Article Text

Abstract
Objectives: To determine the efficacy of subsequent disease modifying antirheumatic drug (DMARD) therapies after initial methotrexate (MTX) failure in patients with recent onset rheumatoid arthritis (RA), treated according to the DAS for 2 years.
Methods: In groups 1 and 2 of the BeSt study, 244 RA patients were initially treated with MTX 15–25 mg/week. Patients who discontinued MTX because of insufficient clinical response (disease activity score, DAS >2.4) or toxicity were classified as “MTX failures.” In group 1, these patients switched to sulfasalazine (SSA), then leflunomide and finally to MTX + infliximab (IFX). In group 2, “MTX failures” added SSA to MTX, then hydroxychloroquine (HCQ), then prednisone, and eventually switched to MTX + IFX. “MTX successes” were patients who achieved a DAS ⩽2.4 after 2 years while still on MTX monotherapy. Total Sharp/van der Heijde score (TSS) progression from 0–2 years was assessed in “MTX failures” versus “MTX successes.”
Results: After 2 years, 162/244 patients (66%) had discontinued MTX because of insufficient response or toxicity. Of these, 78% also failed on SSA (adding or switching), 87% subsequently failed on leflunomide (in group 1), and 64% on MTX + SSA + HCQ (in group 2). 34 of 48 patients (71%) in groups 1 and 2 were successfully treated with MTX + IFX. After 2 years, regardless of the “success” on subsequent DMARDs, “ MTX failures” had a median TSS progression of 3 units (mean 9) versus 1 unit (mean 3) in “MTX successes” (p = 0.007).
Conclusion: After failure on initial MTX, treatment with subsequent conventional DMARDs is unlikely to result in a DAS ⩽2.4 and allows progression of joint damage.
- rheumatoid arthritis
- methotrexate
- DMARDs
- joint damage
Statistics from Altmetric.com
Rheumatoid arthritis (RA) is a common disease that causes progressive joint destruction and functional disability.1 Disease modifying antirheumatic drugs (DMARDs) have been proved to suppress disease activity and retard radiological joint damage, leading to a better long term prognosis.2 3 Methotrexate (MTX) is considered the anchor DMARD in treating active RA,4–6 because it has proved to be effective in suppressing disease activity,7–9 retarding radiological joint damage10 and being generally well tolerated.11 12 Many rheumatologists prescribe MTX as the initial drug treatment for RA.13 14 Large observational studies have shown high retention rates for MTX, with discontinuation more frequently caused by toxicity than by inefficacy.11 15 In these studies, various definitions for inefficacy were applied.
Since persistent disease activity is directly related to joint damage progression16 and achieving a state of clinical remission has become a realistic goal in recent years, it is important to suppress disease activity thoroughly and to measure response to treatment at regular intervals using a validated scoring method. Recent studies suggest that RA patients show improved outcomes if treatment is adjusted to achieve low disease activity by monitoring of the disease activity score (DAS).17–20
In the BeSt study,18 the European League Against Rheumatism (EULAR) criteria for clinical response were applied to achieve low disease activity in all patients. Treatment adjustments were obligatory when a DAS ⩽2.4 was not achieved. The aim of the present post hoc analysis of the BeSt study was to assess the efficacy of traditional DMARDs in patients who failed on methotrexate monotherapy in group 1 (sequential monotherapy) or group 2 (step up to combination therapy).
PATIENTS AND METHODS
Patient population
The BeSt study is a multicentre, randomised controlled trial comparing the clinical and radiological efficacy of four different treatment strategies in patients with active and recent onset RA.18 In the present study, patients randomised into groups 1 and 2 who actually began initial monotherapy with methotrexate (group 1, n = 126 and group 2, n = 118) were analysed.
