Article Text

Abstract
Objective: To describe the functional consequences of hand osteoarthritis, and analyse associations between personal factors, hand impairment, activity limitations, and participation restrictions within the framework of the International Classification of Functioning (ICF).
Methods: 87 women with hand osteoarthritis completed a clinical examination including recording of sociodemographic data, measures of hand impairment, and completion of self reported health status measures. The function subscale of the AUSCAN Osteoarthritis Hand Index was used as a measure of hand related activity limitations, while the Canadian Occupational Performance Measure (COPM) was used to describe and measure activity limitations and participation restrictions as perceived by the individual. The study variables were categorised using the dimensions in the ICF framework and analysed using bivariate and multivariate statistical approaches.
Results: The patients described problems in many domains of activity and participation. The most frequently described hand related problems were activities requiring considerable grip strength combined with twisting of the hands. On the impairment level, the patients had reduced grip force and joint mobility in the hands, and resisted motion was painful. Regression analyses showed that hand related activity limitations were associated with measures of hand impairment, while activity and participation (as measured by the COPM) were more strongly associated with personal factors than with hand impairment.
Conclusions: Hand osteoarthritis has important functional consequences in terms of pain, reduced hand mobility and grip force, activity limitations, and participation restrictions. Rehabilitation programmes should therefore be multidisciplinary and multidimensional, focusing on hand function, occupational performance, and coping strategies.
- ASES, Arthritis Self Efficacy Scale
- AUSCAN, Australian/Canadian Osteoarthritis Hand Index
- CMC, carpometacarpal joint
- COPM, Canadian Occupational Performance Measure
- DIP, distal interphalangeal joint
- ICD-10, International Classification of Diseases, 10th revision
- ICF, International Classification of Functioning, Disability and Health
- PIP, proximal interphalangeal joint
- VAS, visual analogue scale
- hand osteoarthritis
- International Classification of Functioning
- occupational therapy
Statistics from Altmetric.com
- ASES, Arthritis Self Efficacy Scale
- AUSCAN, Australian/Canadian Osteoarthritis Hand Index
- CMC, carpometacarpal joint
- COPM, Canadian Occupational Performance Measure
- DIP, distal interphalangeal joint
- ICD-10, International Classification of Diseases, 10th revision
- ICF, International Classification of Functioning, Disability and Health
- PIP, proximal interphalangeal joint
- VAS, visual analogue scale
Osteoarthritis is the most common joint disorder in the world, affecting as many as 12% of the American population between the ages of 25 and 75 years.1 The most commonly affected joints are hands and feet, hips, and knees. Hand osteoarthritis typically involves the distal interphalangeal joints (DIP), the proximal interphalangeal joints (PIP), and the first carpometacarpal (CMC) joints, and affect 75% of women aged 60 to 70 years.2,3 Many studies conclude that hip and knee osteoarthritis causes severe functional limitations.4–,6 However, the contribution of hand osteoarthritis to impairment and activity limitations is less clear.7 Although there seems to be an association between radiographic abnormalities and clinical findings such as bony swelling, pain, and decreased grip strength, the discordance between symptoms, signs, and functional impairment in hand osteoarthritis is well recognised.8,9,10,11 Thus more knowledge of the consequences of hand osteoarthritis is required to improve the outcomes of professional services and to ensure that rehabilitation services are focused on the patient’s expressed needs and problems.6,7
In order to describe and analyse the functional consequences of various health conditions, the World Health Organisation (WHO) has developed the framework International Classification of Functioning, Disability and Health (ICF).12 In ICF, health and health related components are classified in two dimensions: body functions and structures, and activity and participation, with impairment, activity limitations, and participation restrictions as the negative terms or consequences of problems in each ICF dimension. The model also describes contextual facilitators or barriers as either personal or environmental factors. Each component in the ICF is further classified, except the category “personal factors”. According to WHO, ICF may be combined with the International Classification of Diseases (ICD-10), thereby serving as models to sum up information and measures of disease and disability, and to analyse associations between different aspects of functioning.13
However, the ICF has been criticised for overlooking the subjective dimension of disability, not taking into account that the importance, satisfaction, and meaning connected to the ability to perform various activities or participate in life situations may vary among individuals.14 Furthermore, several studies have shown that personal factors such as the patient’s level of self efficacy are related to clinically important outcome measures, such as pain and health status.15–,17
Our aim in this study was to describe and measure both the objective and the subjective functional consequences of hand osteoarthritis with regard to impairment, activity limitations, and participation restrictions. A second objective was to analyse associations between personal factors and body functions in terms of hand function (grip force, pain, and mobility of the finger joints), and activity limitations and participation restrictions.
