Article Text

Abstract
Objectives To assess the impact of abatacept on sleep quality in patients with rheumatoid arthritis (RA), and the validity of the sleep disturbance scale of the Medical Outcomes Study Sleep Questionnaire (MOS-Sleep).
Methods Data from two randomised, double-blind, placebo-controlled abatacept trials (Abatacept Trial in Treatment of Antitumor necrosis factor IN adequate responders (ATTAIN) and Abatacept in Inadequate responders to Methotrexate (AIM)) were analysed. Sleep quality was assessed using the MOS-Sleep. Changes in the Sleep Disturbance Scale were assessed according to clinical responses (including American College of Rheumatology (ACR) and Disease Activity Score 28 C-reactive protein criteria). Correlations between sleep disturbance and patient-reported outcomes were assessed. The sensitivity to change of sleep disturbance was assessed by calculating the standardised response means (SRMs).
Results 258 abatacept- and 133 placebo-treated patients in ATTAIN and 433 abatacept- and 219 placebo-treated patients in AIM were analysed. In ATTAIN, mean improvements to month 6 were significantly greater for patients treated with abatacept than for placebo patients in sleep disturbance (11.3 vs 2.9, p<0.001), sleep adequacy (9.0 vs 0.6, p<0.05), somnolence (10.5 vs 1.6, p<0.001) and Sleep Problems Index (SPI) I (9.5 vs 1.4, p<0.0001) and II (9.8 vs 2.1, p<0.001); mean improvements in AIM to year 1 were statistically significant for sleep disturbance (12.9 vs 8.9, p<0.05) and SPI I (9.4 vs 6.7, p<0.05) and II (10.4 vs 7.3, p<0.05). Associations between mean improvements in sleep disturbance and clinical responses were statistically significant (3.8, 12.7, 18.0, p<0.001 and 5.0, 11.5, 15.7, p<0.001 for European League Against Rheumatism responses, none, moderate and good in ATTAIN and AIM, respectively; 10.2, 14.4, 22.8, p=0.007 and 10.9, 14.9, 17.7, p=0.006 for ACR 20, 50 and 70 responses in ATTAIN and AIM, respectively). SRMs for sleep disturbance were 0.38 (ATTAIN) and 0.19 (AIM).
Conclusions Abatacept treatment provides significant improvements in multiple aspects of sleep in patients with RA. The Sleep Disturbance Scale of the MOS-Sleep shows validity, reliability and sensitivity to change.
Statistics from Altmetric.com
Introduction
Patient-reported outcomes (PROs) provide an assessment of health, wellbeing and treatment response from the patient's perspective, and provide information about aspects of disease that are not captured by standard clinical assessments. These outcomes can provide valuable information about improvements in health-related quality of life (HRQoL) that are important to the patient and, in turn, may influence other factors, such as adherence to treatment. One important patient-reported aspect of health and wellbeing is quality of sleep. Sleep quality has been identified as a key concern for patients with rheumatoid arthritis (RA),1 and its importance has been identified by the Outcome Measures in Rheumatology Clinical Trials group.2 3 However, it is often not taken into consideration by treating doctors and is not encompassed by the current ‘core set’ of outcome measures. Chronic conditions, such as RA, can adversely affect sleep quality; pain and other consequences of inflammation negatively impact the quality of sleep experienced by patients with RA and, conversely, disturbances in sleep can contribute to and exacerbate, feelings of pain, fatigue and stiffness,4 5 and stress.6 Given that sleep quality can have such a significant role in the quality of life of patients with RA, it is informative to assess the impact that treatments for RA have on sleep quality. Despite this, the impact of RA treatment on sleep quality is not often reported in clinical trials.7
Sleep is multidimensional and the Medical Outcomes Study Sleep measure (MOS-Sleep)8 is a validated instrument used to measure different aspects of patient-reported sleep problems. The MOS-Sleep has been used across a range of diseases (including diabetic neuropathy9 and fibromyalgia10), and it was ranked highly for both psychometric properties and feasibility in a recent review of sleep instruments for patients with RA.11 Within the MOS-Sleep measure, the specific dimension of sleep disturbance has been identified by patients and researchers as a particularly important aspect of sleep quality: a recent study in patients with RA showed that two of the primary areas covered by the Sleep Disturbance Scale (sleep initiation and sleep maintenance) table 1) were ranked very highly.11 This central role for sleep disturbance is reflected in the recent proposal to include sleep disturbance in a core set of measures of PROs for the assessment of patients with RA.1 Although sleep disturbance is clearly a key aspect of sleep quality in patients with RA, the psychometric properties of the Sleep Disturbance Scale have not previously been validated in this patient population.
