Article Text

Abstract
Objective: To investigate outcome as measured by health status, disease process, and damage in an unselected group of patients with early rheumatoid arthritis (RA) monitored prospectively for 10 years and to search for prognostic factors.
Patients and methods: 183 patients with RA with disease duration <2 years were assessed annually at a team care unit. Health status was measured by the Health Assessment Questionnaire (HAQ) and functional class. Disease process was assessed by clinical and laboratory measures of disease activity and evaluation of disease course. Damage was quantified as occurrence of major extra-articular manifestations and need for large joint replacements. Possible predictive factors were evaluated by logistic regression analyses.
Results: 168/183 patients completed the entire follow up period. Of all 183 patients, 137 (75%) had been treated with disease modifying antirheumatic drugs and 84 (46%) with low dose oral glucocorticoids. After 10 years 158 patients (94%) managed daily life activities independently (functional class I–II). As measured by the HAQ 20% had almost no disability, 28% were mildly disabled, and 10% were seriously disabled. Median HAQ score had increased from 0.8 to 1.1 (p<0.001). Disease activity was significantly reduced. 133 patients (79%) had a relapsing remitting disease course and 30 patients (18%) were in remission as defined by the American College of Rheumatology criteria. Thirty patients (17%) had undergone large joint replacements. Fifteen patients (8%) had developed major extra-articular complications. The HAQ score during the first three months predicted disability at 10 years with an odds ratio of 13.4.
Conclusions: Prospective studies such as this give important knowledge of the variable long term prognosis of RA and provide necessary background information for clinical trials of new treatment modalities.
- rheumatoid arthritis
- outcome
- prognosis
- function
- ACR, American College of Rheumatology
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- FC, functional class
- HAQ, Health Assessment Questionnaire
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- VAS, visual analogue scale
Statistics from Altmetric.com
- ACR, American College of Rheumatology
- DMARD, disease modifying antirheumatic drug
- ESR, erythrocyte sedimentation rate
- FC, functional class
- HAQ, Health Assessment Questionnaire
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- VAS, visual analogue scale
Rheumatoid arthritis (RA) is a condition which has great impact on all aspects of life for those affected from disease onset and onwards. The patients have both joint related symptoms such as stiffness and pain as well as general malaise and tiredness and their physical and psychosocial function may deteriorate rapidly. However, the disease course in RA varies considerably. Several longitudinal studies of patients with RA with more than five years follow up have been presented.1–10 The outcome reported varies, which may be explained by the application of different outcome measures as well as differences in patient selection.1,2,5,6,8,9 Cultural differences may also influence interpretations.11
Various measures to evaluate outcome of RA are available. Clinical and laboratory indices of disease activity are generally emphasised. However, in long term follow up studies these measures are not necessarily the most important.12
At the fourth OMERACT conference in Mexico in 1998, five core domains were identified and recommended for use in longitudinal observational studies of patients with RA.13 These core domains were health status, disease process, damage, toxicity/adverse reactions, and mortality.
In the prospective Lund observational study of patients with newly diagnosed RA,14 the patients have now been evaluated 10 years after inclusion in the study. We have previously reported the outcome in two of the core domains, health status as measured by psychosocial function15 and mortality.16
In this report we describe health status reflected by physical function, disease process assessed by measures of disease activity, and disease course. Damage was assessed by large joint destruction requiring joint replacement and occurrence of severe extra-articular manifestations. We also evaluate possible predictors for the 10 year outcome of these features.
PATIENTS AND METHODS
Patients
The patients are all taking part in a prospective study of patients with early RA initiated at Lund University hospital in southern Sweden in 1985. Inclusion criteria for this study were definite RA according to the 1958 American Rheumatism Association criteria, age over 18 years, and disease duration less than 24 months. Disease duration was defined as the time from the onset of symptoms. Most patients were referred from primary care as a result of a special campaign to recruit patients with recent onset of symptoms. The study comprises 183 patients (67 men, 116 women) with a mean (SD) age of 51.4 (12.4) years at disease onset. Mean (SD) duration of joint symptoms at inclusion in the study was 11.1 (6.1) months. The patients were included between 1985 and 1989. The patients were assessed at least once a year at a team care unit including rheumatologist, nurse, physical therapist, occupational therapist, social worker, and orthopaedic surgeon. More frequent visits were often required for clinical reasons such as increased disease activity and monitoring of treatment with disease modifying drugs.
