Article Text

Abstract
Objective: To examine the risk factors for self-reported work disability in patients from the LUpus in MInorities: NAture vs. Nurture cohort with systemic lupus erythematosus (SLE).
Methods: Patients with SLE of Hispanic (Texas and Puerto Rico), African American and Caucasian ethnicity were studied. Work disability was defined by patients’ self-report. Only patients known to be employed at the baseline visit were included. The probabilities of self-reporting work disability over time were examined by the Kaplan–Meier method; differences between ethnic groups were examined by the log-rank test. The relationship of baseline socioeconomic–demographic, clinical, behavioural and psychological features with work disability was examined by standard statistical tests. Variables with p⩽0.10 in these analyses were examined by logistic regression.
Results: The rate of self-reported work disability among the 273 patients studied was 19% at 5 years; it was numerically higher for the African Americans (25%) than for the Hispanics from Texas (19%) and the Caucasians (18%). The rate for the Hispanics from Puerto Rico was 7% at 2 years; 5-year rates could not be estimated for this ethnic subgroup (shorter follow-up in the cohort). In the regression analysis, age, male sex, poverty, total disease duration, disease activity and damage accrual were predictors of work disability.
Conclusions: The rate of work disability was 19% at 5 years. Patients with SLE with more severe disease and with lower socioeconomic status are at high risk of becoming disabled. The toll SLE imposes could possibly be reduced in patients at risk if, in addition to medical treatment, services needed to overcome their disadvantageous socioeconomic status are provided.
- ACR, American College of Rheumatology
- LUMINA, LUpus in MInority populations: Nature vs. Nurture
- SLE, systemic lupus erythematosus
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- LUMINA, LUpus in MInority populations: Nature vs. Nurture
- SLE, systemic lupus erythematosus
As a chronic condition, systemic lupus erythematosus (SLE) can inflict considerable and sometimes irreversible morbidity that is reflected not only in the patients’ overall clinical status but also in their quality of life.1–5 As a result, patients may experience important functional limitations that can affect their activities of daily living and also their ability to work.6,7,8,9,10 As lupus tends to occur during the most productive years of life, these limitations contribute to the overall cost of the disease,11 at both the individual (patient and family) and societal levels.
Prior studies on work disability in patients with SLE have shown that about one third of the patients become disabled within 3–12 years of diagnosis.8,9,10 Strategies aimed at reducing work disability in these patients are therefore crucial. As predictors of work disability are likely to be multifactorial, a first step towards reducing its effect should be to identify potentially modifiable factors influencing its occurrence.
Using data from the Lupus in Minorities: Nature vs. Nurture (LUMINA) study, a multiethnic longitudinal cohort with SLE, we studied the factors predictive of self-reported work disability. We hypothesised that disease severity, along with some sociodemographic variables indicative of poor socioeconomic status, may affect the occurrence of work disability among patients with SLE.
PATIENTS AND METHODS
As described previously,12,13 LUMINA, established in 1994, is a longitudinal study of outcome in patients with lupus. All LUMINA patients meet the American College of Rheumatology (ACR) criteria for the classification of SLE,14,15 have disease duration ⩽5 years, are aged ⩾16 years, are of defined ethnicity (African American, Hispanic (from Texas and from the Island of Puerto Rico) and Caucasian) and live in the geographical recruitment area of the participating centres or their affiliated facilities (University of Alabama at Birmingham, University of Texas Health Science Center at Houston and University of Puerto Rico Medical Sciences Campus). These patients are, for the most part, referred for medical care and captured into LUMINA from either the inpatient or outpatient services of these university centres or their practices. About 90% of all patients referred for possible enrolment into LUMINA have agreed to participate; those who have refused to participate have been, in general, of sociodemographic and clinical features comparable to the ones recruited into the cohort. The institutional review board of each participating centre approved the LUMINA study; written informed consent was obtained from each participant according to the Declaration of Helsinki. At the time these analyses were conducted, 611 patients constituted the LUMINA cohort.
Before enrolment, all medical records were reviewed to confirm the patient’s eligibility and to gather socioeconomic–demographic and relevant clinical data from the time of diagnosis (TD) to enrolment (T0). Every patient had a baseline visit; follow-up visits are conducted every 6 months for the first year (T0.5 and T1, respectively) and yearly thereafter (T2, Tn). A LUMINA study visit consists of an interview, a physical examination and laboratory tests. Data for missed study visits are obtained, whenever possible, by a review of all available medical records. TD is defined as the time at which patients meet the four ACR criteria for the classification of SLE. Disease duration is defined as the interval between TD and T0, and follow-up time is defined as the interval between T0 and the last study visit (TL).
