Article Text

Abstract
Objectives To describe how inflammation on MRI of the sacroiliac joints in patients with recent-onset inflammatory back pain (IBP) evolves over time, and to study determinants of activity on MRI of the sacroiliac joint.
Methods A 2-year follow-up study with annual MRI of the sacroiliac joints was conducted in patients with IBP of less than 2 years' duration. Images were scored for bone marrow oedema on short τ inversion recovery and enhancement after administration of gadolinium on T1.
Results Of the 68 patients (38% male; mean age 34.9±10.3 years) enrolled, 44 had a negative baseline MRI. Of these 44 patients, 39 patients had at least one follow-up MRI of whom six patients (15%) developed activity on MRI during follow-up. 24 patients (35%) had an abnormal MRI at baseline. In 23 of these 24 patients follow-up MRI was available. The MRI became negative in seven of these 23 patients (30%) during follow-up. Human leucocyte antigen B27 (HLA-B27) positivity and male gender determined independently the likelihood of a positive MRI at any time point. In an HLA-B27-positive patient the likelihood of a positive MRI during follow-up is 88% if the baseline MRI is positive and 27% if the baseline MRI is negative. In an HLA-B27-negative patient with a negative MRI at baseline the likelihood of a positive MRI during follow-up is less than 5%.
Conclusions A positive MRI at baseline predicts a positive MRI during follow-up in HLA-B27-positive patients. A negative MRI at baseline in HLA-B27-negative patients strongly predicts a negative MRI during follow-up.
Statistics from Altmetric.com
The concept of spondyloarthritis covers a family of seronegative rheumatic disorders that share distinct clinical and genetic characteristics. General symptoms include inflammatory back pain (IBP), peripheral arthritis, enthesitis, dactylitis and anterior uveitis. Ankylosing spondylitis (AS) is the prototype of spondyloarthritis with predominant axial involvement.1 2 Other subtypes of spondyloarthritis are characterised by predominant peripheral involvement, such as psoriatic arthritis. To classify patients with spondyloarthritis, several criteria sets are available. These are the European Spondyloarthropathy Study Group criteria and Amor criteria for spondyloarthritis and the modified New York criteria specifically for AS.3,–,5 A new criteria set for classifying axial spondyloarthritis has recently been developed, mainly because available classification criteria were considered too insensitive, especially in early and mild disease.6 Although not intended for this purpose, classification criteria are frequently used in daily practice. As a consequence, the diagnosis of AS is often delayed for 10 years, because according to modified New York criteria sacroiliitis should be demonstrated on a conventional radiograph, which is a relatively late feature of the disease.7
MRI can play an important role in the non-radiographic stage of axial spondyloarthritis. It has been shown that MRI can detect the early inflammatory stages of sacroiliitis, months to years before structural damage can be detected on a conventional radiograph.8
Although activity (inflammation) detected on MRI is considered an important manifestation in early spondyloarthritis, there is still uncertainty about how activity on MRI evolves over time. MRI follow-up studies in patients with a short duration of symptoms are limited. Oostveen et al8 suggested that chronic changes on radiographs are preceded by inflammatory lesions on MRI. More recently, Bennett et al9 showed that both severe sacroiliitis on MRI at baseline as well as human leucocyte antigen B27 (HLA-B27) positivity predict the development of abnormalities on radiographs 8 years later. It is, however, unclear whether activity in the sacroiliac joints as seen on MRI is stable over time, becomes quiescent after an initial period of activity, or fluctuates over time. More knowledge about this is important with regard to the reliability of the new Assessment of SpondyloArthritis Society (ASAS) classification criteria in which activity on MRI is considered one of the entry criteria. Furthermore, it is extremely important for clinical practice to know if one single MRI is sufficient or that it is necessary to repeat the MRI in certain patients during the diagnostic process.
The aim of the present paper is to describe the evolution of active changes on MRI of the sacroiliac joints in a group of patients presenting with IBP of short duration who were followed for 2 years with repeated MRI.