Derived sleep scales of the MOS-Sleep measure
The first objective of this analysis was to investigate which aspects of sleep improve when patients with RA are treated with abatacept, a selective T-cell co-stimulation modulator which has previously demonstrated benefits in patients with RA across a range of clinical efficacy measures.12 13 The second objective was to use abatacept clinical trial data to determine the validity, reliability and sensitivity to change of the Sleep Disturbance Scale of the MOS-Sleep measure.
Methods
Datasets
The ATTAIN (Abatacept Trial in Treatment of Antitumor necrosis factor (TNF) IN adequate responders) trial was a 6-month, phase III, multicentre, randomised double-blind, placebo-controlled trial of abatacept in patients with active RA and an inadequate response to anti-TNF treatment.12 The AIM (Abatacept in Inadequate responders to Methotrexate (MTX)) trial was a 1-year, phase III, multicentre, randomised double-blind, placebo-controlled trial of abatacept in patients with active RA and an inadequate response to MTX.13 Patients were randomised 2:1 to receive abatacept or placebo on a background of at least one disease-modifying antirheumatic drug (in ATTAIN) or MTX (in AIM). The detailed study designs and efficacy and safety results of these trials have been published previously elsewhere.12 13 We performed analyses on data from the double-blind periods of these two trials (6 months for ATTAIN and 1 year for AIM) to assess sleep quality and investigate the psychometric properties of the Sleep Disturbance Scale. As the double-blind periods of these trials were of different lengths, analyses were also performed at the 6-month time point for the AIM trial.
Sleep assessments
Medical Outcomes Study Sleep Questionnaire
The 12-item MOS-Sleep measure is composed of 12 questions (table 1). For question one, patients were given five possible responses as follows: 0–15, 16–30, 31–45, 45–60 or >60 min. For question two, patients were required to report the actual number of hours. For the remaining questions, patients were given the following options: all, most, a good bit, some, a little, or none of the time. The score for each item was converted to a 0–100 range, with a higher score indicating more sleep problems.14 Scores for particular items were averaged together to create seven scales (table 1).14 For example, the Sleep Disturbance Scale is generated using the following questions: ‘How long did it usually take for you to fall asleep during the past 4 weeks?’; ‘How often during the past 4 weeks did you: (1) feel that your sleep was not quiet (moving restlessly, feeling tense, speaking etc, while sleeping)?; (2) have trouble falling asleep?; (3) awaken during your sleep time and have trouble falling asleep again?’. For sleep adequacy, an increase in score represents an improvement; for all other scales a decrease in score represents an improvement.
In addition, assessments were also performed for optimal sleep duration. Optimal sleep duration was recorded as a dichotomous variable with optimal sleep defined as 7–8 h,8 15 and 1–6 or 9–23 h classed as suboptimal. The change from baseline in the proportion of patients reporting optimal sleep was reported.
Assessments of the psychometric properties of the Sleep Disturbance Scale
If the Sleep Disturbance Scale accurately assesses changes in sleep disturbance associated with RA, these changes should correlate with changes in other measures of RA severity (ie, the Sleep Disturbance Scale should have ‘construct validity’). The construct validity of the Sleep Disturbance Scale was assessed by examining how well sleep disturbance scores reflect clinical response to treatment and disease status. Response to treatment was assessed using the American College of Rheumatology (ACR) criteria,16 and disease status was measured using the Disease Activity Score 28 (DAS28) C reactive protein criteria.17 European League Against Rheumatism (EULAR) response states were classified as good response (improvement of >1.2 and a present score of ≤3.2); moderate response (improvement of >0.6–≤1.2 and a present score of ≤5.1, or an improvement of >1.2 and a present score of >3.2); or no response (improvement of ≤0.6, or improvement of >0.6–≤1.2 and a present score of >5.1). A DAS28 score of ≤3.2 was defined as low disease activity state (LDAS), and a score of <2.6 was defined as remission.17 In addition to clinical measures of efficacy, the following PROs were assessed: patient global assessment, pain, Health Assessment Questionnaire Disability Index, activity limitation, fatigue and the physical and mental component summary scores of the Short Form-36 (SF-36) questionnaire.