Work disability is defined by patients’ self-report of their inability to work; options to this question include whether the patient is a housewife, student, part-time worker, full-time worker, retired or disabled; these categories are mutually exclusive.
Variables
As described previously,16 the LUMINA database includes variables from the following domains: socioeconomic–demographic, clinical, immunological, genetic, behavioural and psychological. These variables are measured at T0 and at every subsequent visit. Only the variables included in these analyses are now described; excluded variables were those thought not to exert an immediate and direct effect on work disability (eg, genetic variables).
Variables from the socioeconomic–demographic domain included age, sex, ethnicity, education, poverty (as defined by the US Federal government adjusted for the number of people in the household),17 marital status, health-related behaviours (smoking, drinking, not exercising or using recreational drugs) and health insurance.
Clinical variables included the number of ACR criteria at TD, disease onset type (acute (accrual of four ACR criteria within 1 month) v insidious (accrual of four ACR criteria in >1 month)), disease duration, follow-up time, total disease duration (or the sum of both disease duration and follow-up time, or the time that elapsed between TD and TL), disease manifestations independent of the cause, disease activity and damage accrual, comorbidities, ancillary laboratory tests and drugs.
Disease activity was assessed using the Systemic Lupus Activity Measure—Revised18 at T0. The Systemic Lupus Activity Measure is a validated instrument, which includes 23 clinical manifestations and seven laboratory parameters present some time during the preceding month and attributable to SLE. Patients and doctors also grade disease activity using a 10-cm visual analogue scale, where 0 is no disease activity; 10 is the maximum disease activity possible. Patients complete the visual analogue scale at the time of their visits, whereas physicians complete theirs after the laboratory parameters were available.
Damage was measured with the Systemic Lupus International Collaborating Clinics Damage Index19 at T0 and TL. This index documents cumulative and irreversible damage irrespective of its cause in 12 different organ systems. To be scored, each manifestation must be present for at least 6 months, unless otherwise noted in the instructions accompanying this instrument.19
The following comorbidities were examined:
-
Diabetes mellitus (either self-reported or on the basis of doctor’s diagnosis or requiring pharmacological treatment)
-
Hypertension (defined as a systolic blood pressure ⩾140 mm Hg or diastolic blood pressure ⩾90 mm Hg on ⩾2 occasions, or patient’s self-reported intake of drugs for hypertension, regardless of the cause)
-
Myocardial infarction
-
Congestive heart failure
-
Obesity (defined as body mass index, calculated as weight (kg)/height2 (m2), ⩾30 kg/m2)
-
Depression
-
Cognitive impairment (defined by the presence of memory deficits or difficulty with calculation, spoken or written language or poor concentration as per the Cognitive Symptoms Inventory)20
-
Fibromyalgia (as per ACR criteria)21
All clinical manifestations were ascertained during the observation period—that is, until the occurrence of the event (work disability) or until TL if work disability had not been reported.
The following behavioural and psychological variables were examined:
-
Social support, ascertained with the Interpersonal Support Evaluation List, where higher scores indicate better social support22
-
Learnt helplessness or the perception that the patient can do nothing that will change his or her disease, ascertained with the Rheumatology Attitude Index, where higher scores indicate higher levels of helplessness23
-
Abnormal illness-related behaviours, ascertained with the Illness Behavior Questionnaire, where higher scores indicate more abnormal illness-related behaviours24
-
Self-reported health-related quality of life, ascertained with the Short Form-36 physical and mental component summary measures, where the mean (standard deviation) is 50 (10), higher scores indicate better function25
-
Fatigue ascertained with the Fatigue Severity Scale (FSS),26 where higher scores indicate more fatigue
-
Self-efficacy ascertained with the Arthritis Self-Efficacy Scale, an instrument that measures the extent to which people may successfully perform specific actions to attain health-related goals,27 where higher scores indicate greater confidence in a person’s ability to perform behaviours necessary to better control symptoms of SLE (arthritis replaced for SLE in this instrument)
-
Discrimination at work or getting a job, ascertained at each study visit with the work-related questions from the CARDIA VI questionnaire28
-
The level of pain, ascertained with a 10-cm visual analogue scale: 0, no pain; 10, maximum pain.
