Article Text

Abstract
Objective: To apply and compare different classification criteria on a representative nationwide sample of psoriatic arthritis (PsA) twins and to estimate the prevalence and incidence of PsA.
Methods: The study comprised three Danish nationwide twin cohorts. In 1994 37 388 Danish twin individuals and in 2002 46 418 twin individuals received a questionnaire, including questions on rheumatic diseases. Twins reporting PsA and their co-twins were classified according to the Moll and Wright and CASPAR (ClASsification criteria for Psoriatic ARthritis) criteria based on interview, clinical examination and scrutiny of medical records.
Results: 228 twin individuals reported PsA and 164 (72%) participated in clinical validation. By using the Moll and Wright and CASPAR criteria, 54 and 50 cases were diagnosed with PsA respectively. The positive predictive value of self-reported PsA was 31%. According to the Moll and Wright and CASPAR criteria the prevalence was 0.15% (95% CI: 0.13%, 0.22%) and 0.14% (95% CI: 0.11%, 0.19%) respectively. The annual incidence rate based on new self-reported cases in 2002 was 6/100 000 person-years (95% CI: 3/100 000 person-years, 11/100 000 person-years).
Conclusions: The positive predictive value of self-reported PsA was 31%. The prevalence and incidence figures of PsA were equivalent to the previously reported occurrence in population- and hospital-based studies.
Statistics from Altmetric.com
Psoriatic arthritis (PsA) is a systemic inflammatory joint disease occurring in 5–42% of patients with psoriatic skin disease.1 In 1964 the American College of Rheumatology (ACR), formerly the American Rheumatism Association (ARA), accepted PsA as a unique disorder. Research on PsA has, however, been hampered by the lack of a validated or accepted case definition. Since the first case definition by Moll and Wright (M&W) in 1973,2 quite a few different criteria have been proposed.3 Recently, Helliwell and colleagues validated and compared existing criteria for PsA and showed that those by Vasey and Espinoza (V&E) had the best combined sensitivity and specificity.4 5 Subsequently, the same group developed a new set of PsA classification criteria—CASPAR (ClASsification criteria for Psoriatic ARthritis.5 6 However, the sensitivity and specificity of these new criteria are almost equivalent to those by V&E, when applied to PsA cases attending hospital clinics.6 Except for the CASPAR, the McGonagle and the criteria by Fournie, available criteria sets require the co-occurrence of psoriasis and arthritis. The CASPAR, McGonagle and Fournie criteria accept a family history of psoriatic skin disease.
Previously, there have been several attempts to identify subsets of PsA. The first attempt by Moll and Wright, which divided PsA into five subsets, has gained widespread acceptance.2 Subsequently, several modifications of this subclassification have appeared,7–12 which makes it difficult to compare across studies. However, at disease onset, the majority of cases present with asymmetric oligoarthritis, whereas symmetric polyarthritis or just polyarthritis is the most prevalent PsA phenotype in most studies on patients with long-standing disease.7 8 10 12–22 The proportion of patients with predominantly axial disease varies from a few per cent to 25%.
Previous representative studies including clinical evaluation of PsA cases or scrutiny of hospital records report prevalence rates of PsA at 0.10–0.20%.18 23–26 One recent study based on a telephone survey without clinical evaluation or review of medical files report a slightly higher prevalence at 0.25%.27 Annual incidence figures on PsA among Caucasians range between 3 and 8 per 100 000 person-years.18 28–31
The present study aims at estimating the prevalence, incidence and predictive value of self-reported PsA by applying the M&W and the CASPAR criteria on subjects with self-reported disease recruited from a nationwide cohort of unselected Danish twins (the National Danish Twin Registry).
METHODS
Ascertainment and characterisation of twins with psoriatic arthritis
This cross-sectional study was based on the Danish Twin Registry (DTR). In 1994, 38 790 twin individuals born 1921–1940 and 1953–1982 were invited to participate in a nationwide twin survey. A follow-up survey was conducted in 2002, which included 46 418 twin individuals among the 1931–1952 and 1953–1982 twin cohorts.32 The twins were asked identical questions about rheumatic diseases in the two surveys, including if the person had ever been diagnosed with PsA. The questions on PsA were validated in a rheumatology outpatient clinic and resulted in a sensitivity and specificity of 94% and 92% respectively (data not shown).