METHODS
Patients
The study was part of a larger study aimed at describing clinical and functional consequences of hand osteoarthritis, and was approved by the regional ethics committee.18 Participants were recruited among patients previously referred to a rheumatology outpatients department. Of those agreeing to participate in the larger study, the first 100 were consecutively included in the present study. Inclusion criteria were age between 50 and 70 years, ability to communicate well in Norwegian, and osteoarthritis of the hand according to the classification criteria of the American College of Rheumatology.19 Exclusion criteria in the present study were functional problems mainly related to diseases other than osteoarthritis, or cognitive deficits affecting the interview or scoring processes.
Sample and data collection
The study employed a cross sectional design. The data collection comprised a comprehensive clinical examination by a rheumatologist, including recording of sociodemographic data and disease related factors, and completion of several self reported health status questionnaires. Within three weeks after this examination, the patients completed an interview with an occupational therapist, addressing activity limitations and participation restrictions. Following the interview, hand function was evaluated according to previous recommendations concerning core outcomes for clinical trials in hand osteoarthritis, by measuring joint mobility, grip strength, pinch strength, and pain.20–,22
Assessments
The variables collected were categorised according to the dimensions of the ICF model,12 (fig 1⇓).

The International Classification of Functioning, Disability and Health (ICF) was used to organise potential explanatory variables in the study.
Personal factors
Age, disease duration, comorbidity, and self efficacy were grouped as personal variables.
Self efficacy is concerned with people’s judgements of their capabilities to execute given levels of performance and to exercise control over events,23 and was measured using the function subscale in the Arthritis Self Efficacy Scale (ASES).24 This subscale contains nine statements on function with which the patient may agree or disagree. The scores are expressed as values between 10 and 100, a score of 10 representing the lowest possible level of self efficacy.
Impairment variables
The impairment variables are measures of limitations or problems in body function or structure related to the disease.12 The most important clinical characteristics of hand osteoarthritis are pain and reduced joint mobility and grip force. The following measures were chosen to reflect these characteristics at the impairment level.
Joint mobility of both hands was measured as follows:
flexion deficit of digits II-V as the distance in mm from the distal palmar crease to the distal point of the digits;
extension deficits of digits II-V as the distance in mm from the distal point of the nailbed of the extended fingers to a table where the patients rested their hand in a supinated position;
opposition deficit of digit I as the distance between the tip of the thumb and the base of digit V;
radial abduction of the thumb as the angle between the metacarpal bones of the thumb and the digit II parallel to the plane of the palm.25,26
For both hands, grip strength and three pod pinch strength (thumb, index and long finger) were measured in Newtons (N) by the Grippit electronic instrument,27,28 with the subjects sitting in a standard position with the elbow in 90° flexion and the wrist in a neutral position. Force recordings are displayed on the Grippit electronic unit every 0.5 seconds while the 10 second grip is in progress. The mean of the 20 registrations was recorded.
Immediately following each assessment of grip force, pain was measured on a 100 mm visual analogue (VAS) scales ranging from 0 = no pain to 100 = maximal pain, by asking the patient to mark the amount of pain experienced during the resisted motion in respectively grip strength and pinch strength for each hand.
Activity and participation variables
Activity limitations are the difficulties an individual may have in executing a task or action, while participation restrictions are the problems an individual may experience in involvement in life situations.12 According to the ICF, one way of differentiating between activity and participation is to designate all detailed domains as activities and the broad category headings as participation.12
We therefore considered the physical disability scale of the Australian/Canadian Osteoarthritis Hand Index (AUSCAN) to be a measure of hand related activity limitations.3,18,29 In AUSCAN the patients rate their problems with performing the following nine activities on a scale of 0 (no problems at all) to 4 (extremely difficult): opening a new jar, carrying a full pot, picking up large heavy objects, fastening jewellery, turning taps/faucets on, doing up buttons, wringing out washcloths, peeling vegetables, and gripping and turning a round doorknob or handle. The mean score of the nine items constitutes the final AUSCAN function score.
The Canadian Occupational Performance Measure (COPM) was used to describe and measure the qualitative and quantitative aspects of activity limitations and participation restrictions as perceived by the individual.30 During a semistructured interview, the patients identify their problems within three areas of self care, productivity, and leisure, and rate the importance of each problem on a scale from 1 (not important at all) to 10 (extremely important) in order to make priorities. Finally, the patients rate the most important activities (up to five) for performance and satisfaction with performance on scales from 1 (not able to do it, not satisfied at all) to 10 (able to do extremely well, extremely satisfied). Total performance and satisfaction scores are calculated by dividing the sum of the scores by the number of problems. The psychometric properties of the COPM have been established in many groups of patients, among them those with rheumatoid arthritis,31 osteoarthritis,32 ankylosing spondylitis,33 fibromyalgia,34 and chronic pain.35
Data analysis and statistics
The qualitative data were analysed as follows: first the patients’ statements concerning activity problems and participation restrictions during the COPM interview were read through, then codes were identified to describe the data, after which the codes were combined into broader categories.36 Frequency counts on responses were undertaken where appropriate.
