Article Text

Abstract
New bone formation of the vertebral column is pathognomonic for ankylosing spondylitis (AS), while acute and/or chronic changes in the sacroiliac joints are relevant for diagnosis.
The ‘gold standard’ for assessment of structural changes in AS are conventional radiographs, while MRI is useful to assess inflammation. Recent MRI studies have shown that the lower half of the thoracic spine is most commonly affected in AS.
Scoring tools for spinal inflammation such as the ASspiMRI-a have been proposed, successfully used in large clinical trials and compared in a multireader experiment; none was finally preferred by OMERACT.
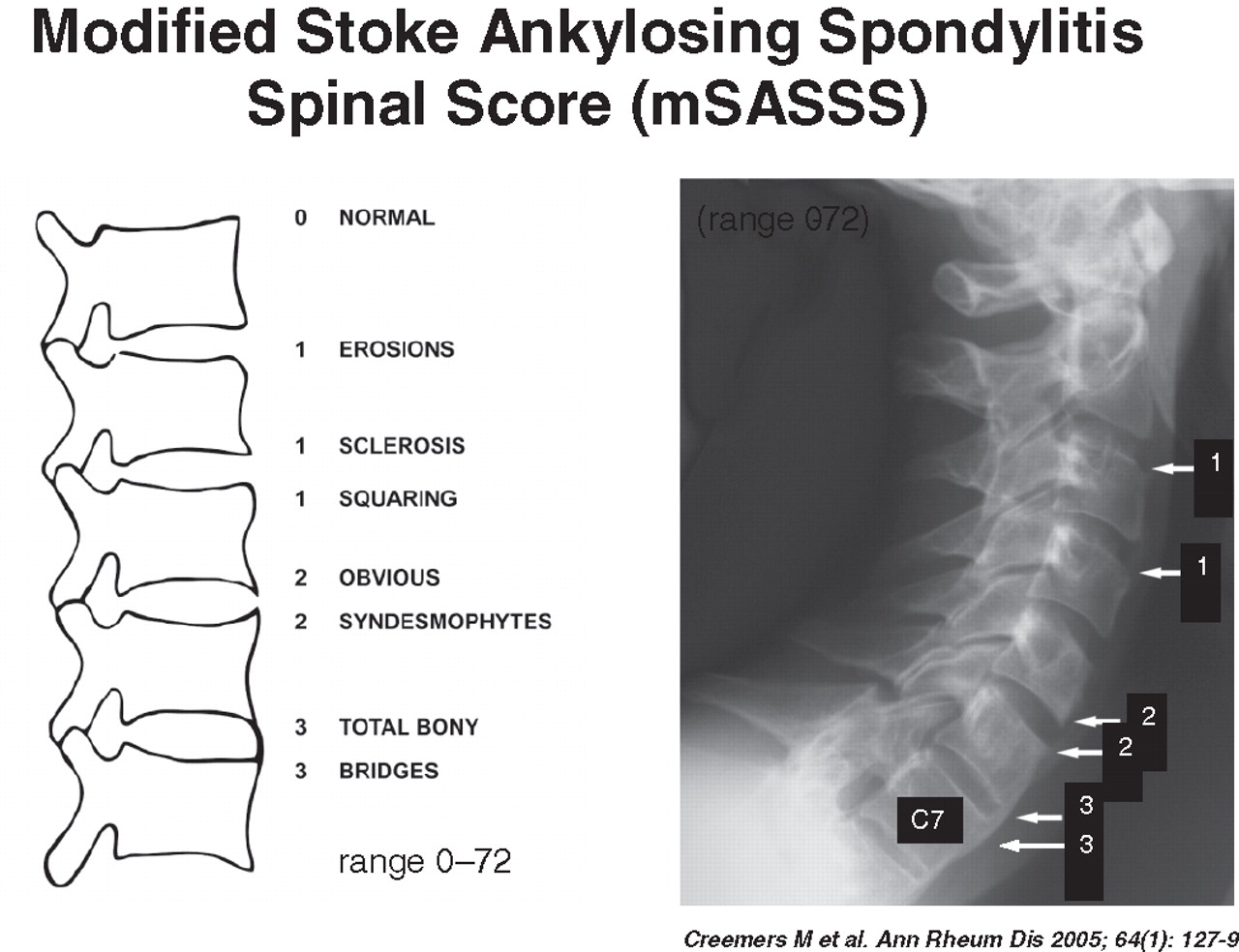
Quantification of structural spinal AS changes is performed by the modified Stokes AS Spine Score (mSASSS), which evaluates lateral cervical and lumbar radiographs. Two years was identified as the shortest possible follow-up time based on the reliability and sensitivity to change of the mSASSS. A potential disadvantage of the mSASSS is that the thoracic spine is not included. Recent data based on the mSASSS have suggested that tumour necrosis factor blockers do not inhibit radiographic progression in AS. Since the mean radiographic change is reported to be less than 1 syndesmophyte over 2 years, the sensitivity to change of the mSASSS has been questioned. However, in one study where continuous non-steroidal anti-inflammatory drugs use was compared with on-demand use, a difference between these two methods of drug intake was reported. The face and construct validity of the mSASSS has been criticised because a score of ´1´ contains a mixture of osteodestructive (erosions) and osteoproliferative changes (squaring and sclerosis). A new scoring system, the RASSS, which concentrates only on bone formation and which includes the lower part of the thoracic spine is currently being evaluated.