The test–retest reliability of the Sleep Disturbance Scale was determined for a subset of patients who showed little or no change in disease activity, defined as <2% change in patient global assessment between the baseline and 1-month study time point (the first assessment after study initiation). The intraclass correlation between baseline and month 1 was calculated by determining Shrout–Fleiss reliabilities for this subset of patients for sleep disturbance.
The sensitivity to change of sleep disturbance was assessed by calculating the standardised response mean (SRM; the ratio of the treatment difference to the pooled SD of the mean change scores). By convention, an SRM of 0.2, 0.5 or 0.8 is considered as small, moderate or large, respectively,18 with a larger SRM representing a greater sensitivity to change.
Data analysis
The impact of abatacept on sleep was assessed by comparing the active and placebo arms in the ATTAIN and AIM trials separately. Analyses were based on the intention-to-treat population for patients with available data at the visit of interest (as observed). Mean improvements from baseline to the end of the double-blind period were compared using t tests, and the proportions of patients achieving optimal sleep were compared using χ2 tests. The construct validity of sleep disturbance was assessed using pooled as-observed data from the abatacept and placebo groups, for both trials combined. F tests and t tests were used to determine the statistical significance of the association between sleep disturbance change scores and these treatment response and disease state categories, and a χ2 test was performed to assess the linearity of these relationships. Spearman's rank correlation coefficient was used to assess the correlation between sleep disturbance PROs. To assess the test–retest reliability of sleep disturbance, the intraclass correlation between baseline and month 1 was calculated by determining Shrout–Fleiss reliabilities. SRMs for sleep disturbance were calculated according to the following formula:

Where ma and sa are the mean and SD respectively, of the change in scores from baseline in the abatacept group, and na is the number of patients in this group. Similarly, mc, sc, nc are the corresponding values for the control group.
Results
Baseline demographics and clinical characteristics
A total of 258 and 133 patients were randomised and treated with abatacept or placebo, respectively, plus at least one disease-modifying antirheumatic drug in the ATTAIN trial,12 and 433 and 219 patients were randomised and treated with abatacept or placebo, respectively, plus MTX in the AIM trial.13 A total of 218 and 99 patients, respectively, completed 6 months and entered the long-term extension period in ATTAIN, and 378 and 161, respectively, completed 1 year and entered the long-term extension period in AIM. Demographics and clinical characteristics at baseline (including the seven scales of the MOS-Sleep) were comparable between the abatacept and placebo groups for both datasets, and patients were predominantly female and Caucasian (table 2). Patients in the ATTAIN trial had a longer disease duration than those in the AIM trial (for the abatacept and placebo groups mean duration was 12.2 and 11.4 vs 8.5 and 8.9 years, respectively).
Baseline demographics and clinical characteristics
Impact of abatacept treatment on sleep quality
The actual mean values for each sleep scale at month 6 of the ATTAIN trial and year 1 of the AIM trial are presented in figure 1A, B, respectively. For the ATTAIN study, scores were comparable for all scales (∼35–42) except awakening with shortness of breath or headache, which was considerably lower (∼15 for both the abatacept and placebo groups; figure 1A). For the AIM study, scores were slightly lower but a similar pattern was observed with the exception of sleep adequacy, which was considerably higher (>50 for each group; figure 1B). Scores were similar when the AIM data were analysed at month 6 (online supplementary figure 1A).

Mean scores in each of the derived sleep scales of the MOS-Sleep measure. (A) The ATTAIN trial and (B) The AIM trial. *n=257 for sleep disturbance and Sleep Problems Index II, n=250 for snoring and n=253 for sleep SoB or headache; †n=125 for snoring; ‡n=447 for sleep disturbance and Sleep Problems Index II and n=438 for snoring; §n=216 for snoring and n=221 for sleep SoB or headache. AIM, Abatacept in Inadequate responders to Methotrexate; ATTAIN, Abatacept Trial in Treatment of Antitumor necrosis factor; MOS-Sleep, Medical Outcomes Study Sleep; SoB, shortness of breath.
