Article Text

Abstract
Objectives: To suppress rheumatoid arthritis (RA) patients’ disease activity, it should be periodically measured and patients should be treated on the basis of the disease activity outcomes. Insight into the actual care, by using quality indicators, is the first step in achieving optimal care. The objective of this study was to develop a set of quality indicators to evaluate RA disease course monitoring of rheumatologists in daily clinical practice.
Methods: A RAND-modified Delphi method in a five-step procedure was applied: a literature search for quality indicators and recommendations about disease course monitoring; a first questionnaire round; a consensus meeting; a second questionnaire round and drawing up the final set.
Results: The systematic procedure resulted in the development of 18 quality indicators: 10 process, five structure and three outcome indicators that describe seven domains of disease course monitoring: schedule follow-up visits; measure disease activity; functional impairment; structural damage; change medication; preconditions for measuring disease activity and outcome measures in terms of disease activity.
Conclusions: This quality indicator set can be used to assess the quality of disease course monitoring of rheumatologists in daily clinical practice, and to determine for which aspects of disease course monitoring rheumatologists perform well, or where there is room for improvement. This information can be used to improve the quality of disease course monitoring.
Statistics from Altmetric.com
The goal of rheumatoid arthritis (RA) treatment is to suppress disease activity as soon as possible and as long as possible to prevent joint damage and loss of function.1 To achieve this goal it is important that patients’ disease activity is monitored and treatment decisions are based on the disease activity outcomes.2 ,3 ,4
Recommendations about optimal disease course monitoring can be derived from trials and international treatment guidelines.2 ,3 ,4 ,5 ,6 ,7 The aim of these recommendations is to support rheumatologists and patients in their medical decisions in order to supply RA patients with the best possible quality of care in daily clinical practice. However, the publication and dissemination of trial outcomes and guidelines does not automatically lead to a change or improvement in daily clinical practice.
The first step towards change and improvement is to gain insight into the actual quality of the given care.8 ,9 ,10 Precise measures, so-called quality indicators (QIs), are needed to measure the quality of care. QIs are often more specific compared with guideline recommendations: QIs describe exactly who should do what to whom and exactly when.11 ,12 ,13 ,14
So far, there have already been some initiatives in the development of QIs for rheumatic diseases. Maclean et al15 developed a QI set for rheumatic and musculoskeletal diseases and Khanna et al16 developed QIs specifically for RA. In addition, the American College of Rheumatology developed a set of QIs in which a number of the QIs of Khanna et al16 and Maclean et al15 are incorporated.17 However, in these three publications disease course monitoring was a minor topic, as the QIs focused on all aspects of care: from history to treatment (safety). Furthermore, these QIs are primarily about minimal standards of care and not about the optimal achievable quality of care. Therefore, the objective of this study was to develop a set of QIs specifically for disease course monitoring in RA to evaluate the quality in daily clinical practice in this area.11 ,18
Methods
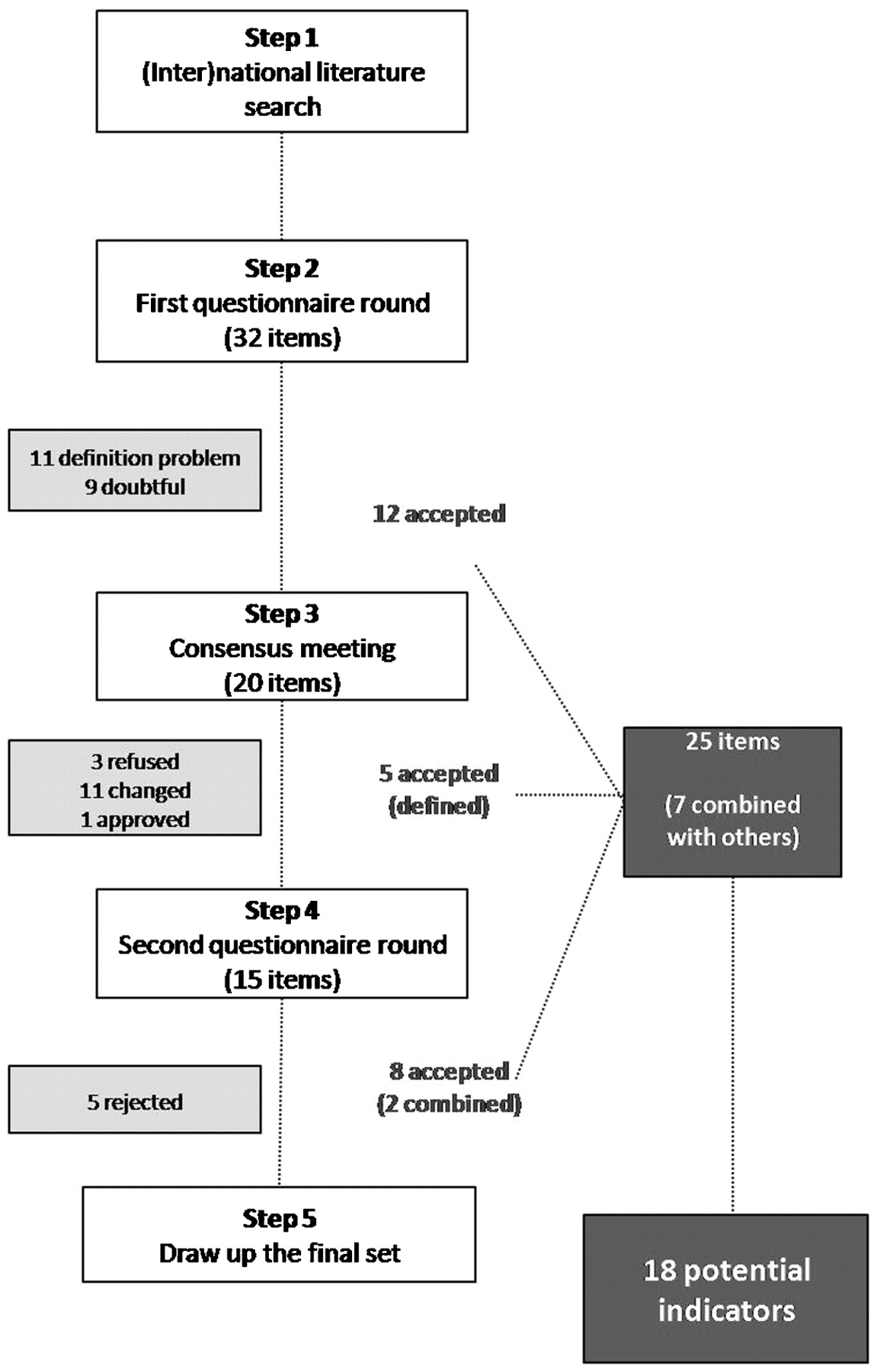
To develop a QI set for disease course monitoring, we applied a systematic approach: the RAND-modified Delphi method.19 The procedure is presented in fig 1 and consisted of five steps. For a complete description of the methods see appendix A (supplemental file available online only).