Proportion and frequency counts were also calculated for categorical variables, while mean and standard deviation were computed for continuous variables. Differences between the right and the left hand were examined by paired samples t tests. Correlations between the COPM scores, the AUSCAN score, and the impairment variables were examined by Pearson correlation coefficient.
Three hierarchical regression analyses were conducted. The AUSCAN score, an indicator of hand related activity limitations, served as the dependent variable in the first model, while the COPM performance score and the COPM satisfaction score served as the dependent variables in the two other models, as indicators of activity limitation and participation restrictions.
According to the ICF model, a blockwise analysis was used to calculate the explanatory power of the independent personal and impairment variables on the dependent variable. To do this, the following variables were entered into the model in two blocks (fig 1⇑):
Block 1 (personal factors): age, disease duration, comorbidity, and the self efficacy function score.
Block 2 (impairment variables) (all measures are for the right hand): grip force in pinch grip, pain during resisted motion (pinch grip), and mobility restrictions digits I-V (computed as the sum of the three mobility deficit measures).
Before conducting the regression analyses, possible colinearity of the independent variables was examined using the variance inflation factor. Further on, distribution of the residuals was examined for normality. As recommended when small samples are involved, we chose a conservative approach in presenting the results from the regression analyses, using the adjusted R2 values.37 We used SPSS for Windows (version 11.0) for the statistical analyses. Probability (p) values below 0.05 were considered significant.
RESULTS
Sample
Of 100 consecutively approached patients, 94 attended the baseline assessments. Two of these were excluded because of functional problems mainly related to cerebral palsy (n = 1),and cognitive deficit (n = 1). As sex is known to affect pain and function,7 and there were only five men among the included participants, it was decided to exclude these from the further analyses. The demographics of the 87 final female patients are presented in table 1⇓. Although the inclusion criterion was hand osteoarthritis, more than half of the patients also had osteoarthritis in other joints, with the knees being the most commonly affected joints.
Personal characteristics, activity limitations, and participation restrictions in 87 women with osteoarthritis.
Activity limitations and participation restrictions
The patients listed a total of 801 occupational performance problems in the COPM interviews, and prioritised 361 of these. As the COPM interviews were oriented towards revealing activity limitations and participation restrictions in general, the patients described the problems they experienced in their daily life regardless of whether these were caused by osteoarthritis of the hands or of other joints.
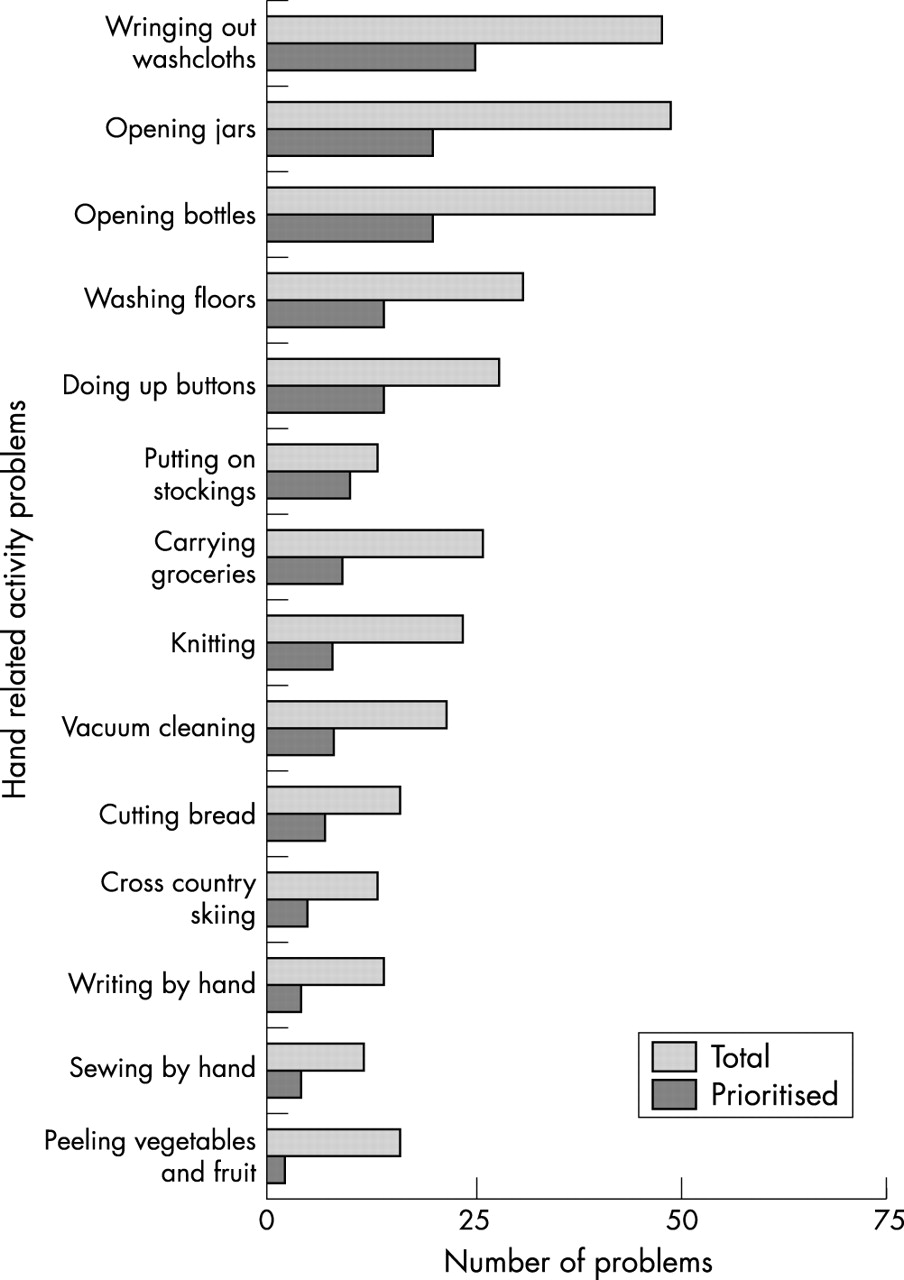