For the ATTAIN study, mean improvements from baseline to month 6 in MOS-Sleep Scales were significantly greater in the abatacept than in the placebo group for sleep disturbance (p<0.001), sleep adequacy (p<0.05), somnolence (p<0.001) and Sleep Problems Index (SPI) I and II (p<0.001 for both; figure 2A). For the AIM study, mean improvements from baseline to year 1 were generally of a greater magnitude than the improvements observed over 6 months in the ATTAIN trial, but differences between the treatment arms were smaller in AIM, and were only statistically significant for sleep disturbance and SPI I and II (p<0.05 for each; figure 2B). Differences between abatacept and placebo for sleep adequacy and somnolence (which were statistically significant for ATTAIN) failed to reach statistical significance in the AIM study. Scores were similar when the AIM data were analysed at month 6, although the separation between treatment groups was less pronounced for some of the scales (notably sleep adequacy and somnolence and SPI I and II; supplementary figure 1B).

Mean improvements in each of the derived sleep scales of the MOS-Sleep measure. (A) The ATTAIN trial and (B) The AIM trial. *p<0.001; †p<0.05; ‡n=257 for sleep disturbance and Sleep Problems Index II, n=250 for snoring and n=253 for sleep SoB or headache; §n=125 for snoring; ¶n=447 for sleep disturbance and Sleep Problems Index II and n=438 for snoring; **n=216 for snoring and n=221 for sleep SoB or headache. AIM, Abatacept in Inadequate responders to Methotrexate; ATTAIN, Abatacept Trial in Treatment of Antitumor necrosis factor; MOS-Sleep, Medical Outcomes Study Sleep; SoB, shortness of breath.
For both studies, optimal sleep significantly improved in the abatacept versus control group. The proportion of patients reporting optimal sleep improved by 18% versus 12% from baseline to month 6 (p<0.001) in the ATTAIN trial. In the AIM trial, the proportion of patients reporting optimal sleep improved by 16% versus 5% from baseline to year 1 (p=0.021) and by 13% versus 3% from baseline to month 6 (p=0.020).
Psychometric properties of the Sleep Disturbance Scale
Construct validity
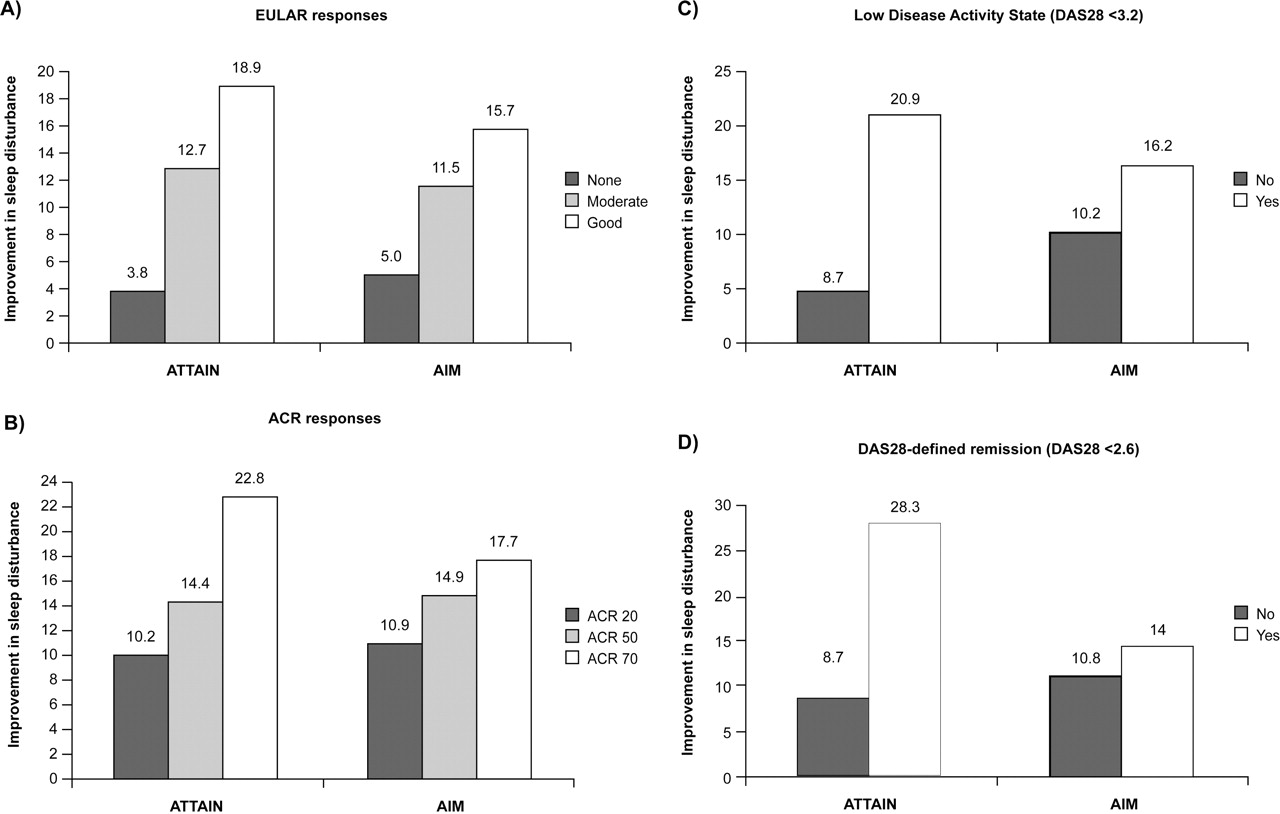
Improvements from baseline in sleep disturbance scores increased in a linear manner with improving treatment responses (figure 3A, B), from EULAR non-responders to moderate responders to good responders (p<0.001 for linear trend in both trials), and from ACR 20 to 50 to 70 (p=0.007 for linear trend in both trials). The association between improvements in the Sleep Disturbance Scale and responses to treatment were statistically significant (in ATTAIN, p<0.001 for EULAR responses and p=0.007 for ACR responses and in AIM, p<0.001 for EULAR responses and p=0.007 for ACR responses).