Study design and treatment
The EULAR response criteria based on the DAS21 22 were used to monitor treatment success and provided guidelines for dosage adjustments, aiming for a DAS ⩽2.4 in all patients, which is the first requirement for classifying the effect of therapy as “good response.” The DAS is a validated composite outcome measure consisting of the Ritchie articular index (RAI), the number of swollen joints (swollen joint count, SJC, out of 44), general wellbeing as indicated by the patient on a visual analogue scale (VAS) and the erythrocyte sedimentation rate (ESR). Research nurses who were blinded for study treatment performed DAS calculations every 3 months. All patients began therapy with MTX 7.5 mg/week, after 4 weeks instantly increased to 15 mg/week, in combination with folic acid (1 mg/day). In the case of a DAS >2.4 after 3 months, MTX was increased to 25 mg/week (or the highest tolerated dose). Patients with a persisting DAS >2.4 on MTX 25 mg/week proceeded to next treatment steps (1 month overlap when switching from one single DMARD to the next, fig 1).

If a DAS ⩽2.4 was achieved and maintained for ⩾6 months, medication was tapered to a single DMARD in maintenance dose: 10 mg/week for MTX (tapering by 2.5 mg/month), 2000 mg/day for SSA and 10 mg every other day for leflunomide. Patients in group 2 tapered medication to MTX 10 mg/week. Prednisone and infliximab (IFX) were always tapered to zero. If the DAS increased to >2.4 after tapering to maintenance dose, the last effective dose of the last tapered drug was resumed. If DAS remained >2.4, the patient proceeded to next treatment steps.
In case of adverse drug events (ADEs), the responsible drug was tapered to the lowest tolerated dose, or discontinued if not tolerated at all. In this case, group 1 patients proceeded to the next step in the treatment protocol and group 2 patients continued with the other drugs in the combination. Concomitant treatment with non-steroidal anti-inflammatory drugs (NSAIDs) and intra-articular injections with corticosteroids were permitted. Systemic corticosteroids were not permitted.
Efficacy and definition of success
Patients who achieved a DAS ⩽2.4 during 2 years of follow-up on any therapy and remained on that therapy were classified as “successes” on that therapy. Patients who did not achieve a DAS ⩽2.4 or experienced ADEs and moved on to the next treatment step in the protocol were classified as “failures.” For each DMARD, “failures” were classified into three groups by reason of failure: (1) insufficient clinical response (DAS >2.4); (2) toxicity (ADEs resulting in DMARD discontinuation); (3) other reasons.
ADEs were reported by the patient, physician or investigator as a result of non-specific questioning on patients’ wellbeing, or physical or laboratory examination. ADEs could result in dose decrease, temporary or permanent DMARD discontinuation. The decision whether or not to discontinue the responsible DMARD was left to the discretion of the treating rheumatologist. Two trial physicians verified adherence to the pharmacoprotocol by checking the patients’ medical records every 3 months. Per treatment step, the actual number of days patients were on the DMARD or combination of DMARDs was determined to plot Kaplan-Meier drug survival curves. Patients who were lost to follow-up or withdrew consent with a last DAS ⩽2.4 were censored.
Radiological joint damage on radiographs of the hands and feet at baseline and after 2 years of follow-up was assessed comparing “MTX successes” and “MTX failures.” Two trained assessors, blinded for patient and centre identity scored all radiographs independently in random order according to the modified Sharp/van der Heijde method.23 Progression was defined as a change in total Sharp score (TSS) > smallest detectable change (SDC, 4.6 units).24
Statistical analysis
Differences between groups were tested using the χ2 test or the Student t test or the Mann-Whitney U test depending on the tested variable. For radiographic data, the mean (SD) and median (interquartile range, IQR) were given; differences between groups were tested by the Mann-Whitney U test. Patients with radiographs available at baseline and 2 years of follow-up (“completers”, n = 213) were included in the radiographic analysis. For the first three treatment steps in groups 1 and 2, Kaplan-Meier survival analysis was performed to determine the proportion of “successes” versus “failures” over time; differences were tested by the log rank test. Candidate variables with a p value of ⩽0.1 were selected for multivariate logistic regression analysis to identify demographic and disease characteristics at baseline as predictors for treatment success on methotrexate and sulfasalazine. All statistical analyses were performed using SPSS software (version 12.0.1 for Windows). p Values less than 0.05 were considered significant.