Evaluation of health status
The patients estimated pain, during the week preceding the visit, on a visual analogue scale (VAS, 100 mm). To facilitate the comparison with the Health Assessment Questionnaire (HAQ) scores, the VAS value in millimetres was multiplied by three and then divided by 100, thus giving a range of 0–3.
Functional class (FC) was classified according to Steinbrocker et al.17 Disability was evaluated using a validated Swedish version of the Stanford HAQ disability index.18 The range of the HAQ score is 0–3.0. Patients were classified as mildly disabled with a score of 0–1, moderately disabled with a score of 1.01–2, and severely disabled with a score >2.19
Evaluation of disease process
Joint inflammation was assessed by an active joint count, defined as swollen and either tender or painful on motion. The 50 joints evaluated in the active joint count included all but two from the Ritchie index—namely, the neck and subtalar joints. Patients' assessment of morning stiffness was defined as the average duration in minutes during the past week.
The erythrocyte sedimentation rate (ESR) was evaluated according to Westergren. Rheumatoid factor of IgM class was analysed with an enzyme linked immunosorbent assay (ELISA).20 HLA-DRB alleles were typed by restriction fragment length polymorphism analysis with sequence specific primers as previously described.21
The disease course was regarded as relapsing remitting if the patient had no active joints on examination at least at one follow up visit, and persistent if the patient had active joints at all evaluation points. Remission was defined according to the ACR criteria.22 Because we did not record fatigue, remission was considered present if four of the remaining five criteria were fulfilled.
Evaluation of damage
Joint surgery and occurrence of extra-articular manifestations, as well as the presence of nodules, were registered continuously. If nodules were present at two or more consecutive evaluation visits, the patients were considered to have nodular disease. If patients showed symptoms of extra-articular disease, appropriate examinations were performed. Table 1 shows the methods for diagnosing the extra-articular manifestations.
Registered severe extra-articular manifestations and methods used for diagnosis, according to the organ systems affected
Statistical analysis
Non-parametric tests were used. Differences between groups were analysed by Mann-Whitney's test, Wilcoxon's test, or χ2 tests when appropriate.
Logistic multiple regression was applied to try to find predictors of outcome in different domains after 10 years. A forward stepwise approach was applied. The validity of the obtained models was tested by the goodness of fit and model χ2. Exponent B in the regression model could be interpreted as an odds ratio and the 95% confidence interval for this factor was therefore also calculated. All tests were two tailed and limit value for significance was set at p<0.05.
RESULTS
Patients
One hundred sixty eight of the 183 patients were still monitored after 10 years. Of the other 15 patients, nine had died. Five deaths were caused by heart disease, three by malignant disease (two in the lung and one in the uterus), and one by alcohol intoxication.16
Six other patients were lost to follow up. Of these, four had moved to other areas, one had stopped attending owing to psychiatric disease, and one did not want to participate because of old age. This female patient was followed up for six years and was in remission during the last two years. She is still alive at age 93. No significant differences in baseline variables were found between the 15 patients not followed up for 10 years and the patients completing the 10 year follow up. Data from all patients are included in the description of the disease course.
Seventy five per cent of the patients were rheumatoid factor (RF) positive. Of the 170 genotyped patients, 145 (85%) carried the shared epitope. Fifty four (32%) carried the epitope on both alleles.
Patients with active disease were offered disease modifying antirheumatic drug (DMARD) treatment and 137/183 (75%) patients received such treatment during 57% of their follow up time. Fifty eight patients received one drug, 35 two drugs, 25 three drugs, 10 four drugs, and 9 were given five to seven different DMARDs. Table 2 shows the frequency of different DMARDs used during the entire study period. Low dose oral glucocorticoids were given to 84/183 (46%) of the patients and median (interquartile range) 14 (6–25) intra-articular glucocorticoid injections were given during the study. At the 10 year evaluation 87 patients (52%) were treated with DMARDs. Methotrexate was the most frequently used drug (23%) at that time. At the 10 year visit 52 patients (31%) were treated with low dose oral glucocorticoids, 30 of these in combination with DMARDs.