Statistical analyses
Only patients who were employed at T0 were included in these analyses. Work disability rates for these patients by ethnic group were estimated by the Kaplan–Meier method, and the differences between ethnic groups were examined by the log rank test. Features from the different domains were then compared between patients self-reporting and those not reporting work disability using descriptive statistical tests, Student’s t test for continuous variables and the χ2 test for categorical variables. Variables with p⩽0.10 in the univariable analyses were included in the multivariable analyses; age, sex and ethnicity were entered in all models. A time-dependent analysis (Cox’s proportional hazard regression model) was first examined, but the sample size was reduced further because of missing data for some of the variables. Thus, a logistic regression using a backward selection method was performed. Statistical significance in the regression was defined as p⩽0.05. All data were statistically analysed using SPSS V.10.0.
RESULTS
We studied 273 patients who were employed at T0. As expected, patients were predominantly women (90.5%) and of middle age (mean 36.5 (SD 12.4) years) Overall, 19.0% were Hispanics from Texas, 22.0% were Hispanics from Puerto Rico, 28.9% were African Americans and 30.0% were Caucasians. The mean (SD) total disease duration (TD–TL) was 4.7 (3.2) years; the median was 4.1 (range 0.4–13.2) years.
Work disability
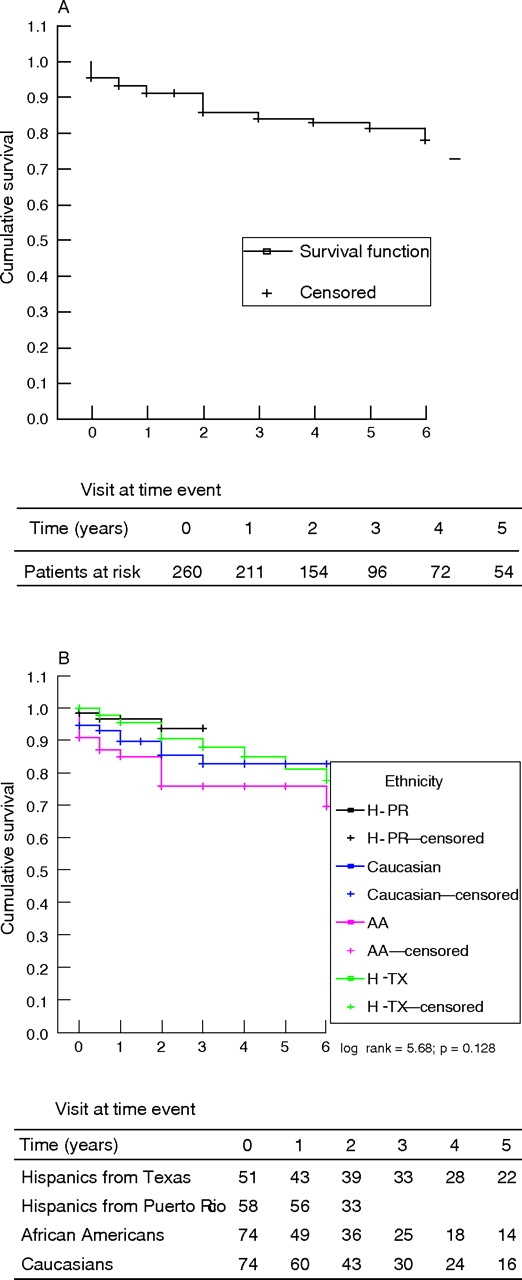
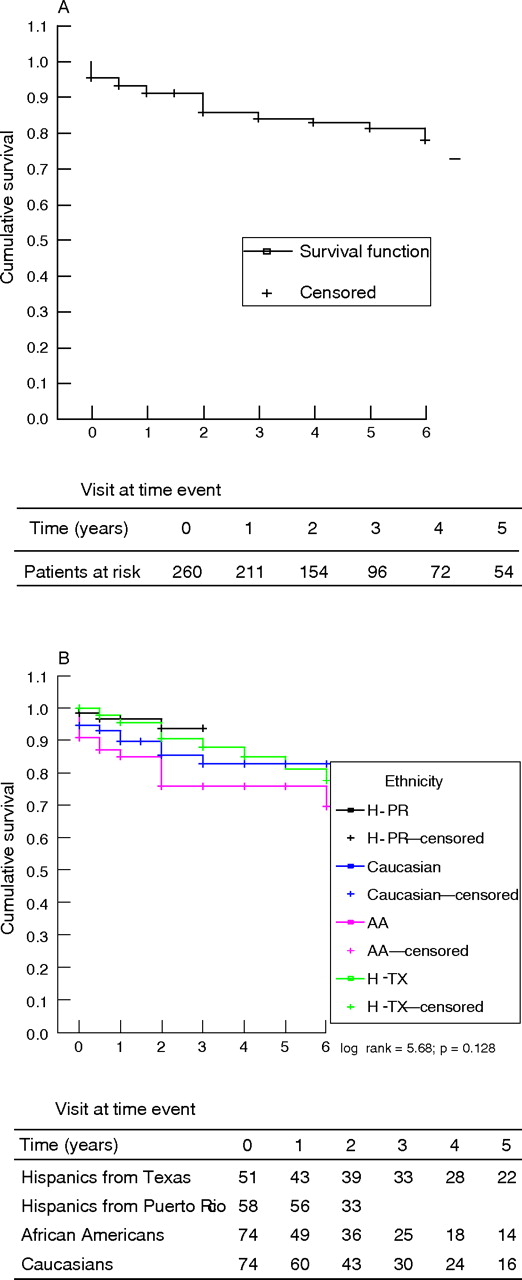
Of the 273 patients who were working at T0, 39 (14.3%) reported themselves as being work disabled sometime afterwards. The cumulative rate of self-reported work disability in the cohort as determined using the Kaplan–Meier method was 19% at 5 years. This rate was higher for African American patients (25%) than for the Hispanics from Texas (19%) and the Caucasians (18%). The 2-year rate of self-reported work disability for the Hispanics from Puerto Rico was 7%; data beyond this time point are not accurate for these patients as they were recruited into the cohort later than all others.13 The differences between these rates were not statistically significant whether or not the Hispanics from Puerto Rico were included (fig 1).