The relationship between inflammation and new bone formation in AS has recently been investigated. Low sclerostin and DKK-1 serum levels, both inhibitors of bone formation, were found to be associated with syndesmophyte formation in patients with AS.
Statistics from Altmetric.com
Introduction
Axial spondyloarthritis (SpA) including ankylosing spondylitis (AS) is a chronic inflammatory rheumatic disease that mainly affects the axial skeleton by causing inflammatory and osteoproliferative changes in the sacroiliac (SI) joints and spinal structures, which give rise to inflammatory back pain and stiffness.1 2 Axial SpA is an essential part of the spectrum of SpA (figure 1). Sacroiliitis, spondylitis, spondylodiscitis and spondyloarthritis are the main inflammatory manifestations,3 while syndesmophytes and ankylosis of the vertebral column are the characteristic findings indicating new bone formation.4 These pathognomonic structural changes tend to occur increasingly over time in the course of the disease but some patients have rapid progression.5 How inflammation and osteoproliferation are linked in AS is incompletely understood (see below).

The main concept of the spondyloarthritides (SpA) differentiates the main manifestations and the subtypes of SpA. The new term axial SpA covers both non-radiographic axial SpA and the classical ankylosing spondylitis (AS). The term ‘undifferentiated’ indicates absence of psoriasis, IBD and a triggering infection.
In addition to the typical osteoproliferative changes, patients with AS may also show osteodestructive changes, such as erosions, in both the SI joints and the spine.6 However, recent analyses have indicated that these changes occur rather infrequently in AS.4
Imaging of the spine has an important role in diagnosing, classifying and monitoring patients with AS and other SpA. While the bony changes are best identified by conventional radiographs,4 spinal inflammation is best assessed by MRI. Conventional radiographs of the axial skeleton are considered the ‘gold standard’ to identify and quantify structural changes in AS,3 but these can only depict structural changes and cannot directly visualise active inflammation. Nevertheless, definite structural changes in the SI joints but not of the spine are part of current classification criteria for AS. However, since involvement of the spine may, although infrequently, occur in the absence of definite structural changes in the SI joints, a diagnosis of AS in an individual patient may also be made when clear-cut syndesmophytes are present.3 Quantification and scoring of structural changes in the spine are major outcomes of clinical trials in AS, and different scoring systems have been proposed.7,–,9 There is increasing evidence that special chronic structural changes may also be detected by MRI.10 11
However, spinal MRI has been so far mainly used to detect and localise inflammatory rather than structural changes, and spinal MRI is currently considered a powerful tool to document treatment effects by detecting improvement, persistence or new onset of spinal inflammation in AS.12,–,14 Furthermore, spinal inflammation as detected by MRI is now increasingly used to predict the effect of antitumour necrosis factor α (anti-TNFα) therapy.15
The value of MRI for detecting structural changes in the SI joints and the spine is currently being further evaluated (see below).
Imaging as part of classification criteria
Conventional radiographs of the SI joints and the spine have been of critical importance for diagnosing AS for several decades. Definite structural changes of the SI joints have been part of the diagnostic and classification criteria for almost 50 years (figure 2).16,–,20 Usually, a grading of 0–4 is used with bilateral changes ≥2 being considered critical for the diagnosis of AS.21 Sclerosis, erosions and ankylosis are the major findings. The complicated anatomy of the SI joint and the two-dimensional capacity of conventional radiography are known to cause problems in the differentiation of doubtful cases.22 With increasing age, degenerative changes of the SI joints become more prevalent and the differential diagnosis more problematic.23 CT is considered the gold standard for assessing structural changes in SI joints.24 However, conventional radiography is usually performed for screening purposes. The decision, whether a pelvic x-ray examination or a lumbar spine anteroposterior view is obtained for assessing the SI joints, is made on an individual basis. MRI may be added in doubtful cases.22

The modified New York criteria for classification of patients with ankylosing spondylitis (AS): one out of three clinical criteria plus the radiological criterion have to be present (van der Linden et al21). SI, sacroiliac.