Patients and methods
Design and study population
Patients with IBP of less than 2 years' duration were included in the Early Spondyloarthritis Cohort (ESpAC) study. The details of this study have been described previously.10 In brief, IBP was defined according to the Calin criteria, and was considered present if four out of five of the following criteria were present: onset of back pain before the age of 40 years with a persistence of at least 3 months; insidious onset; association with morning stiffness and improvement with exercise.11 Patients who fulfilled only three out of five of the Calin criteria but reported night pain were also included in ESpAC. The presence of other common spondyloarthritis features as defined in the European Spondyloarthropathy Study Group criteria, such as a positive family history, anterior uveitis or a history of psoriasis or inflammatory bowel disease, was preferred but not mandatory.
The study was designed as a prospective cohort study that consisted of three identical clinical and radiological examination rounds performed at baseline and after 1 and 2 years. Data obtained at baseline have been published previously.10 12 13
The study was approved by the institutional review board and all patients have provided written informed consent.
MRI
MRI of the sacroiliac joints was obtained with a 1.5 Tesla Philips Gyro Scan ACS-NT (Philips, The Netherlands). Patients were examined in a supine position with their knees bent. The following sequences were used in an oblique coronal orientation: T1-weighted spin echo (SE), short τ inversion recovery, T2-weighted fast SE with fat saturation and T1-weighted SE with fat suppression after administration of the intravenous contrast agent gadolinium diethylenetriaminepentate (Gd-DTPA; 0.1 mmol/kg body weight). The slice thickness was 4 mm with intervals of 0.4 mm. The matrix was 512 for the T1 fat suppression post-Gd-DTPA sequence and 256 for the remaining sequences. The MRI of each patient were scored as one set with random time sequence, by one experienced radiologist (AGJ), who was blinded to clinical, laboratory and radiographic results.
The magnetic resonance images were scored using a combination of the Spondyloarthritis Research Consortium of Canada (SPARCC) method and a modified version of the Aarhus MRI scoring method.14 15 The sacroiliac joints were divided into four quadrants: upper iliac; lower iliac; upper sacral and lower sacral. In contrast to the original SPARCC system, there was no maximum to the number of evaluated slices, in order to maximise the detection of abnormal magnetic resonance findings. The total number of evaluated slices in individual patients remained stable. Inflammation in the cartilagenous part of the joint was scored per slice in a dichotomous manner (present vs absent). Both subchondral bone marrow oedema and enhancement after administration of Gd-DTPA were scored. Bone marrow oedema was defined as areas of increased signal intensity on short τ inversion recovery images compared with normal bone marrow. Its presence was estimated in each of the four quadrants. Lesions extending at least 1 cm from the joint space or demonstrating high signal intensity comparable to that of spinal fluid were given an additional score on a per joint and per slice basis.
Subchondral enhancement was defined as areas of increased signal intensity compared with normal bone marrow on post-Gd-DTPA images. Scoring was comparable with scoring oedema, including additional scores for depth and high signal intensity comparable to enhanced vessels, respectively.
An MRI was considered positive for active sacroiliitis according to the ASAS/Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) MRI working group definition: the presence of at least one active lesion in at least two successive slices or the presence of more than one lesion in only one slice, which is highly suggestive of sacroiliitis.16
Statistical analysis
The MRI scores were analysed and described in three different manners. First, we described the MRI status over time (positive or negative). Second, we have investigated the likelihood of having a positive MRI at any time during follow-up, as well as factors determining MRI positivity, making use of generalised estimating equation (GEE) analysis for binomial outcome variables, with MRI status as a dependent variable, and HLA-B27 status and gender as independent explanatory variables. The contribution of C-reactive protein (CRP) in explaining a positive MRI was tested by adding CRP in the model as a covariate. GEE is an appropriate technique to study time trends in datasets with missing values while adjusting for within-patient correlation. Third, we have investigated the likelihood of finding a positive MRI if the baseline MRI is either negative or positive.
SPSS software version 15.0 was used for all descriptive statistics and the GEE analysis. All p values were two-tailed and statistical significance was set at the 0.05 level.
Results
Patient characteristics
In total, 68 patients with IBP were included in this study. Baseline characteristics are shown in table 1. Details of these patients have been described previously.10 Ninety-seven per cent of all patients fulfilled at least four out of five Calin criteria. Almost half of the patients were HLA-B27 positive. Anterior uveitis and inflammatory bowel disease were reported in 10 (15%) patients each, and 16 (24%) patients had a history of psoriasis. Twenty-five patients had a positive family history for AS. Table 1 also provides information about the 44 patients who completed the 2-year follow-up. These patients did not differ from the complete group at baseline.