{kind=link}
Time to the occurrence of self-reported work disability in the LUMINA cohort: (A) entire cohort and (B) by ethnic group. H-TX, Hispanics from Texas (green line); H-PR, Hispanics from Puerto Rico (black line); AA, African Americans (purple line); and Caucasians (blue line).
Univariable analyses
Table 1 shows the distribution of selected baseline socioeconomic–demographic features for both categories of patients: work disabled and non-work disabled. Work disability occurred more frequently among men of either African American or Hispanic (from Texas) ethnicity. Work-disabled patients were also more likely to be poorer and less educated.
Baseline socioeconomic–demographic features of patients from the LUpus in MInority: Nature vs. Nurture cohort, according to their work disability status
Table 2 shows the cumulative clinical features. Patients with work disability tended to have longer disease duration and more renal involvement, whereas integument, musculoskeletal and haematological involvement were less frequent among them. They also had higher levels of disease activity, damage accrual and levels of pain. Depression was, however, less common among them. When only patients with renal involvement were examined, those who became disabled were more likely to be African American, below the poverty line and less educated, and to have less social support and coping skills, more disease activity, damage accrual, fatigue and lower levels of physical and mental functioning than those who did not become disabled (data not shown).
Cumulative clinical features of patients from the LUpus in MInority: Nature vs. Nurture cohort, according to their work disability status
Table 3 shows the baseline behavioural and psychological features for patients with and without work disability. Patients with disability showed higher levels of abnormal illness-related behaviours and helplessness, but lower levels of social support, self-efficacy, and self-reported physical and mental function. Self-perceived discrimination and fatigue occurred with comparable frequency in both groups.
Baseline behavioural and psychological features of patients from the LUpus in MInority: Nature vs. Nurture cohort, according to their work disability status
Multivariable analyses
Variables predictive of work disability were age (odds ratio (OR) 1.068; 95% confidence interval (CI) 1.018 to 1.119), male sex (OR 4.489, 95% CI 1.277 to 15.873), poverty (OR 2.860, 95% CI 1.167 to 7.004), total disease duration (OR 1.211, 95% CI 1.061 to 1.380), disease activity as per the Systemic Lupus Activity Measure—Revised (OR 1.248, 95% CI 1.129 to 1.379) and damage accrual as per the Systemic Lupus International Collaborating Clinics Damage Index (OR 1.362, 95% CI 1.115 to 1.663; table 4). Age and disease activity were also found to be significant in Cox’s model (data not shown).
Factors predictive of work disability by multivariable logistic regression analysis
DISCUSSION
Advances in medical care have changed the natural history of SLE from a disease with a high mortality to a more insidious chronic disease that can profoundly affect patients’ lives. This study confirms our hypothesis that disease-related factors (disease activity and damage accrual) and also socioeconomic–demographic factors influence the occurrence of work disability. Male patients with more severe disease in terms of disease activity and damage accrual but also older and with a more disadvantageous socioeconomic status (as reflected by poverty) were more likely to report work disability. Other variables that were significant in the univariable analyses, such as poor social support, self-efficacy and physical and mental function, higher level of helplessness and pain, and presence of renal involvement, were not retained in the multivariable regression analyses; yet they could be important determining factors in some patients.