The different DMARDs used during the study period
Health status
Figure 1 shows the distribution of FC over time. After 10 years most patients were in FC II while 16 patients remained in FC I. There were eight patients in FC III and two in FC IV.

Functional class distribution according to Steinbrocker at study start and years 1, 5, and 10.
Figure 2 shows the changes in HAQ and VAS pain score over time. The median HAQ increased significantly from 0.8 at the study start to 1.1 after 10 years (p<0.001), whereas the VAS pain score remained unchanged.
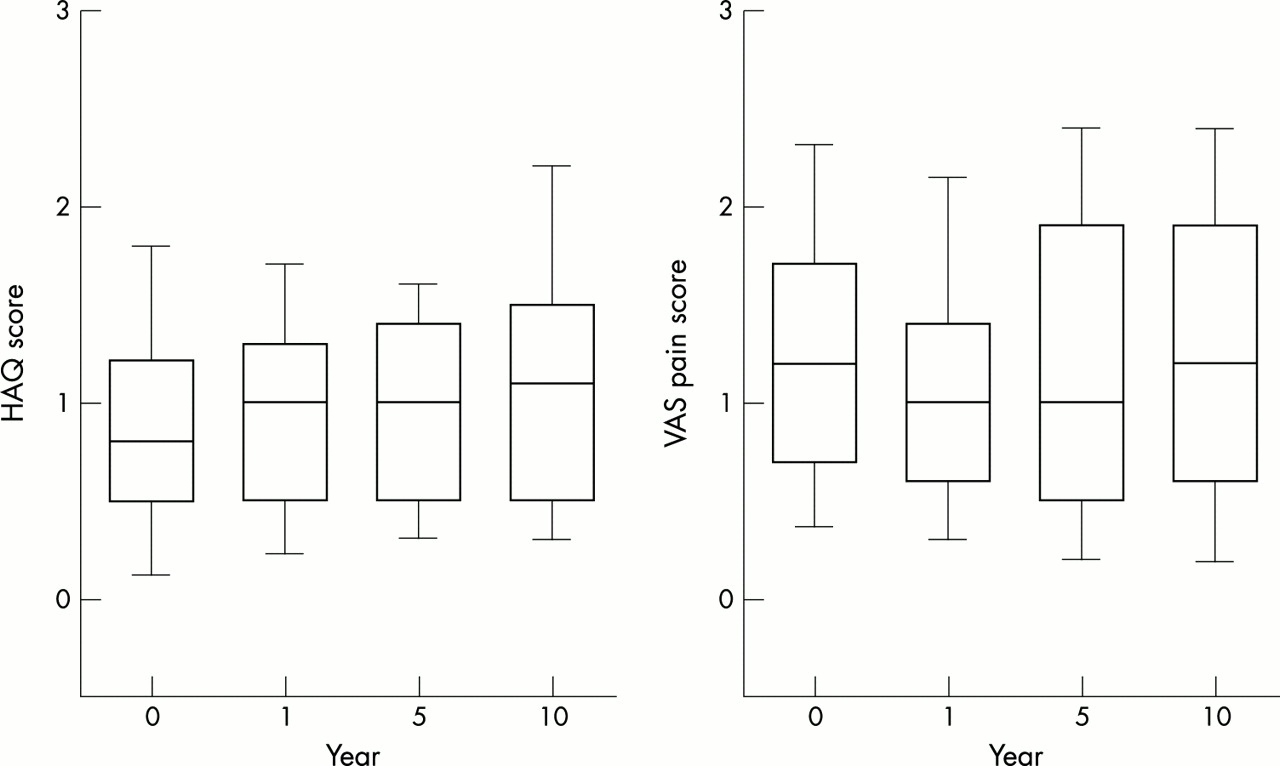
HAQ and VAS pain at the study start and years 1, 5, and 10. The box plots show the median and 10th, 25th, 75th, and 90th centiles.