The most commonly described problems were related to the categories “household management” (337 reported problems), “functional mobility” (119 reported problems), “personal care” (102 reported problems), and “active recreation” (68 reported problems)(data not shown). The most frequent reported hand related activity problems were “wringing out wash cloths”, “opening jars”, and “opening bottles” (fig 2⇓). The mean AUSCAN score was 1.80, indicating that this group of patients has moderate problems with performance of hand related activities (table 1⇑).
{kind=link}
{kind=link}
The 14 most commonly described and prioritised hand related activity problems reported by 87 women in COPM interviews, given in rank order from the most often prioritised to the least often prioritised. COPM, Canadian Occupational Performance Measure.
Impairment of hand function
As shown in table 2⇓, hand mobility was restricted for all digits. With respect to flexion or opposition, the deficit was largest for digits I, II, and III, while the extension deficit was largest for the third and fourth digits. Compared with control values, grip strength was reduced to less than 60% of normal.27 Unfortunately, reduction of pinch strength could not be calculated, as normative values are not yet available for the Grippit instrument. Resisted motion was painful for both grip and pinch.
Impairment variables.
There were significant differences between the right and the left hand in extension deficits for the III, IV, and V fingers, abduction of the thumb, and grip strength. Although the impairments were most severe in the right hand, the grip was stronger in this hand.
Associations among personal factors, impairment, activity limitations, and participation restrictions
The hierarchical multiple regression models are presented in table 3⇓. The personal variables were entered as block 1 and accounted for 18% of the variation in the AUSCAN function score. The contribution of this block was significant (p<0.002).
Predictors of function in hand related activities (AUSCAN), in occupational performance (COPM performance), and in satisfaction with occupational performance (COPM satisfaction) in women with hand osteoarthritis (hierarchical regression analysis)
The impairment variables were added into the model as block 2, and constituted the greatest contribution to the explanation of the dependent variable, with an additional 37% (p<0.001). The most important variables were grip force in pinch grip (p<0.01), and pain during resisted motion (pinch grip) (p<0.01). The final model (with two blocks) explained a total of 55% of the variation in the AUSCAN function scores (p<0.001).
However, repeating the analysis with the COPM performance score and the COPM satisfaction score as dependent variables revealed different results (table 3⇑). In these analyses, the block with personal factors constituted the greatest and significant contribution to the explanation of the dependent variables. The model with the COPM performance score as dependent variable had an explanatory power of 32% (p<0.001), with self efficacy function as the most significant variable (p = 0.004), while the model with the COPM satisfaction score had an explanatory power of 39% (p<0.001), with disease duration, comorbidity, self efficacy function, and hand power in pinch grip as the four significant variables.
