Article Text

Abstract
OBJECTIVE To provide data on (a) the probability of detecting antinuclear antibodies (ANA) in a large and consecutive cohort of serum samples referred for ANA testing and (b) the probability of detecting more specific antinuclear reactivities (anti-DNA and anti-extractable nuclear antigens (anti-ENA)) in serum samples with a positive screening test (indirect immunofluorescence on HEp-2 cells).
METHODS Serum samples from 10 550 consecutive patients sent to the laboratory for ANA detection were analysed. In ANA positive serum samples (23.5% of referred serum samples), ANA were identified by indirect immunofluorescence on Crithidia, by immunodiffusion, and by line immunoassay. Because anti-SSA antibodies were the most frequently identified ANA, sensitively detected by line immunoassay, additional immunoassays were developed to confirm the specificity of the line immunoassay result.
RESULTS At least one fine reactivity could be identified in 21.1% of ANA positive serum samples: anti-dsDNA in 3.2%; anti-ENA (anti-SSA 10.5%, anti-SSB 6.7%, anti-RNP 2.7%, anti-Sm 1.8%, anti-Scl70 1.2%, anti-Jo-1 0.2%) in 15.8%, rRNP and anti-Cenp-B in respectively 0.5% and 4.0%. Multiple reactivities were found in 7.9%. For anti-ENA antibodies, line immunoassay was more sensitive than immunodiffusion (15.4%v 7.7%; p<0.0001). The sensitive detection of anti-SSA antibodies by line immunoassay was confirmed by additional assays.
CONCLUSIONS The data from this analysis are useful in estimating the probabilities of detecting specific ANA. Line immunoassay was shown to be a sensitive test for the detection of anti-ENA antibodies.
- antinuclear antibodies
- line immunoassay
- anti-SSA antibodies
Statistics from Altmetric.com
A humoral autoimmune response is a common manifestation of the rheumatic connective tissue diseases (CTD) and often includes antinuclear antibodies (ANA).1 Indirect immunofluorescence (IIF) on HEp-2 cells is the classically used technique for the detection of ANA.2 Positive fluorescence staining indicates the presence of ANA but does not allow precise identification of these autoantibodies. For that purpose, additional testing is required, employing techniques such as immunoprecipitation in agar, western immunoblotting, enzyme linked immunosorbent assay (ELISA) or, the more recently developed, line immunoassay.1 ,3 ,4 Because a characteristic profile of ANA is associated with most CTD, identification of the fine specificity may provide valuable clues to the diagnosis. Indeed, the presence of anti-dsDNA or anti-Sm antibodies is quite specifically associated with systemic lupus erythematosus (SLE); anti-Scl70 and anticentromere antibodies with systemic sclerosis (diffuse and limited cutaneous disease respectively; anticentromere antibodies, however, can also be seen in patients without this disease); anti-Jo-1 with polymyositis. Anti-SSA and anti-SSB antibodies have a broader spectrum of associated CTD, including Sjögren's syndrome (SS), lupus (systemic and cutaneous form), scleroderma, and rheumatoid arthritis (RA). Anti-RNP antibodies have been associated with the so-called mixed connective tissue disease (MCTD), but may be found in other rheumatic connective tissue diseases as well.1
In this study we analysed a large and consecutive cohort of serum samples referred to our laboratory for ANA testing. In ANA positive samples, further identification of the fine reactivity of these antibodies was obtained with IIF onCrithidia (for the detection of anti-dsDNA antibodies), and by immunodiffusion and line immunoassay (for detection of anti-extractable nuclear antigens (anti-ENA antibodies)).
The present analysis aimed at providing data on (a) the probability of detecting ANA in a large and consecutive cohort of serum samples referred for ANA testing and (b) the probability of detecting more specific antinuclear reactivities (anti-DNA and anti-ENA) in serum samples with a positive screening test for ANA (IIF on HEp-2). Because anti-SSA antibodies were the most frequently identified antinuclear autoreactivity, sensitively detected by line immunoassay, additional immunoassays were developed to confirm the specificity of these results.
Patients and methods
PATIENTS
A total of 15 937 serum samples from 10 550 consecutive patients sent to the rheumatology laboratory (Ghent University Hospital) over a three year period (1996–99) for ANA testing were included in this study. The serum samples were referred by in-house specialists, including rheumatologists (25% of the serum samples), internal medicine specialists (15%), gastroenterologists (7%), dermatologists (5%), neurologists (5%), nephrologists (3%), and external hospitals or laboratories (23%). When multiple serum samples from a single patient were received during this time, only the data for the first serum sample were used in this analysis. For most ANA positive samples (80.1%) further identification of the antibodies was requested and performed by second line tests, including IIF onCrithidia, immunodiffusion with thymus/spleen nuclear extract, and line immunoassay with recombinant and purified nuclear antigens. In a selected group of serum samples, additional tests were performed to confirm the anti-SSA reactivity detected by line immunoassay.