Figure 3 shows the distribution of HAQ scores at the 10 year follow up. Seventy nine patients (47%) had an HAQ score <1.01 and were considered mildly disabled and of these, as many as 33 patients (20%) had almost no disability at all (HAQ <0.5). In contrast, 16 patients (10%) were severely disabled (HAQ>2).
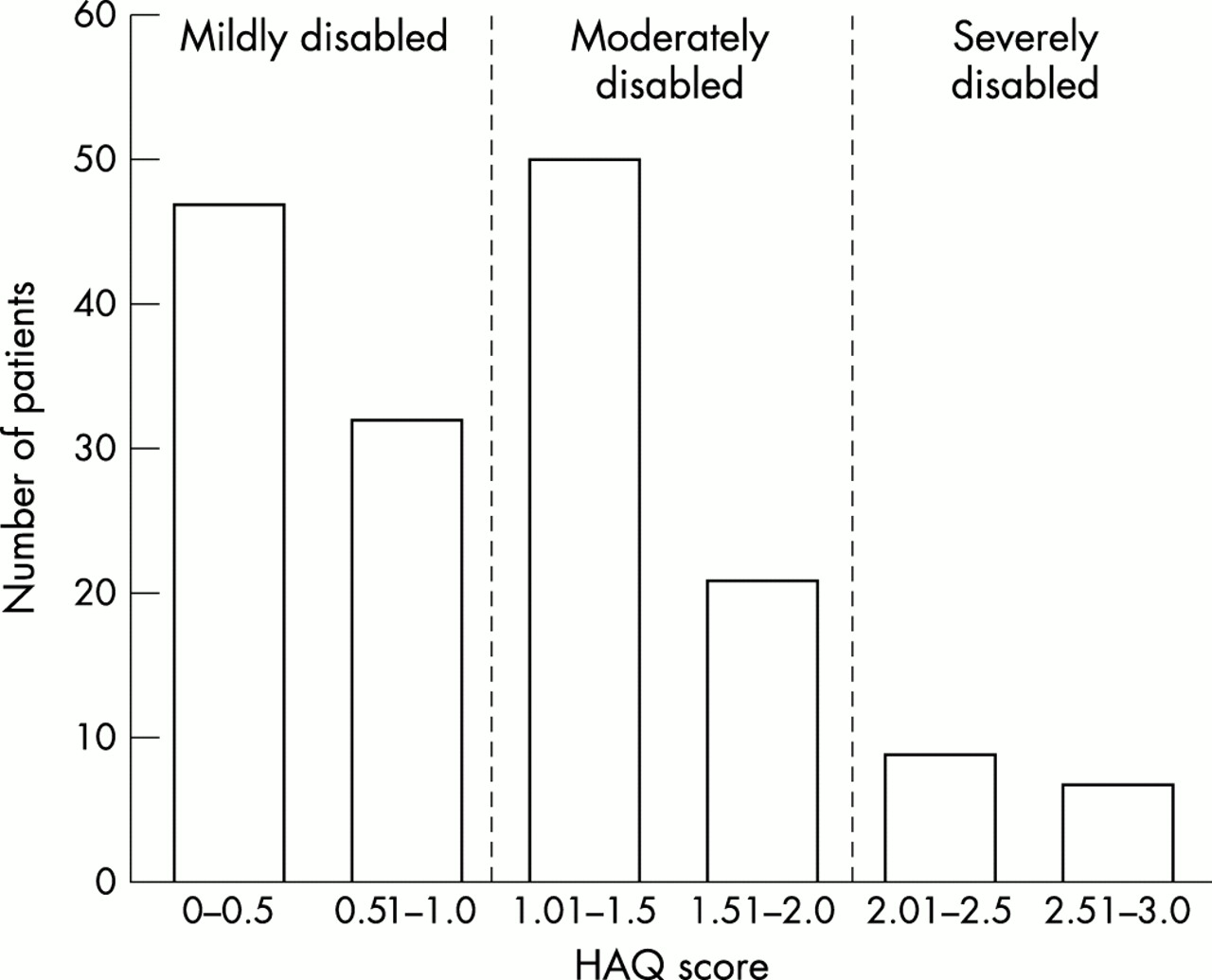
Distribution of HAQ scores after 10 years.