RESULTS
Evaluation of success on MTX
Baseline characteristics did not differ significantly between groups 1 and 2 (table 1).
Fifty-one patients (21%) achieved a DAS ⩽2.4 on MTX 15 mg/week after 3 months; One-hundred and seven patients (44%) achieved a DAS ⩽2.4 on MTX 15–25 mg/week after 6 months. After 2 years, 79 of 244 patients (32%) were “MTX successes” with a DAS ⩽2.4 while still on MTX monotherapy (fig 2A). Of these, 40 first had required a dose increase to 25 mg/week. The mean MTX doses in patients on MTX monotherapy after 6, 12, 18 and 24 months’ follow-up were 21.4, 18.5, 11.3 and 11.2 mg/week, respectively (0.29, 0.25, 0.16 and 0.15 mg/kg/week). Twenty-seven patients initially achieved a DAS ⩽2.4 on MTX within 6 months but proceeded to sulfasalazine after median 11.7 months because of a DAS >2.4 on MTX 25 mg/week.

After 2 years, 162 of 244 patients (66%) had discontinued MTX for the following reasons: 138/161 (85%) had a DAS >2.4 at the highest tolerated dose, 11/161 (7%) because of ADEs and 13/161 (8%) for other reasons (six dropped out, six because of patient incompliance, and one patient because of concomitant illness; all patients had a DAS >2.4). Three patients (1%) who dropped out while having achieved a DAS ⩽2.4 on MTX were censored in the MTX survival curves. Regarding toxicity, 47/244 patients (19%) experienced mild to moderate ADEs (elevated liver function tests or gastrointestinal symptoms) and discontinued MTX temporarily or decreased the dosage. Significantly more “MTX failures” than “MTX successes” received intra-articular steroids at least once (34% vs 20%, p = 0.029, no differences between groups 1 and 2).
Baseline characteristics for “MTX successes” and “MTX failures” differed significantly in sex, HAQ, DAS, tender joint count and time from diagnosis to inclusion (table 2). Multivariate logistic regression analysis identified a higher DAS at baseline (p = 0.006) and female sex (p = 0.023) as significant independent predictors for “MTX failure.”
Radiographic joint damage
Radiographs of the hands and feet at baseline and at 2 year follow-up were available in 213 patients (111 from group 1, 102 from group 2). At baseline, the two groups showed similar numbers of erosions, degrees of joint space narrowing and TSS (table 1). After 2 years, the median (IQR) TSS progression was 2 (0–9) for group 1 (mean (SD): 9 (17)) and 2 (0.5–7) (mean (SD): 5 (8) for group 2 (p = 0.717). TSS>SDC was observed in 40% of patients in group 1 and 35% of patients in group 2 (p = 0.608).