The typical spinal changes in AS are syndesmophytes, which may be difficult to differentiate from spondylophytes in DISH and other degenerative spinal diseases.4
The new classification criteria for axial SpA (figure 3) have recently included sacroiliac inflammation as detected by MRI as a major criterion in the imaging part of this set.25 Therefore, it has been necessary to define a ‘positive MRI’ for the SI joints (figure 4).26 In addition, structural changes in the SI joints may also contribute to a diagnosis of axial SpA.27 28 Whether this really adds information relative to conventional radiographs has not been clarified to date.

The new ASAS classification criteria for patients with axial spondyloarthritis (SpA). To be eligible for these criteria, patients have to be younger than 45 years and have to have had chronic back pain for ≥3 months (from Rudwaleit et al25). CRP, C-reactive protein; IBP, inflammatory back pain; NSAIDs, non-steroidal anti-inflammatory drugs.

Definition of a ‘positive’ MRI for active sacroiliitis for classification of patients to axial spondyloarthritis (SpA) (from Rudwaleit et al26).
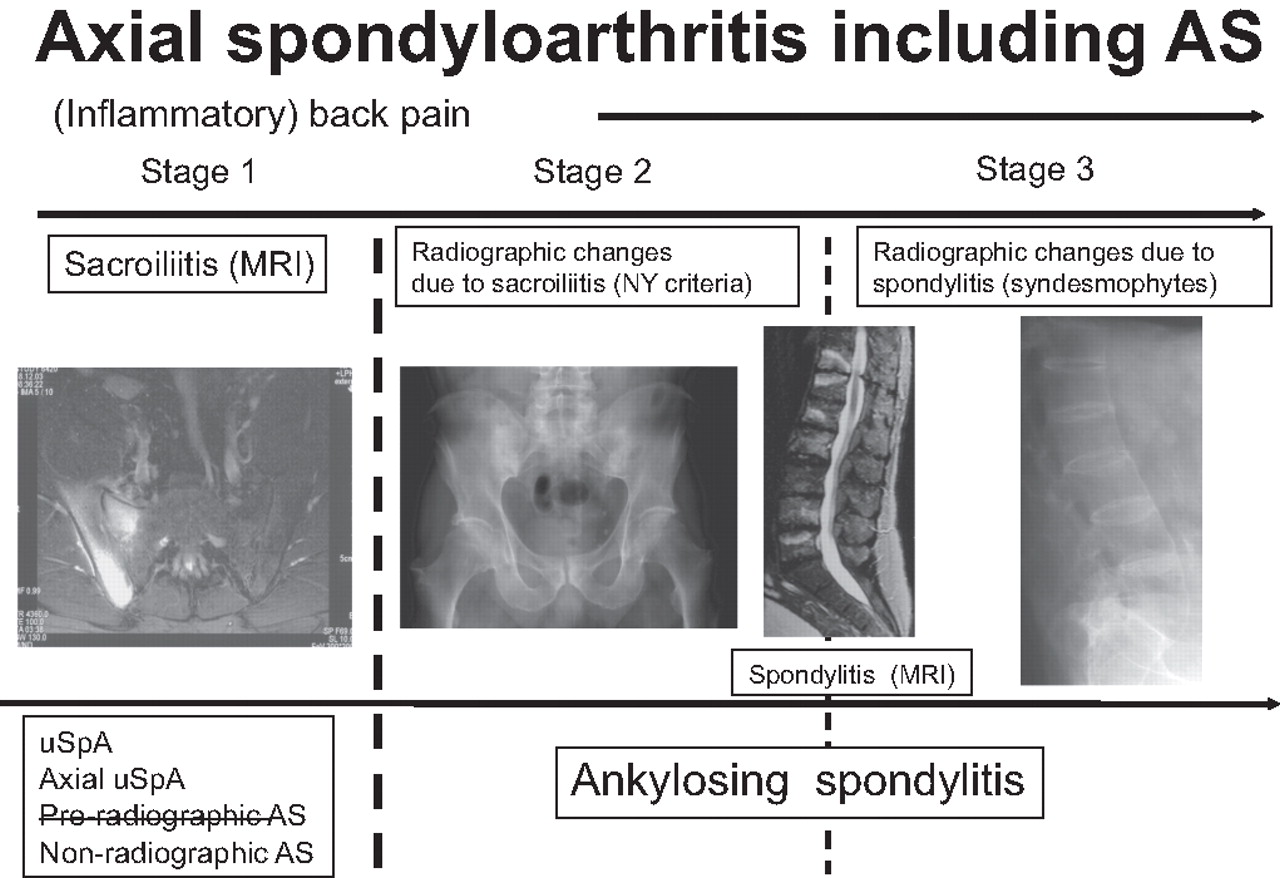
A proposal for a new concept of staging was made recently by Rudwaleit, Braun and Sieper at the ASAS Annual Meeting in Berlin 2010 (modified, figure 5). There was no general agreement on this.
