Article Text

Abstract
Objective: An observational case–control study was designed to analyse the discriminative value of ultrasound (US)-detected joint effusion compared with physical examination in the assessment of sacroiliac joints (SIJ) in patients with spondyloarthropathy (SpA) with or without inflammatory back pain (IBP).
Methods: 45 patients with SpA, classified according to European Spondylarthropathy Study Group criteria, and 30 healthy volunteers were studied. All patients had clinical evaluation of the SIJ, Bath ankylosing spondylitis (AS) metrology index, Bath AS disease activity index, Bath AS functional index, health assessment questionnaire, patient’s and physician’s visual analogue scale on global disease activity.
Results: Ultrasound showed joint effusion in 38.9% of SIJ of patients with SpA and in 1.7% of SIJ of controls (p<0.001). The presence of IBP was significantly associated with SIJ effusion assessed by US alone or plus at least one SIJ test. SIJ effusion assessed by US alone or plus at least one SIJ test had a positive likelihood ratio (LR) (2.67 and 4.04, respectively) for the presence of IBP higher than LR of single clinical tests. Positive sacral sulcus test, iliac gapping and midline sacral thrust test were associated with SIJ effusion assessed by US, but all clinical tests, singly and in various combinations, had a low LR for the presence of SIJ effusion assessed by US.
Conclusions: The study suggests that high resolution sonography is useful in the assessment of SIJ involvement in SpA, resulting in images that are fast and inexpensive and may locate, complementing the physical examination, the origin of IBP.
Statistics from Altmetric.com
The sacroiliac joints (SIJ) may be a hallmark of all spondyloarthropathy (SpA) subsets, such as ankylosing spondylitis (AS), psoriatic arthritis and undifferentiated SpA. The inflammation of these joints may be unilateral or bilateral, with different levels of severity. Inflammatory back pain (IBP) and sacroiliitis occur in all SpA subsets and rarely inflammation of the axial skeleton occurs in the absence of sacroiliitis.1
Many physical examination tests have been advocated as diagnostic aids in patients with SIJ pain, but examination findings are not consistently capable of identifying involvement of SIJ.2 Interpreting SIJ tests is difficult, because the variations in anatomy and motion in the SIJ are accompanied by movements of the lumbar spine and hip.3 Moreover, none of the available SIJ tests appears to be superior to others3 and the reliability of these tests has also been questioned.2
Musculoskeletal ultrasound plays an increasing and relevant role in the evaluation of SpA mainly for its ability to assess joint and periarticular soft tissue involvement and in particular for its capacity to detect enthesitis. Nevertheless, so far very few papers on US evaluation of the SIJ have been published, even though it has been demonstrated that signs of active synovitis could be detected with this diagnostic tool.4
We designed an observational case–control study to analyse the discriminative value of sonographic-detected joint effusion compared with physical examination in the assessment of SIJ in patients with SpA with or without IBP.
Patients and methods
We studied 45 consecutive patients with axial SpA (AS 19; psoriatic arthritis 6; undifferentiated SpA 20), classified according to European Spondylarthropathy Study Group criteria5 referred to the rheumatology clinic at Sapienza University of Rome. Thirty healthy volunteers (60 SIJ) without suspicion of inflammatory low back pain served as a control group.
Our study was conducted in compliance with good clinical practice, following the routine monitoring procedures performed in our unit for patients with SpA.
According to Calin et al6 IBP referred to the lumbosacral or buttock region was defined if four of the five following factors were present: (1) onset of back discomfort before the age of 40 years; (2) insidious onset; (3) persistence for at least 3 months; (4) associated with morning stiffness; (5) improvement with exercise. At the time of the evaluation, the presence or absence of IBP was assessed on the basis of the second question of the Bath ankylosing spondylitis disease activity index (BASDAI).
Patients were initially assessed by a single rheumatologist (GB) who took the clinical history and performed the physical examination, including clinical evaluation of the SIJ, Bath AS metrology index,7 BASDAI,8 Bath AS functional index,9 health assessment questionnaire10 and the patient’s and physician’s visual analogue scale on global disease activity (0–100 mm). Physical examination for the suspicion of SIJ abnormalities included:
Sacral sulcus tenderness (referred to tenderness immediately medial to the posterior superior iliac spine);11
Iliac gapping (with the patient positioned supine, the examiner crossed his arms, placed the heels of his hands on the anterosuperior iliac spines and pressed downward and laterally);12
Iliac compression (with the patient positioned lying on his side, the examiner exerted a downward force on the uppermost iliac crest);12
Midline sacral thrust test (the examiner applies a posteroanterior force to the sacrum as the patient lies prone);13
Gaenslen’s test (the patient lies supine as the contralateral hip is flexed and the ipsilateral hip is extended);11 13
Patrick’s test (stress of the SIJ by flexion, abduction and external rotation of the hip).11
The results of these tests are considered positive if the manoeuvres provoke pain at the right or left SIJ.