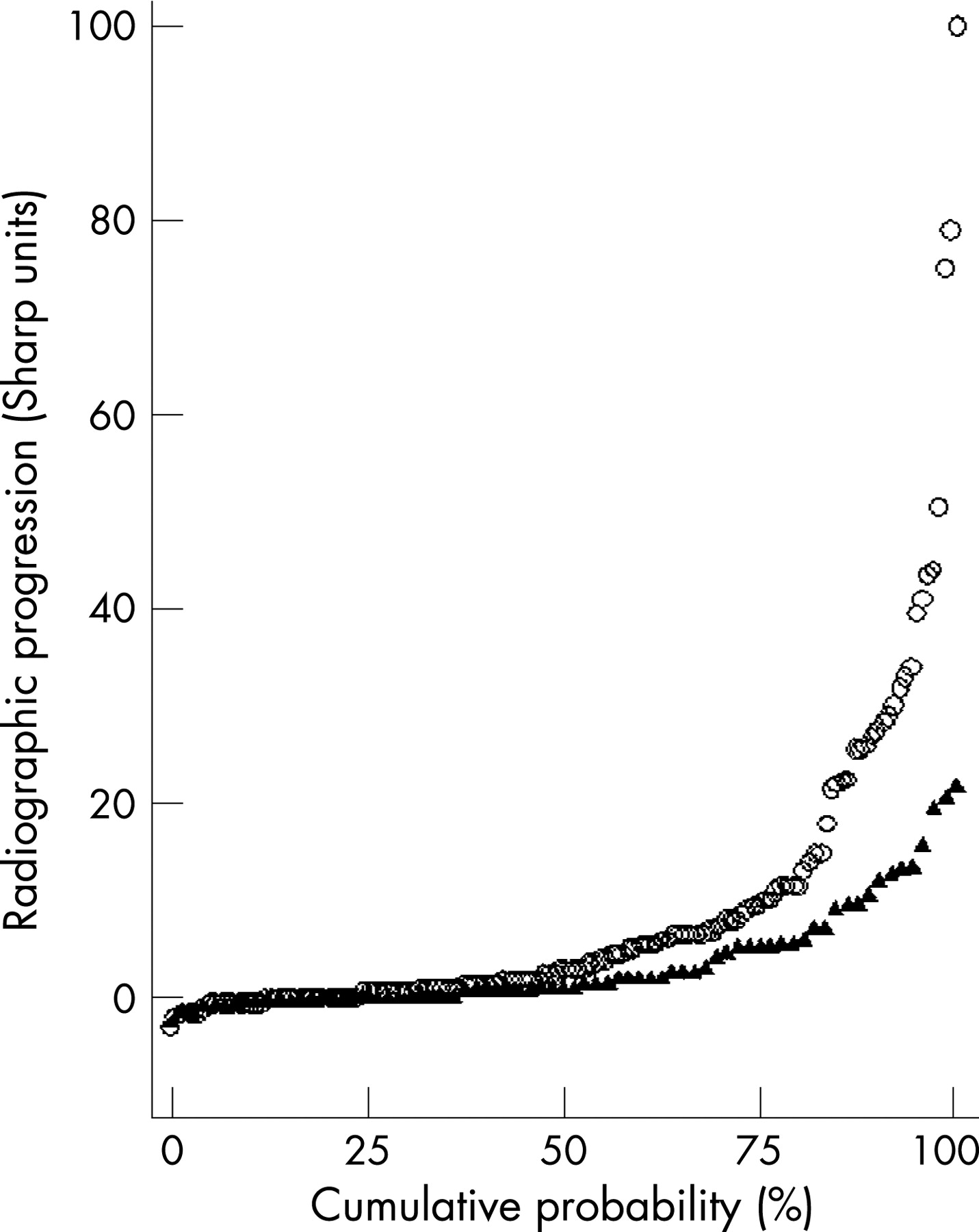
After 2 years, “MTX successes” showed significantly less TSS progression than “MTX failures,” regardless of the success on subsequent treatment steps (table 3 and fig 3). The median and mean TSS progression was 1 (0–5) and 3 (5) for “MTX successes” versus 3 (0.5–10) and 9 (17) for “MTX failures” (p = 0.007). There were no statistically significant differences in TSS progression between group 1 and group 2 in “MTX failures,” nor between patients who remained on MTX ⩽15 mg/week (n = 30) and patients who increased MTX to 25 mg/week (n = 49) in “MTX successes” (data not shown).

{kind=link}
{kind=link}
{kind=link}
Evaluation of success on SSA
During 2 years of follow-up, 138 “MTX failures” (69 from group 1, 69 from group 2) proceeded to sulfasalazine. Fifteen of 69 patients (22%) in group 1 achieved a DAS ⩽2.4 on SSA monotherapy (“successes”). Fifty-four patients (78%) discontinued SSA: 47 because of a DAS >2.4 and seven because of ADEs. Fifteen of the 69 patients (22%) in group 2 achieved a sustained DAS ⩽2.4 (“successes”) by adding of SSA to MTX (mean MTX dose 22.6 mg/week (0.31 mg/kg/week) at the start of SSA). Fifty-four patients (78%) failed on MTX+SSA: 41 because of a DAS >2.4 and 13 because of ADEs.