Disease process
Figure 4 shows the development of ESR and active joint count over 10 years. Morning stiffness had decreased from 60 minutes at the study start to 30 minutes at years 5 and 10. All measures of disease activity decreased significantly during the study time (p<0.001, Wilcoxon's test).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Active joint count and ESR at the study start and years 1, 5, and 10. The box plots show the median and 10th, 25th, 75th, and 90th centiles.
The 23% patients not receiving DMARDs during the entire study period had significantly lower disease activity and better functional ability at all evaluation points.
The disease course was relapsing remitting for 133 patients (79%). Of the 35 patients with continuously active disease, all except one were women. Patients with relapsing remitting disease had a significantly lower HAQ (p=0.013) after 10 years than the patients with continuously active disease.
At the 10 year follow up visit 30 (18%) patients (12 men, 18 women) were in remission. The median time spent in remission was 13 months (range 2–100). Twelve of the 30 patients in remission were treated with DMARDs.
Damage
Thirty patients (17%) needed arthroplastic surgery during the study period. Radiographic damage in joints needing replacement was maximal. In total, arthroplasties were performed in 28 hips, 12 knees, and five shoulders. Five patients underwent bilateral hip replacements, two bilateral knee replacements and one bilateral shoulder replacement. Three patients obtained arthroplasties in three different joints. Three operations were revision arthroplasties (two hips and one knee). The mean duration (SD) from inclusion in the study to surgery was 69 (33.8) months. Joint replacements were more common in male patients (p=0.041), and in patients who carried a double dose of the shared epitope (p=0.038). The patients who obtained arthroplasties had significantly higher mean (at study start and at three months) ESR (p<0.0001) than patients not needing replacements. Twenty eight of the 30 patients needing arthroplasties were followed up for 10 years and 25 remained in FC I–II while two were in FC III and one in FC IV. The patients in FC III–IV had all only received one joint replacement. Five of the patients operated on had HAQ scores >2 while seven had HAQ scores up to 1.
Seventy patients (38%) had nodular disease. Fifteen patients (8%) developed serious extra-articular manifestations. Table 1 lists these manifestations. Nodules were significantly more common among the patients with serious extra-articular manifestations (p=0.003); 12/15 patients had nodular disease.
Prediction
In the logistic regression analyses we tried to predict outcome after 10 years for remission, disability (cut off value HAQ score 1), extra-articular manifestations, and joint replacement, respectively. Age, sex, genotype, RF, HAQ, ESR, and active joint counts from the first months of the studies were used as independent variables in all the different regression models.
With this approach it was only possible to predict outcome with acceptable accuracy in one domain—namely, health status as assessed by the HAQ. The patients could be correctly classified into the two categories, mildly disabled or not (HAQ 1 or more), in 70% of the cases. Mean HAQ during the first three months was the only significant variable in the model. The odds ratio was 13.36 with 95% confidence interval 5.08 to 35.14. A separate explanatory model, in which DMARD treatment or not was included among the independent variables, showed that such treatment had no significant influence on disability.
The models obtained to predict remission, extra-articular manifestations, and joint replacement only reached a correct classification in 0–7% of the cases.
DISCUSSION
Most patients in this study were recruited from primary care and patients were included irrespective of disease activity and severity. We have therefore been able to monitor prospectively patients representing a spectrum from mild to very severe cases, which should strengthen the relevance of the results. During the 10 years only a few—six (3%) patients—dropped out, which further reduces the selection bias.
Some striking observations emerge in this study. Ninety four per cent of the patients were after 10 years still in FC I–II and were thus able to perform daily life activities independently. According to the HAQ half of the patients were mildly disabled and 20% were scarcely disabled at all. Also patients needing joint replacements generally maintained their functional ability well.