Baseline characteristics of 68 patients included in the ESpAC study
MRI findings
MRI of the sacroiliac joints was performed in all patients at baseline. Sixty-two patients had at least one follow-up MRI after 1 or 2 years follow-up and 44 patients completed all three examinations. Table 2 shows the MRI status (positive or negative) at baseline according to the ASAS/OMERACT MRI working group definition as well as how these findings develop over time.
MRI status over time according to the ASAS/OMERACT MRI working group definition in 68 patients with early inflammatory low back pain who were included in the ESpAC
In total, 44 patients (65%) had a negative MRI at baseline, of which 15 patients (34%) were HLA-B27 positive. Of these 44 patients, 39 (89%) completed either one or two follow-up MRI. In six of these 39 patients (15%), the MRI became positive at 1 or 2 years follow-up. In one HLA-B27-positive patient of these six patients the MRI remained positive at 2 years follow-up, in one HLA-B27-negative patient the MRI became negative again at 2 years follow-up, in two HLA-B27-negative patients the MRI became positive at 2 years follow-up and in two HLA-B27-positive patients no MRI were available at 2 years follow-up.
Twenty-four patients (35%) had a positive MRI at baseline, of which 16 (66%) patients were HLA-B27 positive. In total, 23 of these 24 patients completed either one or two follow-up MRI. The MRI became negative in seven of these 23 patients (30%) during follow-up at one or at both assessments. Five of these seven patients were HLA-B27 negative, and in three of them the MRI was only weakly positive at baseline. In the remaining two patients, a strongly positive MRI was detected at baseline, but the MRI became negative during follow-up. In two HLA-B27-positive patients with a negative MRI at 1 year follow-up, the MRI was positive again at 2 years follow-up.
Factors determining a positive MRI
In the GEE analysis, both male gender (OR 3.0, 95% CI 1.1 to 8.2, p=0.035) and HLA-B27 positivity (OR 5.1, 95% CI 1.9 to 13.6, p<0.001) independently determined the likelihood of a positive MRI at any time point. CRP did not contribute to explaining variation in the model. The effects of these determinants are visualised in an absolute manner in figure 1, showing that the likelihood of a positive MRI in HLA-B27-negative women with IBP is only approximately 10% compared with HLA-B27-positive men with IBP in whom this likelihood is close to 70%.