{kind=link}
{kind=link}
{kind=link}
Mean improvements in the Sleep Disturbance Scale of the MOS-Sleep according to clinical response to treatment or disease status. Response to treatment assessed by achievement of (A) a EULAR response (good, moderate or none) or (B) ACR response (ACR 20, 50 or 70). Disease status assessed by (C) achievement of LDAS (DAS28 ≤3.2) or (D) DAS28-defined remission (DAS28 <2.6; yes or no). ACR, American College of Rheumatology; DAS28, Disease Activity Score 28; EULAR, European League Against Rheumatism; LDAS, Low Disease Activity State; MOS-Sleep, Medical Outcomes Study Sleep.
There was also an association between improvements in sleep disturbance and measures of disease status. For DAS28-derived measures, the association was statistically significant for LDAS in the AIM trial (p=0.016; figure 3C); improvements were numerically higher for patients who achieved LDAS (in the ATTAIN trial) or DAS28-defined remission (in either trial) versus those who did not, but this did not reach statistical significance (figure 3C, D). A similar pattern was observed when treatment responses were examined at month 6 for the AIM trial (supplementary figure 2).
For patients in the ATTAIN and AIM trials, respectively, moderate correlations were found between sleep disturbance and fatigue (r=0.37 and r=0.31), activity limitation (0.35 and 0.27), patient global assessment (0.34 and 0.30), pain (0.36 and 0.31), Health Assessment Questionnaire Disability Index (0.31 and 0.32), physical component summary score (–0.23 and –0.29) and mental component summary score (–0.43 and –0.38). Again, similar patterns were observed when treatment responses were examined at month 6 for the AIM trial (supplementary table 1).
Reliability
A total of 59 patients (66% from AIM) showed little or no change in disease activity, defined as <2% change in patient global assessment. In this subset of patients, the Shrout–Fleiss reliabilities were 0.82 (single score), 0.82 (random set), 0.84 (fixed set), representing a high level of test–retest reliability for sleep disturbance.
Sensitivity to change
The SRM (95% CI) for sleep disturbance was 0.38 (0.17 to 0.60) in the ATTAIN trial and 0.19 (0.03 to 0.35) and 0.15 (0.02 to 0.28) at 1 year and 6 months in the AIM trial, respectively, indicating small effect sizes.