INDIRECT IMMUNOFLUORESCENCE ON HEP-2 AND HEP-2000 CELLS
Serum diluted 1/40 in phosphate buffered saline (PBS) was overlaid onto fixed HEp-2 cells (MeDiCa Inc, Carlsbad, Ca) for 30 minutes at room temperature. Slides were washed twice for five minutes each with PBS, overlaid with fluorescence labelled conjugate, which is antihuman IgG heavy and light chain specific (MeDiCa), and incubated for an additional 30 minutes. After washing twice, a coverslip was placed over the slide, and the slides were read using a fluorescence microscope at ×40 power. The fluorescence intensity was scored semiquantitatively from 1+ to 5+ relative to the intensity of a negative and a positive (4+) control.2 The main fluorescence patterns seen were speckled, homogeneous, nucleolar, and centromere. A selected set of serum samples was also analysed by indirect immunofluorescence on the commercially available HEp-2000 (Immunoconcepts, Sacramento, CA), for confirmation of anti-SSA reactivity. In this substrate, cells are transfected with Ro60 cDNA.5 Approximately 10–15% of these cells overexpress Ro60 in a nuclear and nucleolar distribution and can be easily identified from those expressing Ro60 at endogenous HEp-2 levels. Serum samples were incubated according to the manufacturer's instructions. The HEp-2000 result was reported as SSA positive if the characteristic speckled and bright nucleolar staining was present as described previously.5-7
INDIRECT IMMUNOFLUORESCENCE ON CRITHIDIA LUCILIAE
Crithidia luciliae coated slides (Immunoconcepts) were used for the detection of anti-dsDNA. Serum samples diluted 1/20 in PBS were incubated for 30 minutes at room temperature. Slides were washed twice for five minutes each with PBS, overlaid with fluorescence labelled conjugate, which is antihuman IgG heavy and light chain specific (MeDiCa), and incubated for an additional 30 minutes. After washing twice, a coverslip was placed over the slide, and the slides were read using a fluorescence microscope at ×40 power.
DOUBLE IMMUNODIFFUSION
Precipitating antibodies against ENA were detected by immunodiffusion in Ouchterlony plates using thymus/spleen nuclear extract (mammalian extracted nuclear antigen, Immunoconcepts) as antigen source. Antibody specificity was determined by comparison with an anti-SSA/Ro, anti-SSB/La, anti-Sm, anti-RNP, anti-Scl70, anti-Jo-1, and anti-proliferating cell nuclear antigen (anti-PCNA) reference serum. Immunodiffusion was also performed in a selected group of serum samples with natural SSA at 500 U/ml (Immunovision, Springdale, AR).
LINE IMMUNOASSAY
A line immunoassay coated with recombinant and purified nuclear antigens as discrete lines on a nylon strip with plastic backing was applied (INNO-LIA ANA K-1066, Innogenetics, Ghent, Belgium). Coated antigens included Sm-D, Sm-B, RNP-A, RNP-C, RNP-70K, Ro52, Ro60, SSB, Cenp-B, Topo-I/Scl70, Jo-1, and rRNP. The test was performed according to the manufacturer's instructions. Briefly, the nylon strips were incubated with serum at a 1/200 dilution. A goat antihuman IgG labelled with alkaline phosphatase was allowed to bind to the antigen-antibody complex. The enzyme substrate and chromogen 5-bromo-4-chloro-3-indolyl phosphatase (BCIP) produces a dark brown colour in proportion to the amount of specific autoantibody in the test sample. Sulphuric acid stops the colour development. This assay and a standardised cut off point have been validated in a multicentre study for the detection of anti-ENA antibodies.3 Furthermore, a research line immunoassay coated with natural SSA (Immunovision) was applied in a selected number of serum samples.
ELISA
Custom made ELISAs were obtained from Pharmacia Research and Development Laboratory (Freiburg, Germany) coated either with baculovirus-expressed recombinant Ro52 or with both Ro52 and Ro60 proteins in a 50/50 ratio. For the ELISA with baculovirus Ro52, the coated plates were incubated with or without reducing buffer (100 mM Tris-HCl, pH 6.8, 50 mM NaCl, 10 mM dithiothreitol) as described by Pourmand and Petterson8 for one hour at room temperature before the addition of antibodies.