Two British studies starting in the 1950s and 1960s reported a higher proportion of patients with definite RA in functional class III–IV after a follow up time of up to 15 years.1,7 One explanation for the better functional outcome among our patients might be the change of treatment strategy towards early and more active treatment beginning in the 1980s. Another reason might be that our patients received team care, which was not fully developed in earlier days. One Finnish study with a follow up time of a mean 6.2 years had about the same number of patients in FC III–IV as we did.9 On the other hand, more of their patients were in FC I, which might be because of their more aggressive treatment strategy where all patients received DMARDs from the study start.
The patients in our study had higher absolute level of HAQ scores from the start and throughout the study, than reported by some9,10 but not all5 other investigators. One reason for this might be the scoring system, automatically giving a higher HAQ value if aids or appliances are used. Owing to the social security system in Sweden and also the fact that they had team care, our patients were generously provided with aids and appliances from early disease. However, it is notable that the deterioration of HAQ over time was similar in all studies.5,9,10
Importantly in our study the patients with relapsing remitting disease course had a better outcome as measured by the HAQ than the patients with continuously active disease. Thirty one additional patients had acquired relapsing remitting disease between years 5 and 10,23 which implies that active treatment is worthwhile throughout the disease course.
We found a remission rate of 18% at the 10 year evaluation using the ACR criteria for remission. This is in accordance with some earlier findings,24,25 while in Finland9 the remission rate was considerably higher—32% of the patients were in remission after 6.2 years. Patient selection, treatment strategies, and length of follow up might be reasons for the differences.
Major joint replacements were performed in 17% of our patients. A similar frequency was reported by Wolfe and Zwillich,26 while in Finland only 7% underwent large joint replacements during the first six years.9 The differences in frequency of large joint replacements between countries might be due to variations in indication for surgery as well as differences in availability of orthopaedic surgery. The shorter follow up time in the Finnish study might play a part in their lower number of joint replacements, as the mean duration of disease at the first joint replacement in our study was six years. We found that high ESR at the study start, male sex, and a double dose of shared epitope were more common among the patients needing surgery. This is partly supported in the study by Wolfe and Zwillich, who reported that high ESR but also high HAQ scores were associated with an increased risk for joint replacement.26
Nodular disease was common among our patients. A similar prevalence of nodular disease was presented by Corbett et al, 7 whereas in other studies nodular disease was less common.8,9 An awareness of nodules was very high in our study as we registered the presence of nodules or not at each visit.
The frequency of extra-articular manifestations corresponds to findings in a previous Swedish retrospective study,27 while others have shown lower frequencies.28 However, Young et al showed about the same frequency of extra-articular manifestations after five years in their follow up of patients with RA from the 1990s,29 as we did after 10 years. Differences in reported frequencies of extra-articular manifestations may be due to patient selection and different methodologies. Despite the relatively high frequency of major extra-articular manifestations, mortality was not increased in this cohort.16
As might be expected it was difficult to predict outcome in different domains after 10 years. One exception was health status where HAQ during the first three months had strong predictive power with an odds ratio of 13.4. This suggests that treatment aiming at improvement of HAQ in the early phases of the disease might improve functional outcome of RA both in the short and long term. We have previously shown the predictive value of HAQ for the level of disability after two and five years14,30 and it is a notable observation that this still holds true even after 10 years. The HAQ has in other investigations been shown to have prognostic value not only for functional outcome but also for very important outcome features such as work disability15 and mortality.19 At a first glance the HAQ seems a rather simple measure of disability. However, the fact that it is a self administered questionnaire might add other important dimensions—for example, related to the patient's personality and emotional status, which may to some extent explain its robust prognostic value.
Longitudinal observational studies of patients with RA such as the present one provide important insights into the course and prognosis of RA and form a reference source for design and performance of clinical trials.
Acknowledgments
Grants were obtained from the Swedish Medical Research Council, the Österlund and Kock Foundations, the King Gustaf V 80 year Fund, and Reumatikerförbundet.