DISCUSSION
The results of this study confirm that hand osteoarthritis has considerable functional consequences. On the impairment level, the patients had reduced hand mobility and grip force, and resisted motion was painful. Further, the patients described problems in many domains of activity and participation. The regression analyses revealed that the relations among different aspects of functional dimensions are complex, as hand related activity limitations seem to be closely associated with hand impairment, while performance and satisfaction within a broader spectrum of activity and participation are more influenced by personal factors. As a result, rehabilitation programmes should have multidimensional aims, such as reducing hand impairment, improving occupational performance, and enhancing the self efficacy and coping strategies of the individual. The present findings thereby support the proposals from other investigators—that most patients with osteoarthritis will benefit from multidisciplinary care to help relieve symptoms and improve function.38–,42
The most commonly reported and prioritised occupational problems were connected to personal care, household chores, mobility, and leisure activities, a finding also recognised in other studies.5,43 Studies of persons with rheumatoid arthritis have shown that reduced ability to perform recreational activities and engage in social interactions were linked to the onset of new depressive symptoms, and further that satisfaction with abilities seems to mediate the relation between the disease impact on valued activities and an increase in depressive symptoms.44,45 To be able to address this in care, it is important to assess not only functional decline but also how such limitations are experienced by the individual.
When defining specific hand related problems, the activities requiring considerable grip strength combined with twisting of the hands were described as the most difficult to perform (fig 1⇑). These are the same problems most commonly described by women with rheumatoid arthritis,46,47 and are activities where the forces at the finger joints are extremely high, thereby causing discomfort.48 In patients with rheumatoid arthritis, the use of technical aids has been found to reduce pain and increase the capacity and ability to perform activities of daily living.46,47,49 The possession and use of such devices are common also among persons with osteoarthritis.50,51 Future research should therefore be aimed at investigating the effect of assistive devices in these patients. The functional consequences of hand osteoarthritis in men should also be further investigated, as the participants in this study were all women.
In this study, the impairment variables in the regression analysis were chosen to reflect the functional limitations of the typically most impaired joints in hand osteoarthritis, namely the DIP and PIP joints of digits II–V and the thumb. In the hierarchical regression analysis, hand impairment explained 37% of the variations in the AUSCAN score. Associations among hand related activity limitations and hand impairment such as pain, reduced mobility, and reduced grip strength are also recognised in other studies.52,53 Hand power seems to be the most stable contributing factor in explaining both the variation in hand related activity problems and the broader aspects of activity and participation. Home hand exercises and joint protection have been found to be effective means of increasing grip strength and global hand function in patients with hand osteoarthritis.54 These patients should therefore be encouraged to engage in exercises and activities that enhance hand function.
As the thumb is said to contribute 60% to the overall function of the hand,55 considerable attention should be offered to compensate or improve function in this digit. A successful form of conservative treatment addressing this problem is splinting the thumb, which in several studies has proved to be a well tolerated intervention to decrease pain, increase stability, and improve function in daily activities.48,56,57
About 55% of the variation in the AUSCAN scores and 30–40% of the variation in the COPM scores was explained by the independent variables studied. One reason for this difference may be the broader scope of the COPM, also capturing activity limitations and participation restrictions caused by comorbidity or osteoarthritis in other locations. Thus it is likely that COPM scores reflect more the overall participation restrictions than restrictions caused by hand osteoarthritis. Also, as both the AUSCAN and the COPM have an individual focus, the physical, social, and attitudinal barriers in the patients’ environment are not fully captured. Some of the remaining explanatory factors may thus be related to such environmental conditions. In a broader sense, this also indicates that successful rehabilitation depends not only on medical treatment and individual functional improvement, but also presupposes societal changes.58
A limitation of the study is, however, the cross sectional design, which only allows investigation of associations among dimensions of functioning. Future studies with longitudinal design are needed to be able to draw more firm conclusions on cause and effect relations.
Conclusions
Hand osteoarthritis has considerable functional consequences in terms of pain, reduced hand mobility, reduced grip force, and problems in many domains of activity and participation. Regression analyses showed that hand related activity limitations seem to be closely associated with hand impairment, while performance and satisfaction within a broader spectrum of activity and participation are more influenced by personal factors. As a consequence, rehabilitation programmes should be both multidisciplinary and multidimensional, aiming at reducing hand impairment, improving occupational performance, and enhancing the self efficacy and coping strategies of the individual.
REFERENCES
Footnotes
Published Online First 13 April 2005