Twins reporting PsA received a clinical profile questionnaire followed by a telephone interview, and underwent a clinical examination if PsA was still suspected. For each twin with self-reported PsA we recorded demographic details and a standardised medical history was obtained. Clinical examination included a systematic evaluation of 76 joints (temporomandibular, sternoclavicular, acromioclavicular, shoulder, elbow, wrist, metacarpophalangeal, proximal interphalangeal, distal interphalangeal joints of the fingers, hips, knees, ankles, tarsal, metatarsophalangeal, proximal interphalangeal and distal interphalangeal joints of the toes), modified Schober’s test, lateral lumbar flexion, chest expansion and cervical movement. Enthesitis was recorded if present at patella, fascia plantaris, or the Achilles tendon. The pattern of psoriatic skin and nail involvement was recorded and Psoriasis Area and Severity Index score determined. Blood samples were drawn for the measurement of IgM rheumatoid factor, C-reactive protein, erythrocyte sedimentation rate, HLA-B typing on DNA. We collected available medical records to gain additional information about arthritis and psoriatic skin disease in the past. If relevant, additional x-rays were obtained. Before the study was initiated we addressed Dr Helliwell, Leeds, to be certain that we would apply all measures used in the CASPAR validation study. PsA was classified using the M&W as well as the CASPAR criteria.2 6 Psoriatic skin disease was both accepted if observed by the investigator and/or if documented in medical records by a dermatologist or a rheumatologist. In addition, arthritis was accepted if observed by the investigator or documented in medical records by a rheumatologist. Axial disease was defined as inflammatory back pain and definite sacroiliitis on x-ray. Polyarthritis and oligoarthritis was defined as ⩾5 and ⩽4 affected joints or joint areas (grouping affected metacarpophalangeal, proximal interphalangeal and distal interphalangeal joints as separate joint areas) respectively. As the distinction between oligoarthritis and polyarthritis differs somewhat in the literature, data on these subsets are also presented with cut-off values for oligoarthritis and polyarthritis at 3 and 4 respectively.
Validation of completeness
To identify non-responding twins with PsA or responding twins who failed to report PsA we made a record linkage with the Danish National Patient Registry (NPR). The NPR was established in 1969 and contains records of discharge diagnoses from admission to Danish hospitals and from 1994 records of diagnoses made in outpatient clinics were included. To estimate the extent of ascertainment completeness we used the capture–recapture method for two independent sources.33 34