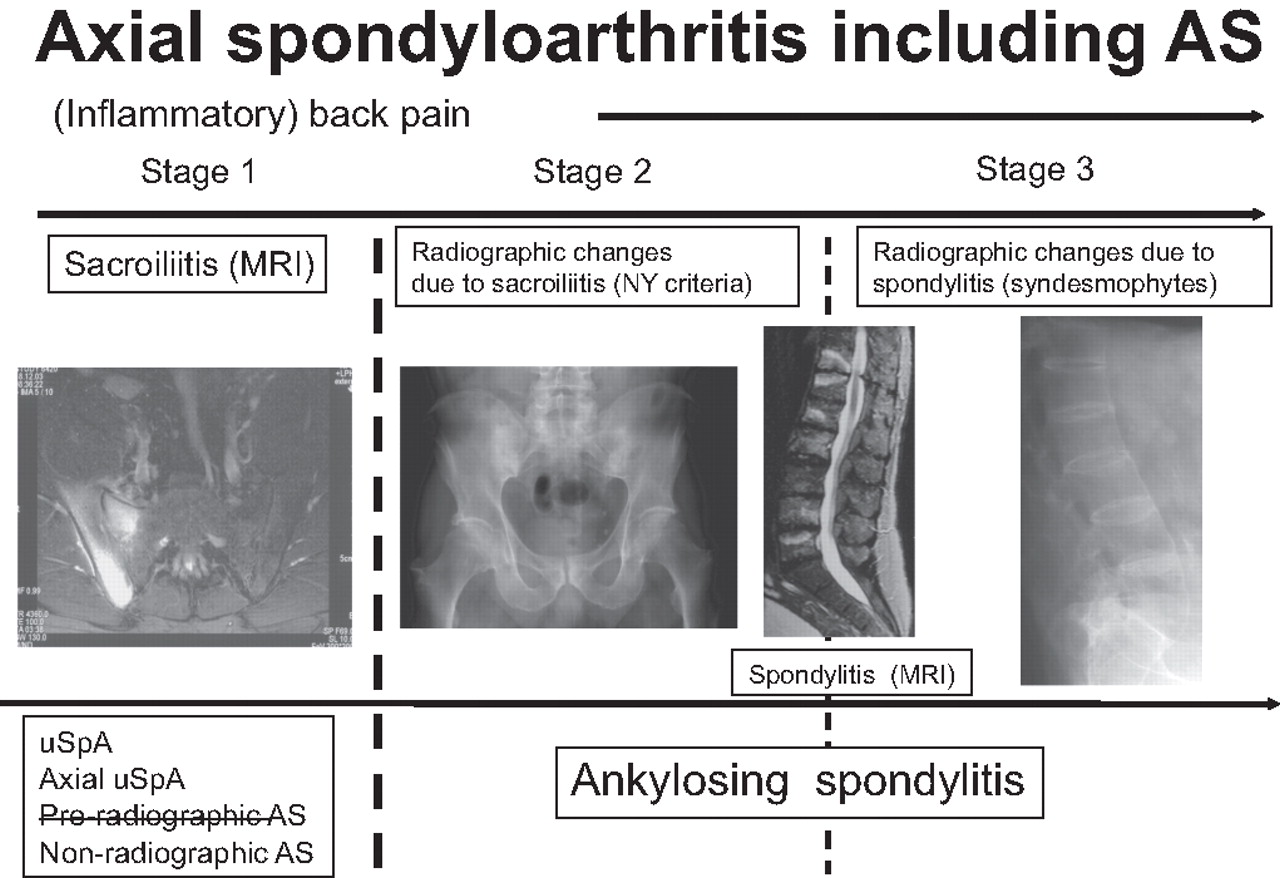
A proposal for a novel concept of staging of patients with axial spondyloarthritis (SpA) including ankylosing spondylitis (AS). uSpA, undifferentiated SpA.