The erythrocyte sedimentation rate and C-reactive protein were measured and applied as biological signs of inflammation.
All patients and controls underwent evaluation of both SIJ.
Sonographic examinations were performed by a rheumatologist experienced in musculoskeletal sonography (AI), who was unaware of the subjects’ signs, symptoms and diagnosis. An Agilent HP Image Point Hx machine equipped with a linear probe (7.5 MHz) was used. Patients were examined in the prone position. The US examination started with the identification of the bony spinous processes in the midline and the posterior part of the SIJ, keeping the probe in a transverse position.14 The posterior contour of the sacrum was visualised as an echogenic line, whereas the sacral spinous process was shown as a concave curve at the midline, with sacral wings, represented by a regular echogenic line laterally. The SIJ was visualised as a hypoechoic cleft between two echogenic lines (sacrum and iliac bone).14 15 Joint effusion was detected when abnormal hypoechoic or anechoic intra-articular material that was displaceable and compressible but did not exhibit Doppler signal was present within the joint space.16 The finding was recorded according to an absent–present criterion.
Interreader reliability for sonographic recorded images, between two trained examiners (AI and FC), was established in 36 SIJ of 18 patients, randomly included independently of the presence or absence of IBP at the time of the evaluation. Intrareader reliability was established on recorded images in 36 SIJ with blinding to previous results and to the patient’s identity. The intrareader reliability was limited to the analysis of recorded images and was not performed on the entire process, which included image acquisition, because the single operator could remember, within a few days, the previous findings and would not have been blinded.
Statistical analysis
Categorical variables were analysed by the χ2 test or Fisher’s exact test when one of the expected cell frequencies was smaller than five. The results were presented as median (25th–75th percentile) and the significance of the differences was determined using the Mann–Whitney test for unpaired samples and Wilcoxon’s test for paired samples.
The sensitivity, specificity and likelihood ratio (LR) have been calculated with 95% CI. For the reliability analysis, the two-way mixed effect model (absolute agreement) and single measure intraclass correlation coefficients were used. Statistical significance was accepted at two-sided p<0.05.
Results
The main clinical and demographic features of 45 patients with SpA are shown in table 1. The mean age (42 years, range 20–68) and gender ratio (M/F 17/13) of controls were comparable with those of SpA patients. Clinical evaluation showed at least one positive test of SIJ in 82.2% of SpA patients and in none of the controls.
Main clinical and demographic features of 45 patients with SpA
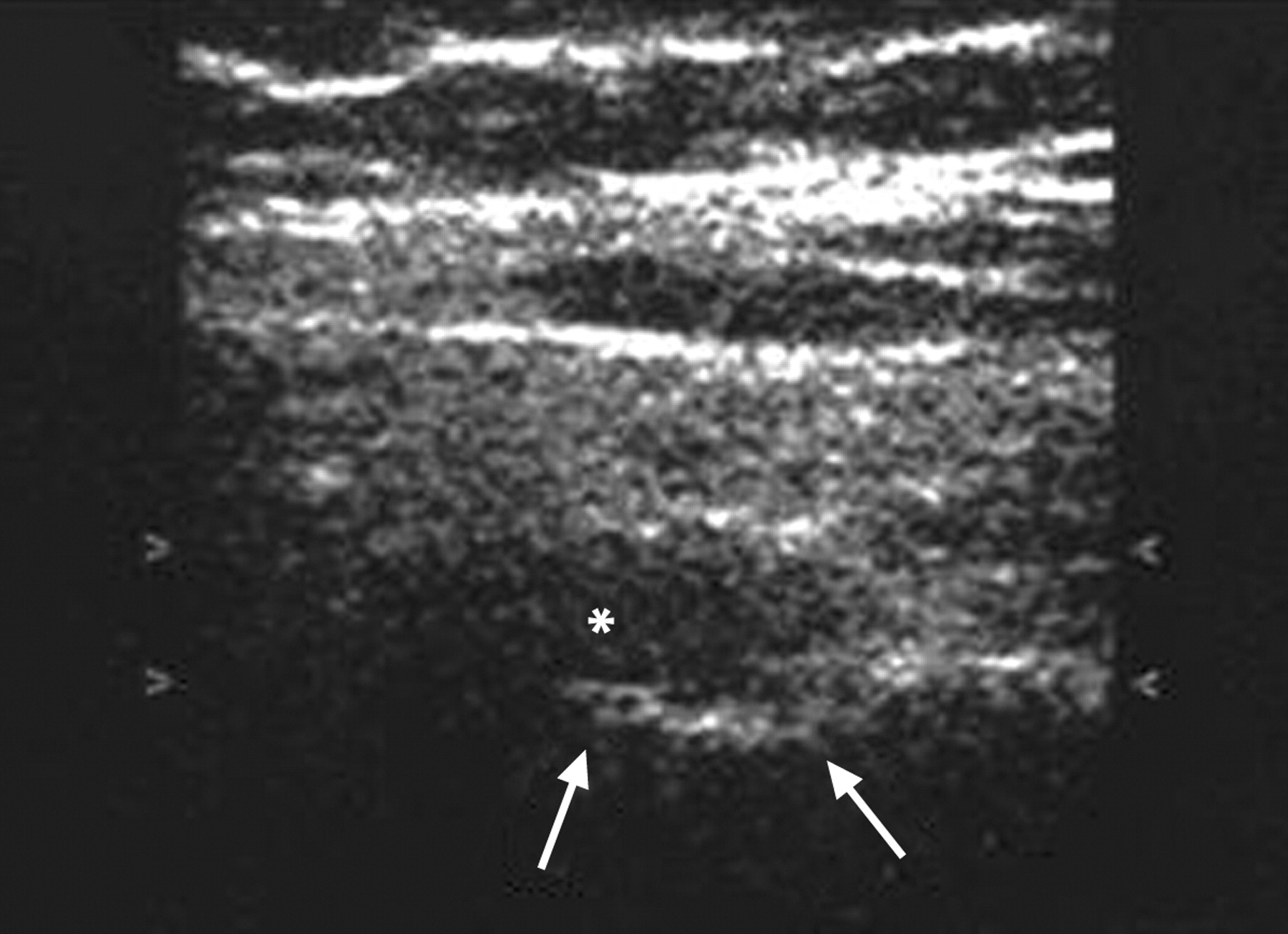