Likelihood of a positive MRI at any time point in patients with short-standing inflammatory back pain assessed at baseline, 1 year and 2 years of follow-up in function of HLA-B27 status and gender. HLA-B27, human leucocyte antigen B27.
Likelihood of a positive MRI during follow-up
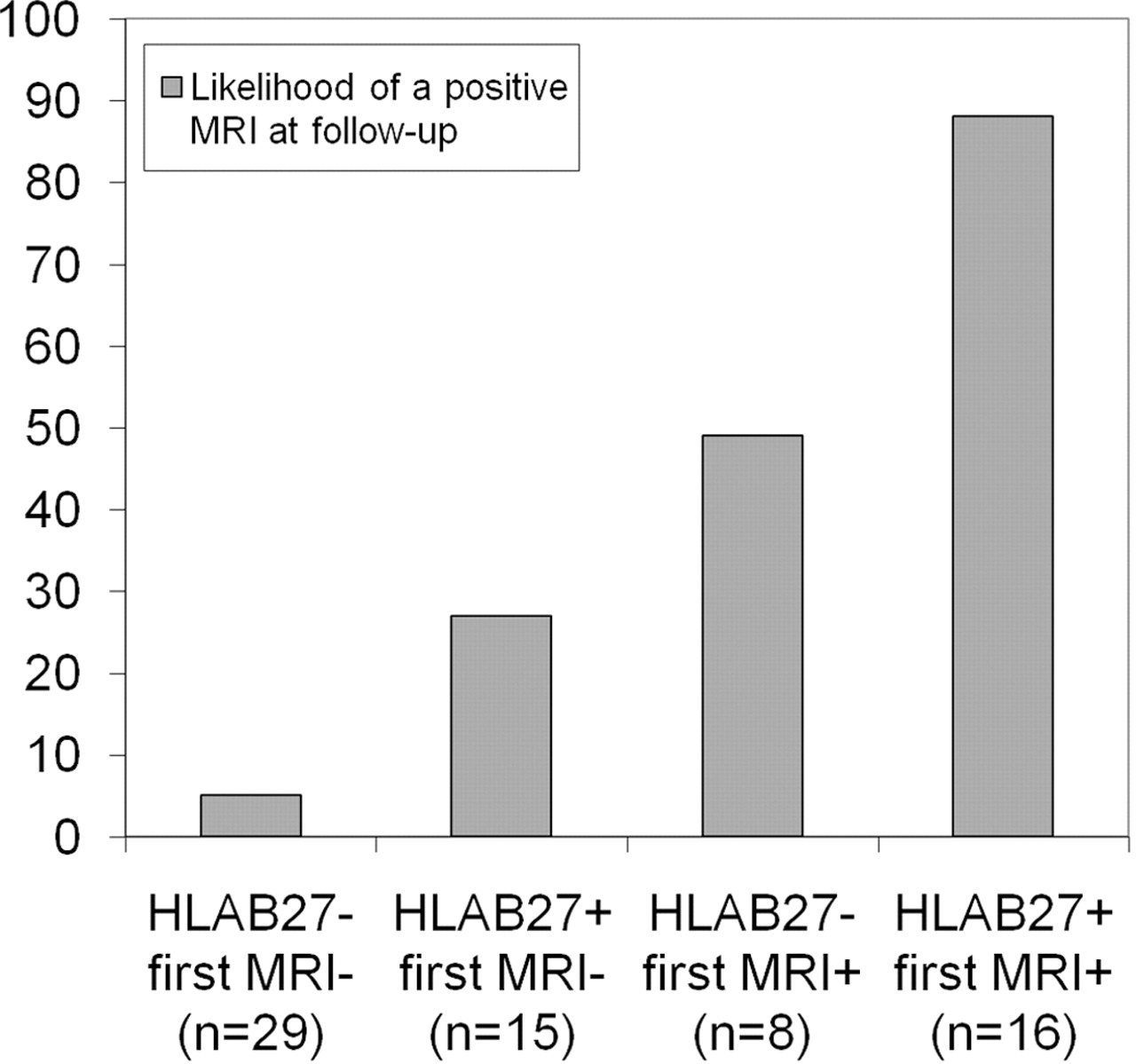
The likelihood of finding a positive MRI if the baseline MRI is either negative or positive was also investigated. Both HLA-B27 status (OR 8.1, 95% CI 2.3 to 28.3, p<0.001) and MRI status at baseline (OR 22.0, 95% CI 6.1 to 79.6, p<0.001) appeared to be strongly and independently contributory to a positive MRI of the sacroiliac joints over time. Figure 2 shows the likelihood of a positive MRI in relation to HLA-B27 status. The likelihood of a positive MRI is negligible (<5%) in the case of an HLA-B27-negative patient with a negative MRI at baseline. The likelihood is close to 90% in the case of an HLA-B27-positive patient with a positive MRI at baseline. The likelihood is intermediate in patients with either HLA-B27 positivity but a negative MRI at baseline (27%) or a positive MRI but negative HLA-B27 status at baseline (49%).

{kind=link}
{kind=link}
Likelihood of a positive MRI at 1 year or 2 years of follow-up in patients with short-standing inflammatory back pain assessed at baseline, 1 year and 2 years of follow-up, in function of the result of the baseline MRI (negative or positive) and HLA-B27 status. HLA-B27, human leucocyte antigen B27.
Discussion
In this cohort of patients with early IBP, almost two-thirds of the patients had a negative MRI at baseline. Interestingly, in only a minority of these patients (15%), the MRI status changed during follow-up. A negative MRI at baseline in combination with a negative HLA-B27 status had a likelihood of 95% of finding a negative MRI in the next 2 years. This finding may be of clinical relevance, because it suggests that in HLA-B27-negative patients with a negative MRI sacroiliitis can be excluded with a high level of certainty.
A similar conclusion can be drawn from the group of patients with a positive MRI. One can conclude that if sacroiliitis is detected by MRI, there is a high likelihood that sacroiliitis remains present in HLA-B27-positive patients (88%). This finding therefore adds to the credibility of MRI as a pivotal measure in the axial spondyloarthritis criteria. It is of note that there was no use of biological agents in this cohort of patients with early IBP during this 2-year period.