Scheme RAND-modified Delphi procedure.
Step 1
A systematic literature search in Pubmed was performed. Papers and (inter)national guidelines were searched for QIs and recommendations including the—at that time preliminary—RA guideline of the Dutch Institute for Healthcare Improvement (fig 2). See appendix B (supplemental file available online only) for all included studies and guidelines. Grade A1 recommendations and indicators were directly included.20 Other evidence grades recommendations and indicators were further processed in the first written questionnaire round.

Search strategy.
Step 2
Selected recommendations and indicators were translated into QIs by describing who should do what, to whom and when. An expert panel of Dutch rheumatologists (n = 13) were asked to rate QIs for the extent to which the description adequately reflected the quality of disease course monitoring on a 1–9 Likert scale (score 1, not at all to 9, excellent) and to define elements of the indicators (eg, “persistent disease”). In fig 3 an example is given. QIs were accepted or entered the following round based on the RAND/University of California at Los Angeles agreement criteria.19

{kind=link}
{kind=link}
{kind=link}
Example of a rating scale of a potential indicator.
Step 3
To achieve consensus about so far not accepted QIs and definitions of QI elements, all experts were invited to a consensus meeting. Rheumatologists received a personalised rating sheet on which the responses of all experts were visible; their own score was marked with an “X” (fig 3).
Step 4
Potential indicators that were discussed in the panel meeting were re-scored in a second questionnaire round. For those already accepted, participants were asked if they agreed with the new definition of QI elements.
Step 5
During a congress meeting organised by the Dutch Rheumatology Association (NVR), rheumatologists could comment on the pre-final set and final adjustments were made. The numerator and denominator descriptions were formulated for each QI: in the denominator the target group was described and in the numerator the actual performance in the target group.
Results
Thirty-two of the 56 papers contained recommendations or QIs for disease course monitoring (see table 1 for reasons for exclusion). In appendix C (supplemental file available online only) all 32 items of the original questionnaire are shown. Because none of the recommendations and indicators had a grade A1 evidence level, all items entered the first questionnaire round.
Reasons for exclusion of articles based on titles/abstracts or full text articles
Thirteen rheumatologists scored the items in the first questionnaire round. Seven rheumatologists (54%) attended the consensus meeting. In the second questionnaire round, 11 of the 13 questionnaires were returned (85% response).
Eighteen of the 32 initial indicators were accepted (56%) (table 2), either or not after reformulation: 10 process, five structure and three outcome indicators describing seven domains of disease course monitoring (table 3). The final QI set was included in the Dutch guideline for rheumatoid arthritis and was approved by the NVR.
Number of indicators in initial and in definite QI set
Final set of quality indicators (QIs) for monitoring of the disease course in RA
Process indicators (n = 10)
Process indicators describe the actual care given to patients. They were selected for five out of six domains (table 2). For “follow-up” it was concluded that RA patients should be seen once every 3 or 6 months on the basis of the patient’s disease activity (table 3).
For the QIs of “measure disease activity” and “measure functionality” the disease activity score in 28 joints (DAS28) and the health assessment questionnaire (HAQ), respectively, were chosen as the most appropriate indices.