Since there is some evidence that spondylitis may also occur before or without sacroiliitis a definition of a ‘positive MRI’ for spinal inflammation is also needed, and it will be essential for future scientific communication to agree internationally on definitions of the different MRI findings of both inflammatory and structural changes in axial SpA including AS; this work is in progress.29 Recent data have suggested that the posterior structures of the spine are involved early in the disease process (figure 6).30
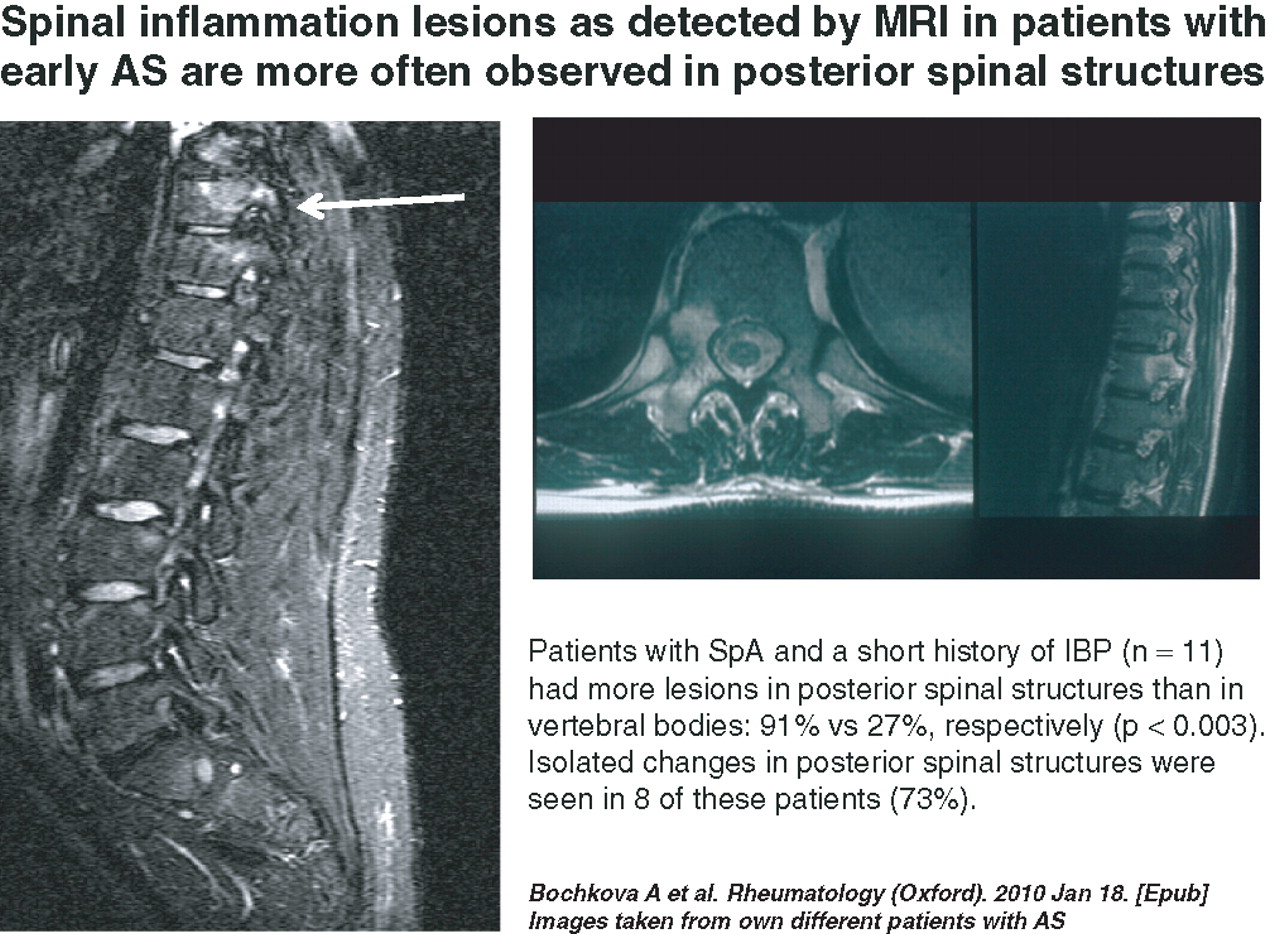
Involvement of the posterior structures of the spine are most frequently seen early in the disease process of spondyloarthritis (SpA). (Bochkova et al30 Images taken from our patients with ankylosing spondylitis (AS)). IBP. inflammatory back pain.