IMMUNOBLOT ANALYSIS
Immunoblotting of E coli-expressed recombinant Ro60 and natural SSA (Immunovision) was performed in a selected number of serum samples, as previously described.3 Briefly, proteins were separated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis (SDS-PAGE) and transferred electrophoretically to nitrocellulose membranes. The filters were cut and incubated with patient serum samples diluted at 1/100. Bound IgG were detected by alkaline phosphatase conjugated, affinity purified goat antihuman IgG (Sigma, St Louis, MO, USA) diluted at 1/1000 and with the substrate nitroblue tetrazolium and BCIP (Sigma). Monoclonal antibodies against Ro52 and Ro60 (Cappel, OT, Turnhout, Belgium) were diluted (1/25) and detected with rabbit antimouse IgG (Sigma). HeLa S100 extract was separated on a 10% SDS-polyacrylamide gel with modified acrylamide:bisacrylamide ratio (172.4:1) to allow efficient separation of Ro52 and the La/SSB protein and blotted onto nitrocellulose.9
STATISTICS
A χ2 test was used to compare proportions. A p value <0.05 was considered significant.
Results
PREVALENCE OF ANA POSITIVITY, STAINING PATTERN, AND FLUORESCENCE INTENSITY
In total, serum samples from 10 550 patients, consecutively sent to the rheumatology laboratory for ANA testing were analysed. The prevalence of positive ANA testing in this population was 23.5%.
Table 1 shows the distribution of fluorescence patterns and fluorescence intensity scores in these ANA positive samples. The most prevalent fluorescence pattern was speckled (42.5%), followed by homogeneous (41.4%), nucleolar (10.6%), and centromere (3.9%).
Antinuclear antibody fluorescence patterns in relation to fluorescence intensity. Results are given as percentages
IDENTIFICATION OF FINE ANTINUCLEAR SPECIFICITY
1986 ANA positive serum samples were further analysed for identification of the fine antigen reactivity, by IIF onCrithidia, by immunodiffusion, and by line immunoassay. Figure 1 shows the identification of fine reactivities, as defined in table 2.
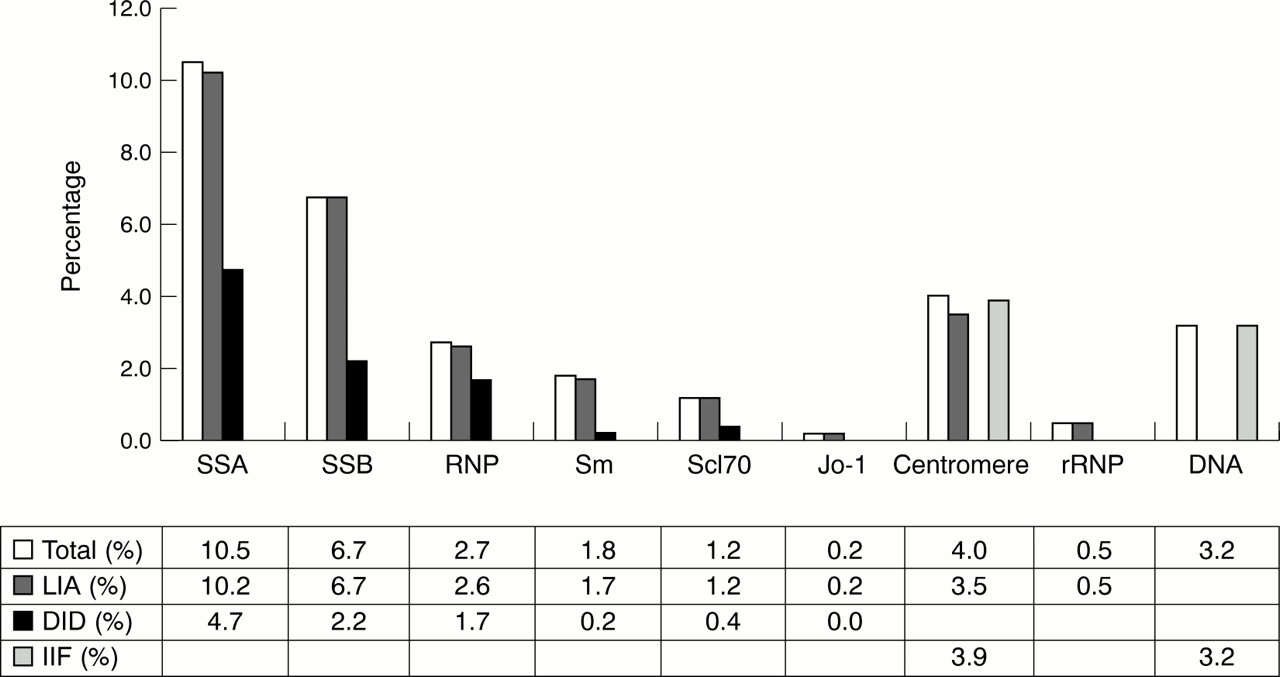
Identification of fine reactivities in ANA positive serum samples. LIA = line immunoassay; DID = double immunodiffusion; IIF = indirect immunofluorescence on HEp-2 cells (for anticentromere pattern) or Crithidia luciliae (for anti-dsDNA).