US showed joint effusion in 35 of 90 (38.9%) SIJ of patients with SpA (fig 1) and in one of the 60 (1.7%) SIJ of the controls (p<0.001). The interreader (0.827) and intrareader (0.945) reliability were very good. At the study entry, 28 (62.2%) of 45 patients with SpA had IBP referred to the lumbosacral region. The rate of US effusion and positive tests of SIJ in SpA patients with (n = 28) or without (n = 17) IBP referred to the lumbosacral region is shown in table 2. The sensitivity, specificity and LR of SIJ effusion and clinical tests for the presence of IBP are shown in table 3. The rate of positive SIJ tests in SpA patients with (n = 35) or without (n = 55) US effusion of SIJ was shown in table 4. The sensitivity, specificity and LR of SIJ clinical tests for SIJ effusion assessed by US are shown in table 5.
{kind=link}
Sonography of the right sacroiliac joint in a patient with spondyloarthropathy, using an Agilent HP Image Point Hx machine equipped with a linear probe (7.5 MHz). Posterior transverse scan. Joint effusion (*) within the sacroiliac joint is demonstrated. Arrows: bone profile of the sacroiliac joint.
Rate of US effusion and positive tests of SIJ in SpA patients with (n = 28) or without (n = 17) IBP referred to the lumbosacral region
Sensitivity, specificity and LR of SIJ effusion and clinical tests for the presence of IBP
Rate of positive SIJ tests in SIJ with (n = 35) or without (n = 55) US effusion
Sensitivity, specificity and LR of SIJ clinical tests for SIJ effusion assessed by US
Discussion
IBP is the key symptom of axial involvement in SpA and is present in the great majority of patients with AS and in approximately 70% of all patients with SpA.5 17 18 Moreover, patients with IBP related to SpA are most likely to move on to AS and may develop a chronic disabling disease. This symptom was considered in the European Spondylarthropathy Study Group5 and SA19 classification criteria. IBP is initially felt primarily deep in the gluteal region, is localised in SIJ but is occasionally referred towards the iliac crest, greater trochanteric or down to the dorsal thigh.19
Many physical examination tests have been advocated as useful tools in identifying patients with SIJ pain.20 21 There are two types of clinical tests in the assessment of SIJ involvement: motion palpation tests to assess movement; pain provocation tests to stress SIJ structures with the aim of reproducing the patient’s symptoms. Motion palpation tests rely on the detection of SJI movements, which are very limited. Moreover, these tests require palpation of landmarks that can vary in anatomy and are influenced by soft tissue tension. Another limit is the lack of specificity for pain provocation tests that not only stress the SIJ but also stress the lumbar spine, the hips and soft tissues over the SIJ.21 SIJ motion tests are thus questionable even if some support exists for the use of pain provocation tests.22 Among the more frequently used provocation tests we can consider sacral sulcus tenderness,11 iliac gapping,12 iliac compression,12 midline sacral thrust test,13 Gaenslen’s test11 13 and Patrick’s test.11 Nevertheless, clinical studies have for the most part demonstrated that physical examination findings are not consistently capable of identifying abnormalities of SIJ as pain generators.23 24 25 In addition, Dreyfuss et al26 found 20% of asymptomatic adults had positive findings on three commonly performed SIJ provocation tests.