There is some evidence that T1-MRI sequences may also be useful for detecting structural spinal changes in patients with AS.10
Scoring conventional radiographs of the spine
New bone formation, such as syndesmophytes and ankylosis of the vertebral column are pathognomonic for AS. Conventional x-ray examinations of the spine are considered the gold standard for the quantitative assessment of chronic structural changes in patients with AS.6 31 The modified Stokes AS Spine Score (mSASSS,9), a validated scoring system for quantification of chronic spinal changes as detected by conventional radiographs,32 is currently considered the best method (figure 7).33 For an acceptable sensitivity to change a minimum follow-up time period of 2 years was shown to be required.34 Changes in mSASSS scores over time are mainly due to the growth of syndesmophytes and ankylosis, which are the most common radiographic features of progression in AS.4 The differentiation between AS-specific and non-specific changes—for example, by separating syndesmophytes from spondylophytes, was shown to have no major impact on mSASSS scores.4

The modified Stokes ankylosing spondylitis (AS) spinal score (mSASSS)—at present the most widely used scoring system for assessment of radiographic changes in AS (Creemers et al9).
According to a recent study, about 25% of the patients with AS have rapid radiographic progression (figure 8).5

The natural course of radiographic progression in patients with ankylosing spondylitis is variable. Although the mean radiographic progression of the cohort (n=146) was 1.3 mSASSS units per year (dotted line), a large proportion of patients showed faster progression rates than the mean (continuous lines) (from Baraliakos et al5). mSASSS, modified Stokes ankylosing spondylitis spinal score.
Treatment with anti-TNFα agents has recently been shown to significantly improve signs, symptoms and function of patients with AS.35,–,38 The inflammatory spinal lesions due to AS, as detected by MRI in short- and long-term follow-up examinations, were shown to regress to a large degree.12 13 39 In contrast, an inhibitory effect on radiographic progression has not been demonstrated until now40,–,44 (figure 9), but no prospective randomised placebo-controlled trials have been performed, only historical cohort data are available for comparison.40 45 46

Radiographic progression in the three major studies with anti-tumour necrosis factor (TNF) treatment in ankylosing spondylitis (AS). As compared with the historical OASIS cohort, an inhibitory effect on radiographic progression has not been demonstrated until now (from van der Heijde et al42,–,44). mSASSS, modified Stokes ankylosing spondylitis spinal score.
The comparison of radiographic progression rates in AS between studies is difficult,4 since there are different orders of reading47—for example, reading in time order and the awareness of the reader about the time sequence of the images, differences in the experience of the readers and also in the number of patients included in the studies.32 45 46 47
Furthermore, there are some methodological problems, such as the inability to assess the thoracic spine by standard radiography,10 and the low sensitivity of the mSASSS,4 which relates to the relatively low degree of damage (mean) that is usually seen in AS studies with less than one new syndesmophyte developing in the spine within 2 years.5 A recently proposed new scoring system, the Radiographic Ankylosing Spondylitis Spinal Score (RASSS), seems to have an increased sensitivity to change because the lower part of the thoracic spine is included, and only osteoproliferative lesions are scored.8 However, more data are needed to establish this new method.
Scoring MRI of the spine
Since the publication of the first scoring system, the AS spinal MRI (ASspiMRI-a, figure 10) 6 13 two other methods have been proposed for scoring spinal inflammation in AS, one is a modification of the original system first used in Berlin,48 and the Spondyloarthropathies Research Consortium of Canada (SPARCC) scoring system.49 All these have proved reliable and sensitive to change, based on a multiple-reader MRI scoring exercise,50 thereby passing the Outcome Measures in Rheumatologic Clinical Trials (OMERACT) filter51 of showing discrimination/sensitivity to change, truth and feasibility. No prioritisation of one of the scoring systems was proposed.