For the domain “measure structural damage”, it was decided that x rays from hands and forefeet should be taken initially and 1 year after diagnosis. Thereafter the frequency depends on the patient’s disease activity and the presence of x rays from hands and forefeet in the previous year to serve as new reference x rays.
The decision to “change medication” should be based on the patient’s disease activity if the time to respond on the recent treatment is fulfilled and no extra-articular manifestations and comorbidities are hindering.
No indicators for “overall health” were accepted. It was agreed that measuring blood pressure and lipid levels was primarily a task of the general practitioner not of the rheumatologist. In addition, rheumatologists did not accept potential indicators on comorbidities and extra-articular manifestations because they could not define these indicators.
Structure indicators (n = 5)
Structure indicators describe organisational aspects of care. The structure QIs had to do with preconditions for measuring disease activity such as the availability of at least one specialised rheumatology nurse. Rheumatologists reported that they considered it important to monitor the disease course in RA, but they stated that it is only possible if there are adequate facilities, as described in the structure QIs, to achieve this.
Outcome indicators (n = 3)
The final goals of the delivered care are described by outcome QIs. They focused on patients’ disease activity in terms of the DAS28 (table 3). No outcome indicators were developed on functionality or structural damage. The experts gave two reasons for this: the effects of disease course monitoring and changing treatment accordingly should first result in a lower disease activity; functional impairment and progression of structural damage are partly seen as a consequence of the patient’s disease activity. Second, functional impairment or progression of structural damage are more influenced by other factors, such as prognostic features, age, disease duration and comorbidities.
Discussion
This is the first study specifically describing process, structure and outcome QIs for disease course monitoring. During their development it turned out that defining the elements within the indicators was the most difficult task for the experts. For example, what exactly was meant by “persistent” disease, “high” disease activity and “periodically”? These terms are commonly used within the field of rheumatology and are also used in recommendations. However, when experts were asked to describe what exactly is meant by them, this resulted in a broad range of definitions. This emphasises the importance of translating recommendations into understandable and measurable QIs to gain insight into the quality of care.
As described earlier, there have already been some initiatives in the development of QIs of RA.15 ,16 ,17 Our set of 18 QIs show some overlap with four QIs in the broader sets, the QIs for: (1) history and exam; (2) regular follow-up; (3) radiographs of hands and feet and (4) disease-modifying antirheumatic drugs. However, the few existing QIs for disease course monitoring were not always clear enough and measurable. For example, all initiatives included a QI describing that medication should be changed in case there is evidence of increased disease activity without describing what exactly was meant by increased disease activity.
This study has some limitations. None of the items had “grade A1” evidence and the structure and outcome QIs all had a “grade D” evidence. That is why all the items were scored by the 13 experts. The RAND methodology guidelines state that panels can be of any size, which permits sufficient diversity (minimum of seven), while ensuring that enough experts are able to participate in the consensus meeting (a maximum of 15). Our 13 participating rheumatologists were all experts: they were involved in the development of the Dutch guideline for RA or were a member of the quality committee of the NVR. Futhermore, many QIs had median scores of 8 and higher. Therefore, we are convinced that more rheumatologists or another expert panel would not have resulted in considerably different results and the same conclusions would have been drawn.21 ,22
The QIs were developed in a Dutch setting. We are convinced, however, that they also apply to other countries, especially because the results were based on internationally published studies and guidelines. However, for the structure indicators this could be different due to different health systems throughout the world. For example, the availability and financial support for a specialised nurse could be different between countries. In addition, we are aware that other (patient) derived measures for disease activity have been internationally developed and validated, such as the disease activity score (DAS), simplified disease activity index (SDAI), clinical disease activity index (CDAI) and rheumatoid arthritis disease activity index (RADAI).23 ,24 ,25 ,26 ,27 ,28 As the DAS28 is most often evaluated, our experts preferred the DAS28. Of course, (elements of) the other measurements can be seen as alternatives. Similarly, for functional impairment other indices and other versions than the HAQ could be used, such as the multidimensional-HAQ, McMaster Toronto Arthritis patient preference questionnaire (MACTAR) and the arthritis impact measurement scales (AIMS). Our expert panel, however, agreed that the HAQ was to be preferred.29 ,30 ,31 Again, the other instruments can be seen as alternatives.
In conclusion, this is the first study that developed process, structure and outcome QIs specifically for disease course monitoring in RA using a RAND-modified Delphi procedure. The applicability of this set should first be tested in practice. After that, this QI set can be used to determine the quality of disease course monitoring, for example by performing medical record examinations. In this manner, they can be used to determine for which aspects there is room for improvement. Furthermore, it is possible to perform determinant analyses to reveal factors that influence current practice. This information can be used to develop tailored interventions to improve the quality of disease course monitoring in practice.9
Acknowledgments
The authors would like to thank all the rheumatologists who participated in this study.
REFERENCES
Supplementary materials
Web Only Data 68/12/1805
Files in this Data Supplement:
Footnotes
▸ Additional supplemental appendices A, B and C are published online only at http://ard.bmj.com/content/vol68/issue12
Competing interests None.
Sponsorship: This study was sponsored by the Dutch Arthritis Association.
Provenance and Peer review Not commissioned; externally peer reviewed.