Ethics
All regional scientific ethics committees in Denmark (20000085), and the Danish data protection board approved the study.
Statistical analysis
Data were analysed using univariate methods. For dichotomous variables, the differences between groups are expressed as a proportion, with 95% confidence intervals (95% CI). For continuous variables, the results are expressed as median values and range. Differences were assessed using the Mann–Whitney U-test with two-tailed p-values with a significance level at ⩽0.05.
RESULTS
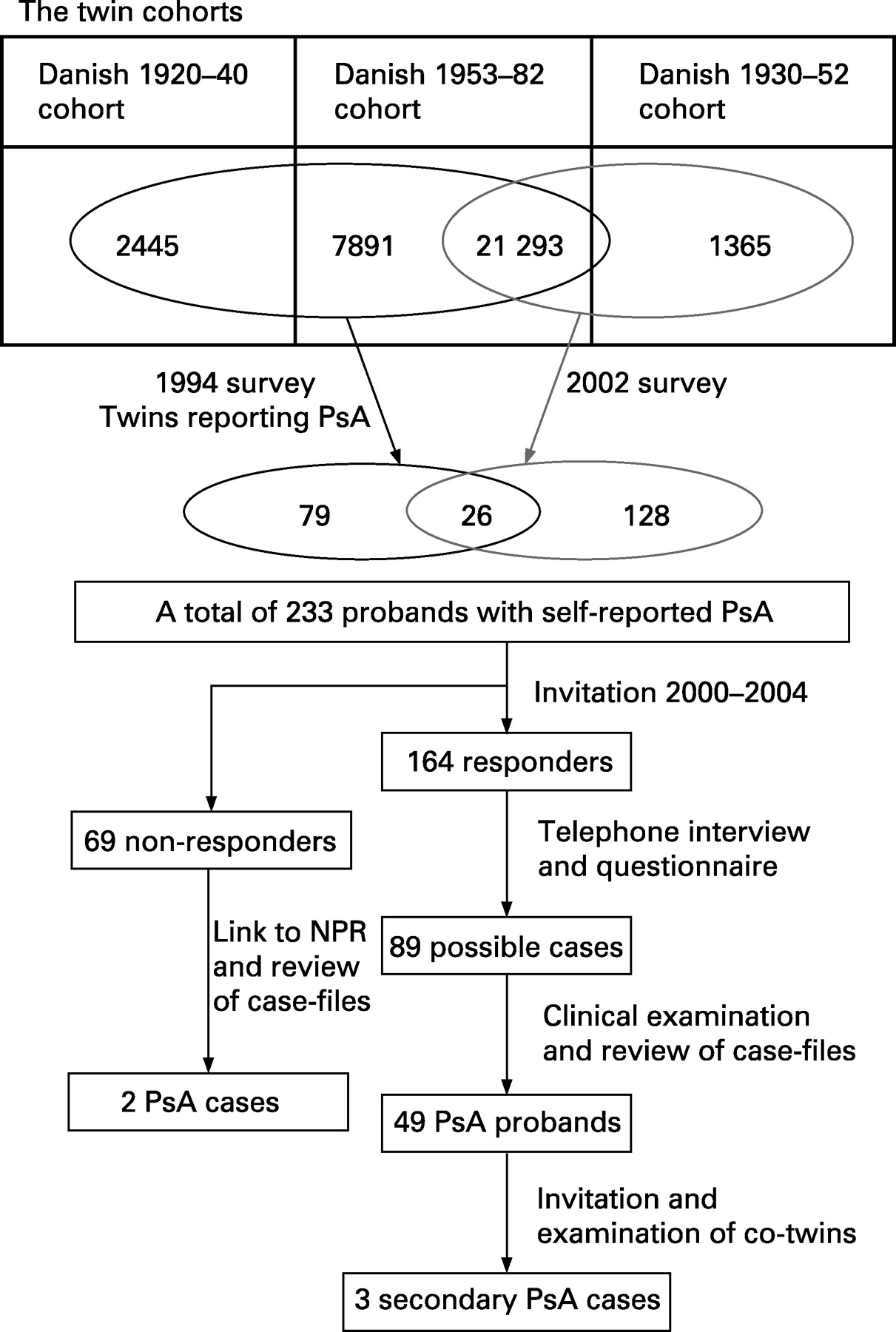
The response rates after one reminder were 81.5% (31 629 of 38 790) and 75.3% (34 944 of 46 418) in the 1994 and 2002 Danish Twin Surveys respectively. PsA was reported by 105 twin individuals in the 1994 survey and 155 twin individuals in the 2002 twin survey. A total of 233 (54 monozygotic (MZ) and 179 dizygotic (DZ)) twin individuals reported PsA in either 1994 or in 2002 or in both surveys. Subsequent invitation aiming at validation of the diagnosis resulted in 164 (38 MZ and 126 DZ) responders (fig 1). Among these, 32 reported either that they did not have PsA or declined from further participation in the study. Record linkage to the NPR and scrutiny of medical records revealed that two of these had PsA. The PsA diagnosis could be rejected in 43 twins prior to clinical examination based on clinical profile questionnaire, telephone interviews and in 10 cases based on their medical records. The remaining 89 twin responders underwent clinical examination and interview to ensure an optimally validated diagnosis. A total of 192 case files comprising 87 of the 89 responders were reviewed. 63 co-twins accepted to participate in the study (fig 1). x-Ray descriptions of peripheral and/or axial joints were collected in 65 participating probands and in seven co-twins.
{kind=link}
Non-responders
Among the non-responders to the secondary invitation 37 reported PsA in 1994, 27 reported PsA in 2002 and one reported PsA in both surveys. Non-responders were younger than responders (mean age responders 51, mean age non-responders 47, difference 4 (95% CI: −0.2, 8.4, p = 0.07)), sex distribution was equal between responders and non-responders (female proportion responders 0.49, non-responders 0.53, difference 0.04 (95% CI: −0.11, 0.18)), and there was almost equal zygosity distribution between the two groups (MZ proportion responders 38/164 = 0.23, MZ proportion non-responders 19/64 = 0.30, difference 0.07 (95% CI: −0.06, 0.20)).