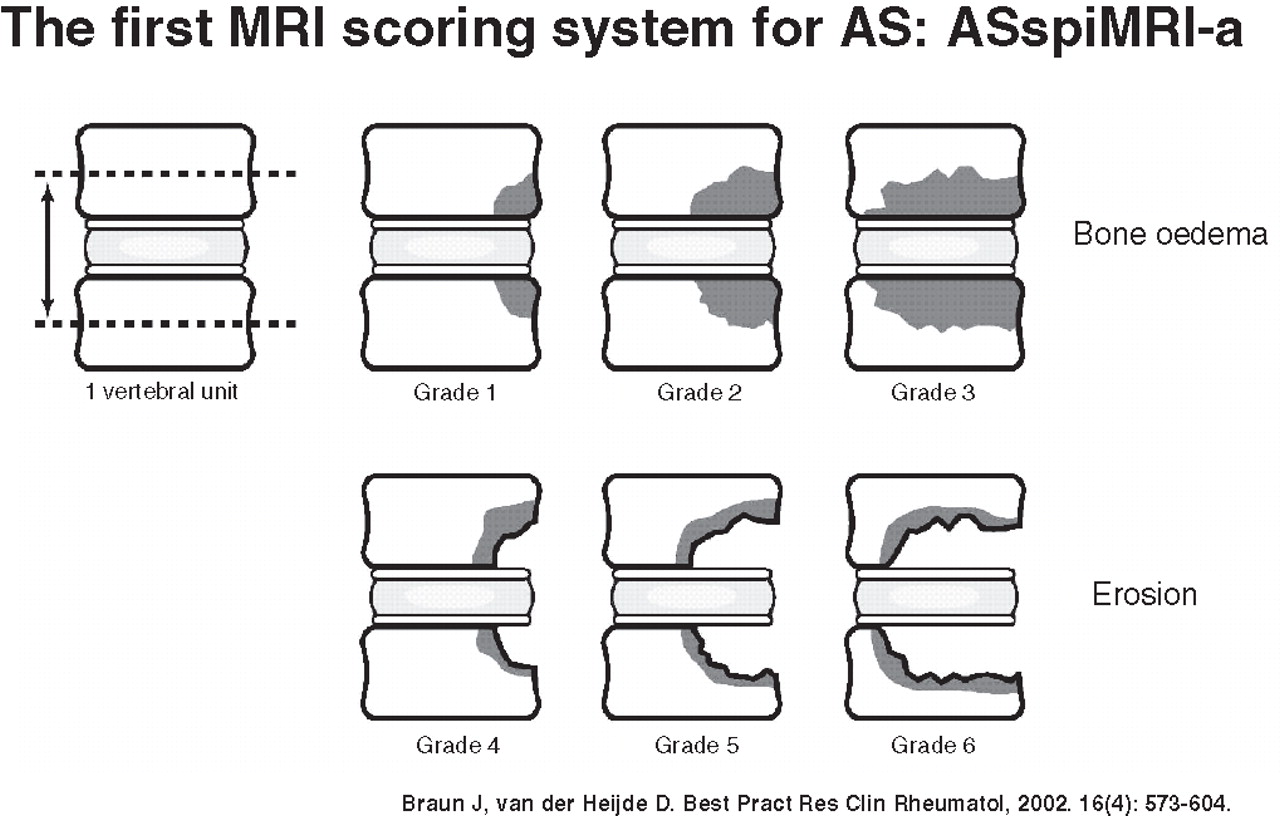
The ASspiMRI-a—the first MRI scoring system for assessment of spinal inflammatory changes in patients with ankylosing spondylitis using MRI (from Braun and van der Heijde6).
Similarly, there was no preference for any of the different MRI techniques used in the studies so far, since both MRI sequences (T1-post-Gd and STIR) can depict inflammatory spinal lesions.52 There are advantages and disadvantages for both techniques but the STIR sequence should be used for screening purposes since it is faster, less invasive (no contrast agent) and cheaper.52
However, as recently explained,50 the scoring systems have different contents. The Berlin score is based on the ASspiMRI-a and the assessment of spinal inflammation is identical in both systems. The additional and special feature of the ASspiMRI-a is the inclusion of active erosions: inflammation without erosions is graded according to the extent of inflammation by grades 1–3, and active erosions (surrounded by inflammation) are quantified by scores 4–6. This part of the ASspiMRI scoring system had been initially developed in order not to miss such osteodestructive changes, which were thought to be a direct consequence of inflammation. However, osteodestructive changes have always played a minor role in AS, since osteoproliferative changes are known to be much more common.10 With both systems, inactive erosions are not scored—only based on the absence of inflammation (score 0). The major advantage of the systems is that, in contrast to the Canadian system, the whole spine is scored53—this allows for direct comparisons with x-ray outcome studies.