Overall, 24% of patients experienced ADEs on SSA. Five patients in group 1 versus eight in group 2 experienced mild to moderate ADEs and discontinued SSA temporarily or decreased the dosage; seven patients in group 1 versus 13 in group 2 permanently discontinued SSA (p = 0.11). The median achieved SSA dose in 119 patients receiving SSA for at least 3 months was 2000 mg/day (range 1000–3000), corresponding to 28 mg/kg/day.
In both groups 1 and 2, “SSA failures” had a significantly higher DAS, higher HAQ and more tender joints at the start of SSA treatment, and comprised more females than “SSA successes” (table 4). Multivariate logistic regression analysis identified female sex (p = 0.02) and a higher DAS at the start of SSA (p = 0.046) as significant independent predictors for “SSA failure”. Kaplan-Meier survival analysis illustrates that switching to (group 1) or adding of (group 2) SSA after MTX failure results in comparable discontinuation rates of SSA over time (p = 0.690, fig 2B).
Evaluation of success on step 3
During 2 years of follow-up, 98 “SSA failures” (54 from group 1, 44 from group 2) proceeded to the next treatment step. Seven of 54 patients (13%) in group 1 achieved a DAS ⩽2.4 on leflunomide (LEF) monotherapy. Forty-seven patients (87%) discontinued LEF: 41 because of a DAS >2.4 and six because of ADEs. Sixteen of 44 patients (36%) in group 2 achieved a sustained DAS ⩽2.4 by adding of hydroxychloroquine (HCQ) to MTX + SSA. Twenty-eight patients (64%) failed on MTX + SSA + HCQ: 21 because of a DAS >2.4; five because of ADEs; two for other reasons (the wish to become pregnant and patient non-compliance). In comparing the drug survival curves, significantly more patients achieved a DAS ⩽2.4 on MTX + SSA + HCQ than patients on LEF (p = 0.028, fig 2C).
Prednisone 7.5 mg/day was added to the treatment of 24 failures on MTX + SSA + HCQ. Twelve patients achieved a DAS ⩽2.4 on MTX + SSA + HCQ + prednisone; 12 other patients retained a DAS >2.4, 10 of whom proceeded to treatment with MTX+IFX.
After 2 years, 59% of all patients achieved a DAS ⩽2.4 with conventional therapy, 20% proceeded to MTX + IFX and subsequent treatment steps, 9% were treated outside the protocol and 12% had a missing DAS or dropped out.
Evaluation of success on MTX + IFX
During 2 years, 48 “failures” on ⩾3 DMARDs (38 from group 1, 10 from group 2) proceeded to MTX + IFX. Thirty-four of these 48 patients (71%, 28 from group 1 and six from group 2) achieved a DAS ⩽2.4 on IFX (nine needed a dose increase to maximum 10 mg/kg) and began tapering IFX to zero. Fourteen patients discontinued IFX: eight retained a DAS >2.4 despite dose increase to 10 mg/kg; six patients initially achieved a DAS ⩽2.4 on IFX 3–7.5 mg/kg but later failed on IFX 10 mg/kg (median 15 months after IFX initiation) for the following reasons: DAS >2.4 (two patients), ADEs (two), the wish to become pregnant (one) and protocol violations (one).
DISCUSSION
The data presented in this study show that 44% of patients achieved a DAS ⩽2.4 on methotrexate after 6 months, and that after 2 years, 32% of patients still exhibited sufficient clinical response on MTX monotherapy. After failure on MTX, consecutive treatment steps with other conventional DMARDs in monotherapy or an add-on setting seldom resulted in a DAS ⩽2.4. These results were obtained by applying strict response criteria derived from the EULAR criteria, defining patients as successes if they achieved and maintained a DAS ⩽2.4 on a specific treatment step.