Comparison between classification criteria
The CASPAR criteria apply different scores to current and previous psoriatic skin and nail disease.6 In the present study, psoriatic skin disease was documented in 72 cases by reviewing case files, but only 43 (60%) had psoriatic skin disease at current clinical examination. If only current psoriasis was accepted for a definite diagnosis of psoriasis, 50 PsA cases (probands and secondary cases) were retrieved using the CASPAR criteria. The definition by M&W does not discriminate between current and previous psoriasis, and consequently 54 cases would be classified with PsA by this definition.
Comparing the cases fulfilling the CASPAR and M&W criteria revealed that eight twins fulfilled the M&W criteria but not the CASPAR and four fulfilled the CASPAR but not the M&W criteria (table 1). The twins fulfilling the M&W criteria only all had previously documented psoriatic skin disease and oligoarthritis, four had previously diagnosed psoriatic nail involvement, and two had enthesitis. Among the twins fulfilling the CASPAR but not the M&W criteria all four reported psoriatic skin disease, which could not be confirmed, all were negative for IgM rheumatoid factor, two had psoriatic nail disease at the time of investigation, and three had dactylitis and enthesitis.
Completeness of the present study
The record linkage to the NPR identified 48 twins with a diagnosis of PsA, who had responded to the 2002 Danish Twin Survey. By scrutinising medical records, PsA was verified (according to M&W criteria) in 22 cases only. Medical records were unavailable in five cases. Based on these 27 cases and the 46 probands who responded to the 2002 survey, it was estimated that we may have missed a maximum of 13 cases (table 2). The completeness of the 2002 Danish Twin Survey was 70%.
Psoriatic arthritis occurrence
The prevalence of PsA among adults (age 20–72), based on PsA probands from the 2002 survey, was 51/34 944 (0.15% (95% CI: 0.11%, 0.19%)) and 46/34 944 (0.13% (95% CI: 0.10%, 0.17%)) according to the M&W and the CASPAR criteria respectively. If all twins responding to the 2002 twin survey, including secondary cases, were included the PsA prevalence was 54/34 944 (0.15% (95% CI: 0.12%, 0.21%)) and 50/34 944 (0.14% (95% CI: 0.11%, 0.19%)) based on the M&W and CASPAR criteria respectively.
Between the first and second survey nine and 10 new PsA cases were identified according to the M&W and CASPAR criteria respectively among the 21 293 twins born 1953–82 who responded to both surveys. This approach yielded an annual incidence rate of PsA at 6/100 000 person-years (95% CI: 3/100 000, 11/100 000) for twins aged 20–49. The peak incidence in this cohort was 10/100 000 person-years (95% CI: 5/100 000, 22/100 000) among twins aged 35–44 (both included). The positive predictive value of self-reported PsA was 31% (95% CI: 25%, 39%) according to the M&W criteria.
Characteristics of psoriatic arthritis cases
There were no differences between cases classified according to the different criteria with respect to age, sex, age at onset of arthritis or psoriatic skin disease, arthritis pattern, HLA-B27 or HLA-B13 prevalence (table 3). The median duration of arthritis was 9 years (range 1–49 years). The difference in proportion with respect to nail involvement between the CASPAR criteria (32%) and the M&W criteria (56%) is attributable to the fact that CASPAR criteria accept nail disease at current examination only. HLA-B27 and B13 antigen was present in 10% of the PsA cases. The prevalence of HLA-B27 and B13 antigens among Danish people has previously been reported at 9.1% and 4.2% respectively.35 None of the PsA probands had HLA-B17, HLA-B37, HLA-B39 or HLA-B62, and only one twin had HLA-B38, although all these different HLA-B types have been associated with PsA in previous studies.36–40
DISCUSSION
This is the first population-based study on the occurrence of PsA using the newly developed CASPAR criteria, which were compared with the M&W definition. The point prevalence of PsA was 0.15% and incidence was 6/100 000 person-years. The positive predictive value of self-reported PsA was 31%. The study was conducted on a nationwide twin cohort. Most previous studies on the prevalence of PsA have reported the occurrence of arthritis in psoriasis skin disease, thereby implying a risk of selection bias. In this setting PsA has been reported to occur in 7–42%.14 21 38 39 41 42 Concerning the occurrence of PsA in populations, most studies have been limited by the lack of clinical validation27 or sampling procedures involving hospital cases only.18 23 24 26 28–31 However, the prevalence and incidence figures in these previous studies conform with our results derived from a comprehensive unselected sample of Danish twins.