After 2 years of anti-TNF therapy, 20–30% of patients with AS continue to have residual spinal inflammation,54 which raises questions about the efficacy of TNF blockers in these patients. Limited MRI data are available on the course of spinal inflammation in anti-TNF treated patients and it is not known whether any change in treatment, including an increase of the dosage, might resolve this problem. It is also unknown whether the persistence of spinal inflammation is linked to syndesmophyte formation. There is a clear need for clarification of these important issues by appropriate studies.
The effect of anti-TNF therapy on the development of fatty lesions (figure 11) in the anterior or posterior edges of vertebral bodies11 is unclear as yet. Preliminary evidence shows that the frequency of such changes may increase after anti-TNF therapy.54a

Example of a possible relationship between fatty degenerated changes seen on MRI and formation of a new syndesmophyte in a patient with ankylosing spondylitis (AS) (Bennett et al11, own images of a patient with AS, not from that paper).
Link between inflammation and new bone formation in AS
The link between inflammation and new bone formation in AS is of major interest ever since one study showed a possible inhibitory influence of non-steroidal anti-inflammatory drugs (NSAIDs) on radiographic progression55—in contrast to TNF blockers. Reasons for the possible lack of an influence of this treatment on syndesmophyte formation have been discussed in detail recently,56 including suggestions that (1) inflammation and new bone formation are, at least in part, uncoupled in AS, and/or (2) anti-TNF therapy by inhibiting osteoclast and promoting osteoblast activity even triggers ankylosing processes by interfering with the Wnt and/or the RANKL pathway.57,–,59 However, there is no evidence that patients receiving anti-TNF treatment have increased bone growth, although bone mineral density in the spine does increase in a relatively short period of time in anti-TNF treated patients.60 Treatment with NSAIDs that inhibit COX-261 may affect bone healing, prevent heterotopic ossification62 and even decelerate pathological bone growth in AS.55
The situation is different in rheumatoid arthritis and psoriatic arthritis. They are rheumatic diseases in which structural damage is regarded as an important outcome measure and in which all anti-TNF agents have been shown to inhibit radiographic progression, erosions and joint space narrowing63 64—structural changes which have an important impact on function over time. The position in AS is different since new bone formation, not bone destruction, is one of the two main factors that influence the functional outcome of patients with AS.4
Although it is conceivable that any ongoing new bone formation may not be stopped by blocking TNF, it seems still possible that new bone formation in patients with AS is prevented if inflammation is suppressed early enough before erosive structural damage has occurred.65
In studies that have directly linked spinal inflammation at baseline to syndesmophyte formation after 2 years66 67 there was evidence for a link (figure 12) but also for some uncoupling of new bone formation in AS. On the one hand, it turned out to be more likely that spinal inflammation resulted in syndesmophyte formation after 2 years, but, on the other hand, in the majority of the cases, syndesmophytes were not preceeded by spinal inflammation. Thus, it seems likely that intermediate changes of the structure of vertebral bodies such as sclerosis and fatty degeneration may be accompanied by functionally different reactions of the bone tissue including a diverse response to treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Formation of a new syndesmophytes 2 years after baseline captured by conventional x-rays and the relationship between previous inflammation in the same vertebral edges, captured by MRI (from Baraliakos et al66). AS, ankylosing spondylitis; TNF, tumour necrosis factor.
In addition to the discussions related to imaging, it should be emphasised that the rate of osteoporotic fractures in the spine of patients with AS is increased several fold.68 Thus a spinal fracture is an important differential diagnosis for patients with AS.
Conclusions
Based on the presented data an important question has recently been asked—what should be considered as the most important outcome parameter in AS?69 Next to structural damage, the outcome parameters of interest are (1) disease activity as best reflected by inflammatory spinal pain, morning stiffness and active inflammation in the SI joints and/or spine as shown by MRI; (2) function as assessed by questions related to activity such as walking, standing, reaching and participation such as toileting, performing jobs around the house, spinal mobility and (3) quality of life. Of course, these are inter-related, and, for example, function is determined by both disease activity and structural damage,70 71 with disease activity being more important early and structural damage later in the course of the disease. It will be interesting to determine at what point the relative impact of either factor will predominate. Clearly, in the first years after the initiation of anti-TNF therapy the suppression of disease activity seems much more important than new bone formation. The suppression of inflammation at an early point in the disease course is the most promising strategy for preventing new bone formation.
References
Footnotes
-
Competing interests None
-
Provenance and peer review Not commissioned; externally peer reviewed.