Reproducibility has been found to be greater for provocative tests than for mobility and alignment assessments, but the validity and reliability of SIJ tests is debated.2 Whereas some studies found moderate to high interexaminer reliability, other studies did not confirm it.2
None of the available SIJ tests thus appears to be clearly superior to others.2 3 21 27 In clinical practice conclusions based on the results of several tests seem to be supported by the evidence that clusters of more pain provocation tests showed good reliability.27 These observations are confirmed by our results showing the lack of association of a single SJI test with the presence of IBP. In fact, a significant association was observed only when we considered a cluster of these tests.
Nevertheless, it is interesting to note that in our study the presence of IBP was significantly associated with SIJ effusion assessed by US alone or plus at least one SIJ test. The diagnostic value of a test can be expressed as the LR, which combines into one value the sensitivity and specificity of it. Our results showed that SIJ effusion assessed by US alone or plus at least one SIJ test had a positive LR (2.67 and 4.04, respectively) for the presence of IBP higher than the LR of single clinical tests used for the suspicion of SIJ abnormalities. However, the LR of IBP for axial SpA is only 3.1, indicating the limited value of this parameter when considered alone in the diagnosis of SpA.28
The clinical value of SIJ effusion assessed by US, according to the OMERACT definition,16 is also sustained by the evidence of a positive LR of 18 for SpA when we considered healthy controls. However, a limitation of this study is the lack of comparison with patients having back pain from other origins. These findings confirmed the previous few results on the usefulness of US in the evaluation of SIJ.17 18 19 24 US guidance can also be useful for local therapeutic injections of SIJ, allowing to have a 76.7% of success in positioning the needle in the SIJ15. Contrast-enhanced colour Doppler US seems to be a very sensitive technique in the detection of active sacroiilitis.29 Increased perfusion around or inside the SIJ is detected by colour Doppler US in 48% of patients with sacroiliitis, but also in some patients with osteoarthritis and in controls.14
More recently, colour and duplex Doppler US of SIJ, thoracolumbar and paraspinal areas showed that vascularisation was increased in patients with active disease therapy,? compared with controls and significantly lowered after anti-TNF-alpha, suggesting that colour and duplex Doppler US might be an alternative to magnetic resonance imaging in order to evaluate response to therapy.30 Nevertheless, it is well known that Doppler techniques may have low sensitivity in the detection of flow in deep areas such as SIJ and that their sensitivity is strictly influenced by the quality of the US equipment. Therefore, in our study we evaluated the presence/absence of effusion without using Doppler in order to assess the relationship between effusion and pain provocation tests and to suggest to clinicians a fast and useful bedside tool without the need for high-quality US machines, which are not commonly available in most rheumatology units and that often need expert operators. Positive sacral sulcus tenderness and midline sacral thrust test were associated with SIJ effusion assessed by US, with the highest sensitivity (71%) for sacral sulcus tenderness and the highest specificity (85%) for iliac gapping. Nevertheless, all clinical tests, singly and in various combinations, for SIJ had a low LR for the presence of SIJ effusion assessed by US.
In conclusion, our study suggests that high resolution sonography is useful in the assessment of SIJ involvement in SpA, resulting in images that are fast and inexpensive and may locate, complementing the physical examination, the origin of IBP. A limit of our study is the lack of comparison of US with magnetic resonance imaging. On the other hand, we would also like to point out that ultrasonographic detection of SIJ effusion is easy to perform, representing a quick but valuable bedside procedure that could be used directly by the clinician while assessing the patient with IBP and SpA. It requires standard and not sophisticated US equipment, available in most rheumatology units, thus suggesting that this diagnostic method could represent a relevant tool in clinical practice. Nevertheless, the value of US in patients with SpA should be confirmed by future research focused on clearly distinguishing inflammatory and degenerative SIJ diseases.
REFERENCES
Footnotes
Competing interests None.
Patient consent Obtained.