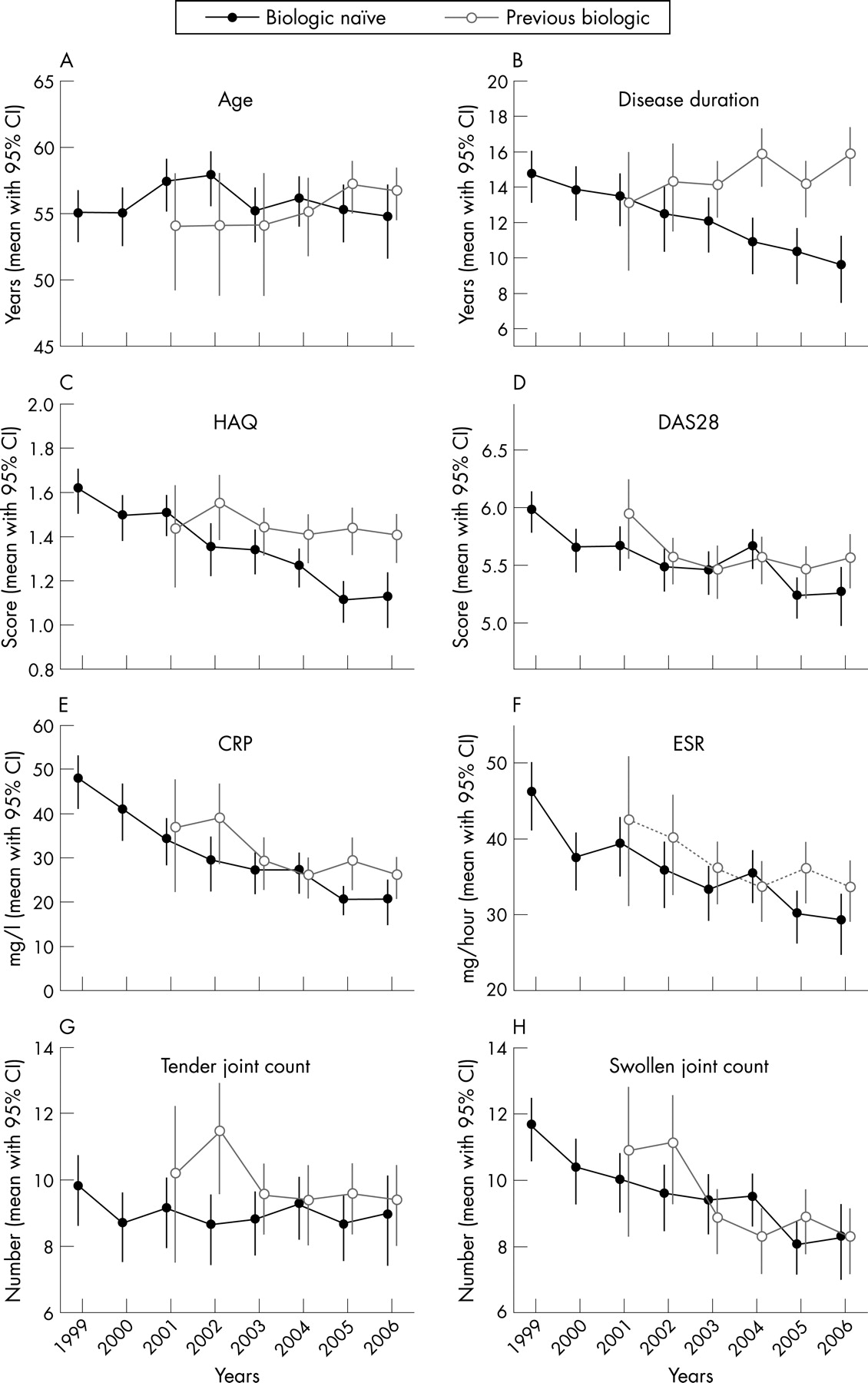
For biologically naïve RA patients, there was a significant negative trend from 1999 to 2006 in baseline disease duration, DAS28, swollen joint count, VAS global health and pain, HAQ, CRP and ESR. Age and tender joint count remained essentially stable over the period. This is illustrated in fig 1A–H, where the lack of overlap in 95% confidence intervals indicates significant differences. The mean DAS28 was 5.4 at initiation of biological treatment in RA in 2006.