Interestingly however, those patients with renal involvement who became disabled showed overall socioeconomic–demographic and clinical features comparable to all patients with disability. This probably explains why renal involvement was not retained in the multivariable model. Surprisingly, fibromyalgia and depression were either absent or occurred less frequently among the disabled patients than in the non-disabled ones, given our experience with these patients in the clinical setting; we do not have a good explanation for our findings.
Few other studies have focused on measuring the extent and factors predictive of work disability among patients with SLE, although disease activity and less years of education were also identified by Partridge et al.8 In terms of the proportion of patients disabled at a given time period, our figure is lower than those reported by Partridge et al,8 Stein et al9 and Yelin et al.10 In Yelin et al’s study, however, disease duration was much longer, about 12 years, and a 5-year estimate was not provided. Not surprisingly, these proportions are higher than those reported for the general population (10% of the 1998 working-age US population had a disability that prevented or limited work).29
The overall probability of patients becoming disabled was 19%, and was higher among African American patients than among those from other ethnic groups; however, the differences between the rates observed were not significant in the survival analyses and ethnicity was not retained in the multivariable analyses. Instead, poverty, which in our cohort was highly associated with this ethnic group, contributed independently to the model. Also, African American patients have been consistently shown to experience more damage accrual and disease activity, variables also independently contributing to work disability in our analyses.13,30,31
On average, the monthly benefit of a worker with disability in the US is almost US$900.00.32 As life expectancy has increased, the number of people with disability in the US has exponentially increased from about 15 000 by 1970 to 9 000 000 by 2003.32 Although the ageing of the population may partially explain this increase, it alone may not be a sufficient justification. An additional explanation may be that being declared “disabled” entitles people to receive benefits, an entitlement that was amended to include a broader definition of disability and covered the population of 1965.33 This increase is expected to have occurred uniformly across those with different chronic conditions, lupus included.34 Therefore, measures aimed at preventing or reverting work disability should be directed towards those patients at high risk of becoming work disabled. Moreover, research is needed to elucidate the effect of specific interventions in employment outcomes in patients with SLE.35 For example, research on other rheumatic diseases, specifically rheumatoid arthritis, has shown that a prompt induction of disease remission translates into the patients’ ability to remain employed.36
Our study is not without limitations.
-
The LUMINA cohort is a primarily tertiary care-based and hospital-based population, which may not be representative of the overall population with lupus. However, this is the first report on work disability among a multiethnic cohort in which two subgroups of Hispanic patients are included.
-
We could not include patients reporting themselves as being disabled at the baseline visit because our database lacked information on previous employment status; possibly, some of these patients may have been disabled before the diagnosis of SLE. Omitting these patients may have resulted in an underestimation of the rates of work disability in our patients. In fact, if all patients are considered, the overall rate reached 40% (data not shown), although this is, with all likelihood, an overestimation.
-
We may have included patients with only transient disability as “disabled”, as we had chosen the end point for these analyses as “becoming disabled”.
-
The questionnaire used to ascertain disability did not include attribution, and thus we were unable to state whether lupus was the underlying reason for patients becoming disabled.
-
We did not have information on the proportion of patients receiving disability benefits among those who self-reported work disability.
-
We did not calculate the indirect costs associated with being work disabled, as this information was not part of our database.
-
We were unable to ascertain work-related characteristics such as work status, satisfaction and earnings that may be associated with work disability, as these data were not part of the database. However, a related construct, discrimination, was not found to be related to work disability.
-
Our findings may not be generalisable to other developed countries, given that their socioeconomic–demographic characteristics (eg, socialised medicine) are quite different from those of the US.
CONCLUSION
About one sixth of the patients from a multiethnic cohort with lupus, who were know to be working at entry into the cohort, reported being work disabled. A less favourable socioeconomic background and a more severe disease are strong predictors of this occurrence. If work disability is to be prevented, patients at high risk need to be identified from the outset and treated aggressively, hoping that organ-system damage does not occur and also that its corollaries, disability included, do not ensue. Direct medical interventions have no effect in terms of abating poverty; yet, providing patients from disadvantageous socioeconomic background with the required social services may diminish its consequences. The toll imposed by SLE at the individual and societal levels may then be substantially reduced.
REFERENCES
Footnotes
-
Published Online First 30 June 2006
-
Funding: This study was supported by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases R01-AR42503 and General Clinical Research Centers M01-RR02558 (UTH-HSC) and M01-RR00032 (UAB); the National Center for Research Resources (NCRR/NIH) RCMI Clinical Research Infrastructure Initiative (RCRII) award 1P20RR11126 (UPR-MSC); and The Mary Kirkland Scholars Award Program and Fellowship from PANLAR and Rheuminations (UAB).
-
Competing interests: None declared.