Definition of defined antinuclear antibody specificities
At least one fine reactivity could be identified in 21.1% of ANA positive serum samples: anti-dsDNA antibodies were identified in 3.2%; anti-ENA (anti-SSA, anti-SSB, anti-RNP, anti-Sm, anti-Scl70, anti-Jo-1) in 15.8%, anti-rRNP and anti-Cenp-B in respectively 0.5% and 4.0%. In a substantial number of patient serum samples, multiple reactivities were identified (two reactivities in 6.6%, three reactivities in 1.0%, more than three reactivities in 0.3%).
The most commonly identified antinuclear autoreactivity was directed towards SSA (10.5%) and SSB (6.7%). Table 3 presents the probabilities of detecting anti-dsDNA or anti-ENA antibodies (anti-SSA, anti-SSB, anti-RNP or anti-Sm) according to the fluorescence intensity and staining pattern. The stronger the fluorescence intensity in the initial ANA screening, the higher the detection rate of fine specificities. In the case of lower intensities, anti-SSA or anti-SSB, or both, were predominantly detected. When confronted with the strongest homogeneous patterns, anti-dsDNA antibodies were found in 36.6%, and anti-SSA/SSB antibodies in 26.8%. On the other hand, the strongest speckled patterns gave an indication towards anti-RNP (51.7%) and anti-SSA/SSB reactivity (34.5%). No other antibodies besides anti-SSA/SSB antibodies were found with the centromere pattern.
Probabilities of detecting anti-dsDNA or anti-ENA antibodies according to the fluorescence intensitity and staining pattern. Results are given as percentages
COMPARISON OF IMMUNODIFFUSION AND LINE IMMUNOASSAY FOR THE DETECTION OF ANTI-ENA ANTIBODIES
For the detection of anti-ENA antibodies, line immunoassay was clearly more sensitive than immunodiffusion (15.4 v7.7%; p<0.0001). Only a small fraction of serum samples showed a positive immunodiffusion result with a negative line immunoassay (9/314 patients).
The higher sensitivity could mainly be attributed to the earlier described better detection by this assay of anti-Ro52 and anti-SSB antibodies.3 The anti-SSA reactivity identified by line immunoassay (INNO-LIA ANA) and not by immunodiffusion was mostly confirmed by other assays (line immunoassay with natural SSA; immunodiffusion with natural SSA; SSA-specific staining pattern on HEp-2000 cells; immunoblot with natural SSA and recombinant SSA/Ro60; immunoblot with HeLa S100 extract; ELISA with recombinant SSA/Ro52 and SSA/Ro60) (table 4). Indeed, in the first group of 65 serum samples consecutively identified as anti-SSA positive by line immunoassay with E coli-expressed SSA/Ro52 and SSA/Ro60 (INNO-LIA ANA) and not confirmed by immunodiffusion with thymus/spleen nuclear extract, anti-SSA reactivity was confirmed by an additional test in 54/65 serum samples (83%) (table 4). The diagnoses in the cases where anti-SSA reactivity was not confirmed were as follows: autoimmune hepatitis (n=1), dermatomyositis (n=1), RA (n=2), SLE (n=1) (this patient also had anti-RNP antibodies), MCTD (n=1) (this patient also had anti-RNP antibodies), psoriatic arthritis (n=1), malignancy (n=1), and three patients with arthralgia, in whom no final diagnostic classification could be made.
Confirmation of anti-SSA reactivity detected by antinuclear antibody line immunoassay
Most of the additional anti-SSB reactivity was previously confirmed by immunoblot with recombinant or natural SSB.3 The observation that most of the anti-SSB antibodies identified by line immunoassay and not by immunodiffusion were found in combination with anti-SSA reactivity (74%) also provides strong evidence that these additional reactivities are real. We also found that these extra fractions were clinically relevant. The diagnostic distribution in the anti-SSA and/or anti-SSB positive population identified by line immunoassay but not by immunodiffusion with thymus/spleen nuclear extract included lupus (30%), scleroderma (18%), polymyositis/dermatomyositis (5%), primary SS (4%), and RA (18%).