In 1999, 15% of the biologically naïve RA patients received treatment within 5 years from disease onset, 59% had a disease duration of 5–20 years, and 26% had a disease duration of >20 years. In 2006, 42% of the biologically naïve RA patients starting biological treatment had a disease duration of less than 5 years, 42% of 5–20 years, and 17% of >20 years. The percentage of biologically naïve RA patients starting biologics within 2 years of disease onset showed a fivefold increase, from 3% in 1999 to 16% in 2006.
There were significant decreasing trends in the number of previous DMARDs and decreasing use of oral corticosteroid treatment in the biologically naïve RA patients (fig 2A–C). Over 93% of the biologically naïve RA patients had previously been treated with methotrexate, regardless of the year.

{kind=link}
{kind=link}
The percentage of biologically naïve RA patients who had previously been taking only one non-biological DMARD increased progressively from 3% in 1999 to 27% in 2006, as did the percentage of patients who had been prescribed 2 consecutive prior DMARDs, from 10% in 1999 to 19% in 2006. On the other hand, biologically naïve RA patients having taken more than 2 consecutive DMARDs decreased from 56% in 1999 to 23% in 2006. The percentage of biologically naïve RA patients with previous combination DMARD treatment varied between 23% and 34%, with no clear trend over time.
Biologically non-naïve RA patients
The demographics and disease activity of the RA patients changing to other biologics are also given in table 1. Overall, RA patients switching between biologics represented a population with particularly longstanding and disabling disease with intolerance/lack of response to traditional DMARDs, but with similar disease activity as compared with the biologically naïve RA patients. Since RA patients switching between biologics are also part of the biologically naïve group in this biologics register, and the group of RA patients switching between different biologics are analysed in this paper as treatment occasions, care must be taken in formal statistical comparisons. To give an indication of possible different characteristics, 95% confidence intervals are given. There were 865 cases of treatment in 636 RA patients switching biological therapy (35% of all biologically naïve RA patients). Of these, 463 (73%), 128 (20%), 35 (5.5%) and 10 (1.5%) had tried 1, 2, 3 or >3 previous biological drugs, respectively.
Disease duration and HAQ remained stable from 2001 to 2006 for RA patients who had previously received biological treatment; otherwise the pattern was similar to those for biologically naïve RA patients regarding measures of disease activity (fig 1A–H). Prednisolone dosage decreased significantly during this period, but the number of previous DMARDs remained high (fig 2A–C).
Biologics prescription pattern for RA patients
The number of RA patients receiving treatment with any biological drug in any year seemed to increase almost linearly between 1999 and 2006 in the SSATG register. However, when looking at actual new RA patients starting biological treatment per year, there are two clear trends of decrease, the first in 2001–2002 and the second in 2006. The decrease in 2001–2002 coincides with the unavailability of etanercept in Sweden during this period. The increase in 2003–2005 coincides with the increased availability of self-administered anti-TNF drugs. There was a trend of levelling off in the prescription of biologics in 2006 for RA patients.
The prescription pattern of the different biological drugs has varied according to the availability of biological drugs in Sweden. Etanercept dominated as the first drug in 1999. The availability of etanercept decreased in 2000–2002 in Sweden, and infliximab became the dominant drug. From 2003, when all biologics were readily available in Sweden, there is a clear trend towards a preference for etanercept and adalimumab in southern Sweden, as both primary and switching biological drugs. The prescription of anakinra peaked in 2002, and it is almost exclusively used as a switching drug. Rituximab has only been used as switching drug, as suggested in the Swedish Society for Rheumatology guidelines.