This report also shows that patients who do not achieve and maintain a DAS ⩽2.4 with MTX, regardless of the success achieved with consecutive treatment steps, develop significantly more radiographic joint damage compared to patients with a DAS ⩽2.4 on initial MTX. To what account this damage progression may be caused by ineffective MTX therapy in the first 6 months is speculative. None the less, this observation confirms earlier studies suggesting that adequate, early suppression of disease activity is paramount for the suppression of joint damage progression.25–27 In addition, RA patients show improved outcomes if treatment is adjusted to achieve low disease activity by monitoring of the DAS,17 19 20 and fluctuations in disease activity are directly related to changes in radiographic progression.16 Therefore it seems appropriate to apply strict criteria for treatment response, in order to achieve better long term outcomes. As a result of our strict response criteria, we found more MTX discontinuation as a result of inefficacy than previous studies, who report mostly on discontinuation because of toxicity.11 15
One may speculate that adopting such strict criteria in the BeSt trial has led to premature discontinuation of MTX in patients with a high baseline DAS who then went on to do even worse on subsequent DMARDs, hence leading to radiological damage progression. However, the gradual decrease over time in average DAS in all treatment groups in the BeSt trial contradicts such a theory, and besides, in group 2 (step-up combination therapy), MTX was not discontinued but incorporated in combination therapies. The recent data from the SWEFOT study, also employing the EULAR criteria, are in concordance with our results, concluding that MTX monotherapy is adequate in only 30% of patients with early onset RA.28 Although not the primary objective, we identified male sex and a low DAS at baseline as independent predictors for MTX response, confirming previous data.28 29 Further research, including genetic polymorphisms,30 is needed to more precisely predict which patients will achieve a good response on MTX monotherapy.
After MTX monotherapy failure, the adding of sulfasalazine to methotrexate provided no additional benefit over switching to sulfasalazine monotherapy. The inhibition of reduced folate carrier by sulfasalazine could clarify this finding.31 Remarkably, a Scottish study reported a modest benefit of MTX + SSA combination therapy over MTX alone in SSA failures, claiming the in vitro effect found by Jansen not relevant in vivo.32 Our observations, however, provide additional evidence discouraging a choice for MTX + SSA combination therapy, as has been shown before in DMARD naive patients.33 34
A significantly higher, although still modest, percentage of patients achieved a DAS ⩽2.4 by adding HCQ to MTX + SSA after failing on MTX + SSA, compared to patients who switched to leflunomide monotherapy. This corresponds to results published by O’Dell, who reported a superior efficacy of the triple combination MTX + SSA + HCQ over MTX + SSA in DMARD naive patients as well as MTX suboptimum responders.35
Patients who failed at least three different conventional DMARDs including MTX were treated with the combination of MTX and infliximab. In this unfavourable subselection of RA patients, 71% responded well to MTX + IFX by achieving a sustained DAS ⩽2.4. These data are comparable with earlier trials showing that infliximab can induce a good clinical response in a majority of patients with active RA despite treatment with methotrexate.36 37 In addition, treatment with infliximab and other tumour necrosis factor antagonists has proved to slow or even stop progression of joint damage in these patients.37–39 Owing to small patient numbers proceeding to MTX + IFX within the 2 years of this study, we could not verify such a beneficial effect on joint damage progression in this population. Because the BeSt trial did not include the immediate introduction of triple or quadruple combination therapy in failures on MTX monotherapy, one can only speculate on the effect of such a regimen.
In conclusion, this subanalysis of the BeSt trial shows that 32% of patients with early onset RA achieve a good clinical response (DAS ⩽2.4) on initial methotrexate monotherapy. Success rates with subsequent conventional DMARDs are disappointing. Regardless of the clinical response on subsequent DMARDs, patients who fail methotrexate monotherapy develop significantly more radiographic joint damage than “MTX successes.” We suggest that in failures on initial methotrexate monotherapy, clinically and radiologically effective treatment with a tumour necrosis factor blocker such as infliximab should not be delayed, since switching to or adding other conventional DMARDs offers little chance of clinical efficacy and allows progression of joint damage.