Discussion
In patients with RA and an inadequate response to anti-TNF treatment (the ATTAIN trial) or MTX (the AIM trial), abatacept significantly improved multiple aspects of sleep quality over 6 months or 1 year, respectively. In the ATTAIN trial, improvements were significantly greater in abatacept-treated than in placebo-treated patients for five out of the seven scales, including sleep disturbance, sleep adequacy, somnolence and SPI I and II. In the AIM trial, improvements were significantly greater than placebo for the scales of sleep disturbance and SPI I and II. The magnitude of the improvements from baseline seen with abatacept were generally comparable or slightly greater for patients in the AIM trial than in the ATTAIN trial, which may be attributed to the higher disease activity in patients entering ATTAIN. Interestingly, improvements observed in the placebo group in the AIM trial were markedly greater than those seen in the placebo group in the ATTAIN trial, which may account for the smaller effect size, resulting in fewer scales reaching statistical significance in AIM. Although not statistically different from the placebo group, the magnitude of improvements were greatest in the sleep adequacy scale in the AIM trial, with mean scores approaching those previously reported for the general population.19
Across both trials, improvements in the Sleep Disturbance Scale and SPI I and II were significantly greater for abatacept-treated patients. It should be noted that these three scales of the MOS-Sleep encompass the widest range of items from the 12-item MOS-Sleep measure and are, therefore, likely to give a more complete picture of the overall sleep quality experienced by patients. For example, SPI II covers areas including trouble falling asleep, time taken to fall asleep, sleep restlessness, awakening during sleep, awakening short of breath or with headache, whether enough sleep to feel rested was obtained, whether the amount of sleep needed was obtained, feelings of drowsiness and trouble staying awake. In further support of this, Hays and Stewart8 demonstrated that these three scales showed the greatest correlation with other HRQoL measures, including assessments of pain and physical function. In addition to these scales of the MOS-Sleep, the proportion of patients achieving ‘optimal sleep duration’ of 7–8 h was significantly greater in abatacept-treated than in placebo-treated patients in both trials. Suboptimal sleep duration (more or less than 7–8 h) has been associated with increased levels of disability, worse signs and symptoms of disease and a higher mortality risk.8
For both of the datasets analysed here, the greatest magnitude of improvement from baseline observed in the MOS-Sleep Scales was for sleep disturbance. Sleep disturbance is recognised as a key component of sleep quality, and is one of the criteria of the EULAR Rheumatoid Arthritis Impact of Disease composite index.1 In addition to examining the impact of abatacept treatment on a variety of aspects of sleep quality in the AIM and ATTAIN trials, we used these datasets to investigate the psychometric properties of the Sleep Disturbance Scale. The Sleep Disturbance Scale demonstrated construct validity against a range of measures of clinical efficacy based on the ACR and DAS28 criteria; patients who experienced improvements in Sleep Disturbance Scale assessments also demonstrated improvements across this range of clinical efficacy measures. In addition, associations were observed between sleep disturbance and a variety of other PROs. The reliability and sensitivity to change of this sleep dimension were also confirmed. The SRMs fell within the range of those previously reported for the mental components of the SF-36,18 although the effect size of the SRM was relatively low in AIM compared with the moderate effect size observed in ATTAIN. This difference may be a result of the larger placebo effect observed in AIM, and differences in disease severity at baseline between the two trials may also have a role.
Sleep quality is perceived as a central component of HRQoL by patients with RA,2 3 and is a symptom of disease that is not dealt with adequately by current clinical assessments. There also appears to be a dynamic interplay between sleep quality and other aspects of RA, including pain, stiffness and fatigue.4,–,6 This is the first time that the impact of treatment on sleep quality has been extensively explored in a large-scale clinical trial of patients with RA. Given the importance of sleep quality to the patient, it is highly relevant to include sleep quality assessments when evaluating the efficacy of treatments for RA, and this aspect of treatment efficacy should be given greater consideration by clinical trial designers. Assessment of PROs, such as sleep quality, can help to distinguish between agents that may have similar effects on disease activity, but differ significantly in their impact on daily symptoms and QoL parameters. The development of standard measures that incorporate assessments of sleep quality will promote more frequent and standardised reporting of this aspect of disease across clinical trials.
Taken together, the findings presented here demonstrate that abatacept treatment provides significant improvements in multiple aspects of sleep quality, as assessed by the MOS-Sleep measure, and suggest that the Sleep Disturbance Scale shows validity, reliability and sensitivity to change, making it a valid candidate for inclusion in a core set of measures of PROs.
Acknowledgments
The authors would like to thank Medicus International, for their editorial assistance.
References
Footnotes
-
Funding This study and the editorial support provided were funded by Bristol-Myers Squibb.
-
Competing interests GW has received research grants and honoraria from Bristol-Myers Squibb; consulting fees from Bristol-Myers Squibb, UCB, Eli Lilly; and speakers bureau fees from Bristol-Myers Squibb and Eli Lilly; TL owns stocks and is employed by Bristol-Myers Squibb; PT has received consulting fees from Bristol-Myers Squibb.
-
Ethics approval Ethics committee approval was obtained from various institutional review boards.
-
Provenance and peer review Not commissioned; externally peer reviewed.