
Abstract
Allopurinol is the drug most widely used to lower the blood concentrations of urate and, therefore, to decrease the number of repeated attacks of gout. Allopurinol is rapidly and extensively metabolised to oxypurinol (oxipurinol), and the hypouricaemic efficacy of allopurinol is due very largely to this metabolite.
The pharmacokinetic parameters of allopurinol after oral dosage include oral bioavailability of 79 ± 20% (mean ± SD), an elimination half-life (t1/2) of 1.2 ± 0.3 hours, apparent oral clearance (CL/F) of 15.8 ± 5.2 mL/min/kg and an apparent volume of distribution after oral administration (Vd/F) of 1.31 ± 0.41 L/kg. Assuming that 90mg of oxypurinol is formed from every 100mg of allopurinol, the pharmacokinetic parameters of oxypurinol in subjects with normal renal function are a t1/2 of 23.3 ± 6.0 hours, CL/F of 0.31 ± 0.07 mL/min/kg, Vd/F of 0.59 ± 0.16 L/kg, and renal clearance (CLR) relative to creatinine clearance of 0.19 ±0.06. Oxypurinol is cleared almost entirely by urinary excretion and, for many years, it has been recommended that the dosage of allopurinol should be reduced in renal impairment. A reduced initial target dosage in renal impairment is still reasonable, but recent data on the toxicity of allopurinol indicate that the dosage may be increased above the present guidelines if the reduction in plasma urate concentrations is inadequate. Measurement of plasma concentrations of oxypurinol in selected patients, particularly those with renal impairment, may help to decrease the risk of toxicity and improve the hypouricaemic response. Monitoring of plasma concentrations of oxypurinol should also help to identify patients with poor adherence. Uricosuric drugs, such as probenecid, have potentially opposing effects on the hypouricaemic efficacy of allopurinol. Their uricosuric effect lowers the plasma concentrations of urate; however, they increase the CLR of oxypurinol, thus potentially decreasing the influence of allopurinol. The net effect is an increased degree of hypouricaemia, but the interaction is probably limited to patients with normal renal function or only moderate impairment.












Similar content being viewed by others

References
Rundles RW. The development of allopurinol. Arch Intern Med 1982; 145: 89–94
Day R, Birkett DJ, Hicks M, et al. Allopurinol: new uses. Drugs 1994; 48: 339–44
van Waeg G, Loof L, Groth T, et al. Allopurinol kinetics in humans as a means to assess liver function: evaluation of an allopurinol loading test. Scand J Clin Lab Med 1988; 48: 45–57
Murrell GAC, Rapeport WG. Clinical pharmacokinetics of allopurinol. Clin Pharmacokinet 1986; 11: 343–53
Fujimoto Y, Sakuma S, Tagami T, et al. N-ethylmaleimide inhibits xanthine oxidase activity with no detectable change in xanthine dehydrogenase activity in rabbit liver. Life Sci 2000; 68: 517–24
Massey V, Komai H, Palmer G, et al. On the mechanism of inactivation of xanthine oxidase by allopurinol and other pyrazolo[3,4-d]pyrimidines. J Biol Chem 1970; 245: 2837–44
Seegmiller JE. The acute attack of gouty arthritis. Arthritis Rheum 1965; 8: 714–25
Campion EW, Glynn RJ, DeLabry LO. Asymptomatic hyperuricemia: risks and consequences in the normative aging study. Am J Med 1987; 82: 421–6
Drayton CJ. Comprehensive medicinal chemistry. Vol. 6. Oxford: Pergamon Press, 1990
Breithaupt H, Tittel M. Kinetics of allopurinol after single intravenous and oral doses. Eur J Clin Pharmacol 1982; 22: 77–84
Colin JN, Farinotti R, Fredj G, et al. Kinetics of allopurinol and oxipurinol after chronic oral administration: interaction with benzbromarone. Eur J Clin Pharmacol 1986; 31: 53–8