Acknowledgments
We thank all patients as well as the following rheumatologists (other than the authors) who participated in the Foundation for Applied Rheumatology Research (all locations are in the Netherlands): WM de Beus, MD (Medical Center Haaglanden, The Hague); MHW de Bois, MD (Medical Center Haaglanden, The Hague); G Collée, MD (Medical Center Haaglanden, The Hague); JAPM Ewals, MD (Haga Hospital, The Hague); BAM Grillet, MD (De Honte Hospital, Terneuzen); KH Han, MD (Medical Center Rijnmond-Zuid, Rotterdam); HMJ Hulsmans, MD (Haga Hospital, The Hague); MH de Jager, MD (Albert Schweitzer Hospital, Dordrecht); JM de Jonge-Bok, MD (Groene Hart Hospital, Gouda); MV van Krugten, MD (Walcheren Hospital, Vlissingen); H van der Leeden, MD (retired); WF Lems, MD (Slotervaart Hospital, Amsterdam); MF van Lieshout-Zuidema, MD (Spaarne Hospital, Hoofddorp); A Linssen, MD (Kennemer Gasthuis, Haarlem); PAHM van der Lubbe, MD (Vlietland Hospital, Schiedam); C Mallée, MD (Kennemer Gasthuis, Haarlem); HK Markusse, MD (deceased); AJ Peeters, MD (Reinier de Graaf Groep, Delft); HK Ronday, MD (Haga Hospital, The Hague); D van Schaardenburg, MD (VU Medical Center, Amsterdam and Jan van Breemen Institute, Amsterdam); PEH Seys, MD (Lievensberg Hospital, Bergen op Zoom); RM van Soesbergen, MD (retired); PBJ de Sonnaville, MD (Oosterschelde Hospital, Goes); I Speyer, MD (Bronovo Hospital, The Hague); JPh Terwiel, MD (Spaarne Hospital, Hoofddorp); AE Voskuyl, MD (VU Medical Center, Amsterdam); ML Westedt, MD (Bronovo Hospital, The Hague); S ten Wolde, MD (Kennemer Gasthuis, Haarlem). We would also like to thank all other rheumatologists and trainee rheumatologists who enrolled patients in this study, and all research personnel for their contribution to this article.
REFERENCES
Footnotes
Competing interests: Professor Dr FC Breedveld did a paid expert testimony for Centocor in 1996 and was a paid speaker in a Schering Plough sponsored symposia. Dr CF Allaart was a paid speaker in a Schering Plough sponsored symposium in 2006.
Funding: The BeSt study was supported by a grant of the Dutch College for Health Insurance Companies (CVZ). Schering-Plough and Centocor provided additional funding. The funding sources were not involved in the design of the study, the collection, analysis and interpretation of data, the writing of the report or the decision to submit the paper for publication.
All authors: FARR Trial Group, Leiden, Netherlands
- Abbreviations:
- ADEs
- adverse drug events
- DAS
- disease activity score
- DMARDs
- disease modifying antirheumatic drugs
- ESR
- erythrocyte sedimentation rate
- EULAR
- European League Against Rheumatism
- HAQ
- health assessment questionnaire
- HCQ
- hydroxychloroquine
- IFX
- infliximab
- IQR
- interquartile range
- LEF
- leflunomide
- MTX
- methotrexate
- NSAIDs
- non-steroidal anti-inflammatory drugs
- RA
- rheumatoid arthritis
- RAI
- Ritchie articular index
- SDC
- smallest detectable change
- SJC
- swollen joint count
- SSA
- sulfasalazine
- TSS
- total Sharp/van der Heijde score
- VAS
- visual analogue scale