Strengths and weaknesses
Several issues should be considered when interpreting these findings, the possibility of bias in particular. However, the risk of selection bias would appear to be minimal in the present study, which was based on recruitment from an unselected, comprehensive twin population. The extent of ascertainment completeness was assessed by record linkage to the NPR, validation of data, and subsequent capture–recapture analysis for two independent sources. By this method it was calculated that we may have missed a total of 13 PsA cases. However, it follows from the ascertainment procedure that we may have missed cases that were undiagnosed prior to the survey. Furthermore, the method used for assessing incidence was limited by the cross-sectional approach, which implies that we may also have missed some incident PsA cases that eventually emigrated or died between the first and the second survey.
Information bias may arise from the same investigator examining the whole cohort or be due to misclassification of PsA. To address the first point, the impact of this factor was minimised by systematic interview and examination of all possible PsA cases, in addition to the collection of medical files. Concerning the possibility of misclassification we collected all data necessary for diagnosing PsA according to previously proposed criteria.
Classification criteria
We adopted the M&W criteria and the newly proposed CASPAR criteria.5 6 Because there is no “gold standard” available for diagnosing PsA, it was only possible to compare the efficiency of the different criteria by qualitative characterisation of the twins escaping classification by use of the different criteria. Although the original CASPAR criteria were anticipated to be more sensitive than the M&W criteria due to the inclusion of family disposition for psoriasis, the M&W criteria turned out to be the most sensitive. The main reason for this finding was the different scores applied to current psoriasis and previously documented psoriasis in the CASPAR criteria and, consequently, eight cases escaped classification by these criteria. Many epidemiological settings involve examination of cases at one time point only, and psoriatic skin and joint disease has a remitting–relapsing course and may eventually enter a complete remission; therefore, it would seem plausible not only to accept a well documented diagnosis of arthritis by a rheumatologist but also to include a previous history of psoriatic skin disease reported by a dermatologist or a rheumatologist.
Subclassification
For comparison with previous studies we adopted Helliwell et al’s 199112 interpretation of the M&W 1973 classification system,2 43 mainly because most other classification systems that have been proposed can be converted into this system. The original M&W classification divided PsA according to symmetric joint involvement and not according to the number of joints involved. Consequently, it is not feasible to compare the present results with all previous studies describing the PsA phenotypes (table 4). The differences between previous and current studies may reflect the differences with respect to genetic background, classification criteria, disease duration and sampling procedures. Only two studies on representative population samples have appeared in the past.21 25 However, the study by van Romunde et al25 did not describe the pattern of joint involvement, and the study by Alenius et al21 did not specify their definition of oligoarthritis and polyarthritis. Considering, that all other studies are based on hospital-treated PsA cases, it is likely that there is a preponderance of severe forms of PsA in these reports.
In conclusion, based on the present unselected nationwide twin study on the occurrence of PsA we have computed disease prevalence and incidence figures that are similar to those reported in previous studies from hospital settings. Consequently, the most valid prevalence measure on PsA among Caucasians is between 0.1% and 0.2% and the incidence is about 6/100 000 person-years.
Acknowledgments
The programme of twin research at the Danish Twin Registry has been supported by funding from the Danish Research Council, the University of Southern Denmark, the Danish National Research Foundation, Helsefonden, the Danish Diabetic Association, the Danish Heart Foundation and the United States National Institute on Aging (P01-AG08761). The present study was supported by the Danish Rheumatism Association, Aage Bang’s Fund, and the Danish Psoriasis Research Foundation and we appreciate the voluntary participation by the twins.
REFERENCES
Footnotes
Competing interests: None.