DISCUSSION
Regarding our first hypothesis, RA patients are treated earlier with biologics. However, this was not reflected by a decrease in age, implying that older RA patients and possibly also patients with more comorbidity were treated with these remedies. Over 40% of the biologically naïve RA patients had a disease duration of less than 5 years in 2006. Reports of good response and remission in early RA treated with biologics have probably contributed to this trend.12 13 However, only 16% of RA patients were prescribed biologics within 2 years of disease onset in 2006. Furthermore, the increasing number of patients switching between biologics clearly demonstrates the existence of a large therapy-resistant RA population, which we at present lack good evidence to identify, although long disease duration, older age, unability to use methotrexate, female sex and poor HAQ score seem to be associated with poor response to biologics 14–16. However, switching to a new biological agent may reduce disease activity and pain, and improve functional status irrespective of the reason for discontinuing the first drug as reported from small series.17–20 Clearly, this should be studied further.
Regarding our second hypothesis, there was a clear trend towards less disease activity in RA patients in 2006 than in 1999 when they were first prescribed biologics. This may be interpreted as either less stringency in the inclusion criteria or a sliding indication in the prescription of biologics towards less severe disease, consistent with remission being the treatment goal.21 However, even though no formal minimum levels of DAS or number of swollen or tender joints are required in Sweden for initiation of biologics in RA, RA patients receiving biologics still had a high disease activity in 2006. We interpret this to show compliance with the national and international requirements of high disease activity in RA at initiation of biologics.
Also in line with national and international guidelines, over 90% of the RA patients in this register had received methotrexate before the initiation of biologics. The proportion of biologically naïve RA patients who had received only 1 or 2 non-biological DMARDs previously increased over time, whereas the proportion of patients who had received more than 3 DMARDs decreased.
The unrestricted policy of prescribing biologics in Sweden probably minimises both patients’ and physicians’ aggravation of symptom bias. Thus, the situation in Sweden is different from that in other countries such as the UK, Finland and Denmark, where there have been/are either formal or practical limitations for the use of biologics 8 15 22–24. This must be kept in mind when comparing results from other study populations, as illustrated in table 2. However, other factors, for example patient preferences, the local capacity to administer infusions, repeated infections and the physician’s judgement of the most appropriate drug, may well influence the choice of drug. Such factors cannot be fully controlled in an observational setting but must be kept in mind when studying reports on drug adherence and adverse events in such settings.15 25 26 In spite of these differences, a decrease in disease activity at onset of biologics has also been reported from Denmark and Norway, although our study was longer.8 The prescription of biologics will of course change if the pattern of adverse event changes or major economic forces come into play, thereby making comparisons between different biological drugs in the observational setting very difficult.27 28
We have previously demonstrated almost complete reporting to the SSATG register from the rheumatological network in southern Sweden,9 and we have no indications that the reporting rate is decreasing, implying that the current information together with efficacy and tolerability data in the observational setting is valuable for health economic modelling and resource allocation.
In summary, our first and second hypotheses were largely confirmed. RA patients with both shorter disease duration and less severe disability are being increasingly treated with biologics. Regarding our third hypothesis, there are at present indications of a trend of levelling off in the proportion of RA patients being treated with biologics in southern Sweden in 2006. Our fourth hypothesis, that is poorer adherence to the national guidelines in prescribing biologics, was not confirmed. The Swedish guidelines for prescription of biologics are followed, regarding active treatment of RA, the requirement of high disease activity at initiation of biologics and previous methotrexate use; all this in spite of a lack of formal or economic restrictions in the prescription of biologics in RA in this region. Regarding our fifth hypothesis, biologically naïve and biologically non-naïve RA patients were demographically almost identical, but non-naïve patients had a longer disease duration and less concomitant DMARD treatment.
Acknowledgments
We would like to thank Jan-Åke Nilsson for help with the statistical analyses. We are grateful for the help provided by all our colleagues and the staff of the South Swedish Arthritis Treatment Group for their cooperation and provision of data. This study was supported by grants from Österlund Foundation, Kock Foundation, King Gustav V 80 Jubilee fund, Lund University Hospital funds and Reumatikerförbundet.
REFERENCES
Footnotes
-
Competing interests: None.