Discussion
Autoimmune serology is an important tool in the diagnosis of a CTD. ANA are certainly among the most frequently ordered tests in this respect. Screening for ANA is widely performed by IIF on HEp-2 cells. We screen for ANA at a 1:40 serum dilution. This classifies virtually all patients with SLE and most patients with SS and scleroderma as ANA positive.10 We perform a typical cascade testing to detect specific ANA11 ,12: once ANA have been found, we use a more specific test to determine the fine specificity. However, there is no consensus about the best way to identify the fine specificity of ANA.
We report here on the probability of (a) detecting ANA in a consecutive cohort of patient serum samples referred to a routine university based rheumatology laboratory for ANA testing; and (b) identifying specific antinuclear reactivities (anti-dsDNA and anti-ENA antibodies) in ANA positive serum samples, using in parallel IIF onCrithidia, immunodiffusion with thymus/spleen nuclear extract, and line immunoassay with recombinant and purified nuclear antigens. Indeed, a positive ANA result itself has only weak predictive value for diagnosing SLE or other CTD, even in a group whose serum samples are specifically referred for ANA testing.13 ,14 Identification of more specific antinuclear reactivities significantly increases the predictive diagnostic value up to a level that is of real diagnostic value in specialist practice.
It is an interesting observation that in 23.5% of serum samples referred for ANA testing, the test was positive. The fluorescence pattern itself does not disclose the fine reactivity of the detected antibodies (except for anticentromere antibodies). However, the pattern may be indicative of the type of reactivities responsible for the IIF staining. In this study, anti-dsDNA antibodies are almost exclusively identified in serum samples with homogeneous ANA staining, with a probability ranging from 3.1% (fluorescence intensity score 3+) to 36.6% (intensity score 5+). Anti-ENA antibodies are more randomly distributed between different fluorescence patterns. It should be noted that the fluorescence pattern may result from the simultaneous occurrence of different ANA. In general, and as expected, anti-dsDNA and anti-ENA antibodies occur with the highest prevalence in serum samples with strong fluorescence staining, with the most notable exception of anti-SSA/SSB antibodies, which occurred in 5.6% of serum samples with minimal nuclear fluorescence (1+). Anti-Jo-1 reactivity was also confined to the lower intensities (3/4 anti-Jo-1 positive samples displayed a fluorescence intensity of 2+, 1/4 displayed a fluorescence staining of 3+). Jo-1 is a cytoplasmic antigen, and immunofluorescence with monospecific anti-Jo-1 serum samples discloses cytoplasmic staining. It is thus unlikely that the antinuclear fluorescence in these serum samples is related to anti-Jo-1 antibodies. Instead, this nuclear fluorescence is more probably related to a co-existing antibody.
The most prevalent specific ANA reactivities identified in this cohort are anti-SSA (10.5% of ANA positive serum samples) and anti-SSB (6.7% of ANA positive serum samples). Both reactivities often occur together, and we could determine that anti-SSA or anti-SSB antibodies, or both, are identified in 11.8% of ANA positive serum samples. An interesting observation is the fact that in 10% of the anticentromere antibody positive patients (identified by centromere pattern and/or line immunoassay), an additional reactivity—namely, anti-Ro52, is identified. The phenomenon of anti-Ro52 antibodies in scleroderma, without obvious concomitant anti-Ro60 antibodies, has recently been described by Frank et al.15They found anti-Ro52 antibodies in one of nine anticentromere serum samples that were screened, which is comparable with our result.
In conclusion, our study is useful in estimating the probabilities of detecting ANA and more specific anti-ENA and anti-DNA antibodies in serum samples referred to a rheumatology laboratory for ANA detection and identification. The main suggestions for the strategy of ANA identification, based on these data, are (a) line immunoassay is more sensitive than immunodiffusion for the detection of anti-ENA antibodies and may therefore replace immunoprecipitation as a second line test after immunofluorescence on HEp-2 cells; (b) low titre ANA are not necessarily insignificant, as they may contain anti-SSA antibodies; (c) anti-dsDNA antibodies should be checked systematically only in serum samples with strong homogeneous nuclear fluorescence, unless there is a very strong a priori suspicion for SLE.

{kind=link}
{kind=link}