In general, both male gender and HLA-B27 positivity independently determined the likelihood of a positive MRI at any time point. This is not surprising, because spondyloarthritis and in particular AS is strongly associated with HLA-B27 and has an overall male predominance. In this study it was found that HLA-B27-positive male patients with IBP have the highest chance of a positive MRI at any time.
It is now well recognised that MRI is superior to conventional radiography in diagnosing early spondyloarthritis. However, insight into the evolution in MRI findings in patients with early spondyloarthritis and sacroiliitis is limited, because follow-up studies are scarce. To our knowledge, this is the first study in patients with early IBP with three successive MRI examinations spanning 2 years of follow-up. Puhakka et al17 performed a 1-year follow-up study to describe changes in MRI findings of the sacroiliac joints in 34 patients with spondyloarthritis of recent onset. In this study, 30 out of 34 patients already had signs of inflammation on their MRI at baseline, which is a higher proportion than in our cohort. Results from this study showed that the general MRI activity score did not change at 1 year; however, bone marrow oedema decreased significantly during follow-up.
The MRI scoring method used in the present study is a combination of the published SPARCC and the Aarhus grading methods.14 15 Both systems have proved to be reliable and reproducible. With the SPARCC scoring method, a maximum of six consecutive slices is evaluated. Instead, we chose to score the entire sacroiliac joint on all qualitatively optimal slices. This was done to maximise the detection of active lesions. In practice, it implied that in the majority of patients between five and eight slices were evaluated, while taking care that the same (number of) slices was scored per patient over time. The scoring of active lesions was done dichotomously as by the SPARCC method. Due to the unlimited number of slices evaluated, the present scoring method demands magnetic resonance scans of the same anatomical area of each patient examined at follow-up to secure that scoring starts and ends at the same anatomical level. This may cause some limitation of the method if the technique for obtaining oblique coronal slices is not standardised. With a scoring based on both oblique coronal and axial slices this problem does not exist as the sacroiliac joints then can be evaluated three-dimensionally.18
The present study has several limitations that need to be acknowledged. Although we had MRI of all patients at baseline, a substantial number of MRI was missing at one or at both follow-up visits. Missing data may have influenced the results, because it is possible that patients with missing MRI represent a proportion of patients in whom the symptoms that made them eligible for inclusion in the ESpAC study have disappeared. Although such a bias cannot be excluded, GEE adjusts to some extent for such spurious effects, by adjusting for within-patient correlation and not excluding patients with missing time points. Another limitation of this study is that the MRI sets were scored by one reader. However, the scoring system used in the present study uses a combination of scoring systems that have already proved to be reliable with respect to inter-reader agreement.19 A general issue regarding assessment of MRI of the sacroiliac joints is that in a previous study in up to 30% of the sacroiliac joints of individuals with chronic low back pain or healthy controls abnormalities were detected.20 Such lesions may have contributed to some extent to the results we have found, but it is likely that these abnormalities will disappear in non-inflammatory conditions over time in contrast to male patients with IBP whp are HLA-B27 positive. At last, the ESpAC cohort in which the analyses were performed is a rather small cohort with characteristics that do not necessarily resemble the average patient presenting with complaints suggestive of spondyloarthritis. Extrapolation of findings should therefore be done cautiously.
In conclusion, MRI is a very useful imaging technique in establishing inflammation in the sacroiliac joints, and may contribute to making a diagnosis of axial spondyloarthritis in patients with IBP. In this cohort of patients with IBP of recent onset, it seems that during a 2-year follow-up period, the proportion of patients with and without signs of MRI activity remains stable to a great extent. This is an important finding, because it suggests that in the case of both a negative MRI and a negative HLA-B27 status, a classifying diagnosis of axial spondyloarthritis can be excluded with great certainty. In this cohort we found that the combination of a positive MRI scan and HLA-B27 positivity is associated with a high likelihood of a persistent positive MRI during follow-up. In HLA-B27-positive patients with a negative MRI at baseline, in whom a classifying diagnosis of axial spondyloarthritis cannot be made by the route of HLA-B27 presence plus two additional spondyloarthritis features, a follow-up MRI can be considered because a reasonable proportion of these patients will develop MRI activity over time, especially in male patients.
References
Footnotes
-
Funding This study was partly supported by a grant from the Dutch Arthritis Association.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review board (Maastricht).
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.