Berlinger WG, Park GD, Spector R. The effect of dietary protein on the clearance of allopurinol and oxypurinol. New Engl J Med 1985; 313: 771–6
de Vries JX, Voss A, Ittensohn A, et al. Interaction of allopurinol and hydrochlorothiazide during prolonged oral administration of both drugs in normal subjects: II. Kinetics of allopurinol, oxipurinol, and hydrochlorothiazide. Clin Invest 1994; 72: 1076–81
Walter-Sack I, de Vries JX, Kreiner C, et al. Bioequivalence of allopurinol preparations: to be assessed by the parent drug or the active metabolite? Clin Invest 1993; 71: 240–6
Simmonds HA. Urinary excretion of purines, pyrimidines and pyrazolopyrimidines in patients treated with allopurinol or oxipurinol. Clin Chim Acta 1969; 23: 353–64
Reiter S, Loffler W, Grobner W, et al. Urinary oxypurinol-1-riboside and allopurinol-induced oroticaciduria. Adv Exp Med Biol 1986; 195 Pt A: 453–60
Robson RA, Begg EJ, Saunders DA. Allopurinol autoinhibition. Clin Exp Pharmacol Physiol 1993; Suppl. 1: 62
Nelson DJ, Elion GB. Metabolic studies of high doses of allopurinol in humans. Adv Exp Med Biol 1984; 165A: 167–70
Graham S, Day RO, Wong H, et al. Pharmacodynamics of oxypurinol after administration of allopurinol to healthy subjects. Br J Clin Pharmacol 1996; 41: 299–304
Shibutani Y, Ueo T, Yamamoto T, et al. A case of classical xanthinuria (type 1) with diabetes mellitus and Hashimoto’s thyroiditis. Clin Chim Acta 1999; 285: 183–9
Reiter S, Simmonds HA, Zöllner N, et al. Demonstration of a combined deficiency of xanthine oxidase and aldehyde oxidase in xanthinuric patients not forming oxipurinol. Clin Chim Acta 1990; 187: 221–34
Auscher C, Pasquier C, Mercier N, et al. Urinary excretion of a 6 hydroxylated metabolite and oxypurines in a xanthinuric man given allopurinol or thiopurinol. Adv Exp Med Biol 1973; 41: 663–7
Spector T. Inhibition of urate production by allopurinol. Biochem Pharmacol 1977; 26: 355–8
Johns DG. Human liver aldehyde oxidase: differential inhibition of oxidation of charged and uncharged substrates. J Clin Invest 1967; 46: 1492–505
Choi HK, Mount DB, Reginato AM. Pathogenesis of gout. Ann Int Med 2005; 143: 499–516
Walter-Sack I, de Vries JX, Ernst B, et al. Uric acid lowering effect of oxipurinol sodium in hyperuricemic patients - therapeutic equivalence to allopurinol. J Rheumatol 1996; 23: 498–501
Bührens K, Berndt P, Hilgenstock CM, et al. Bioequivalence of two allopurinol preparations. Arzneim-Forsch 1991; 41: 250–3
Schuster O, Haertel M, Hugemann B, et al. Studies on the clinical pharmacokinetics of allopurinol. Arzneim-Forsch 1985; 35: 760–5
Metzner JE, Buchberger D, Läuter J, et al. Investigation into the bioequivalence of a new allopurinol tablet formulation compared with a standard preparation. Arzneim-Forsch 1997; 47: 1236–41
Fenner H, Schiemann O, Gikalov I. The clinical pharmacokinetics of allopurinol. 2. Allopurinol/oxypurinol pharmacokinetics following allopurinol in single doses and multiple application. Arzneim-Forsch 1985; 35: 1093–6
Purves RD. Anomalous parameter estimates in the one-compartment model with first-order absorption. J Pharm Pharmacol 1993; 45: 934–6
Turnheim K, Krivanek P, Oberbauer R. Pharmacokinetics and pharmacodynamics of allopurinol in elderly and young subjects. Br J Clin Pharmacol 1999; 48: 501–9
Sheiner LB, Benet LZ, Pagliaro LA. A standard approach to compiling clinical pharmacokinetic data. J Pharmacokinet Biopharm 1981; 9: 59–127
Saji M. A study of the serum oxypurinol concentration and renal function in patients administered allopurinol. Jap J Nephrol 1996; 38: 640–50
Appelbaum SJ, Mayersohn M, Dorr RT, et al. Allopurinol kinetics and bioavailability: intravenous, oral and rectal administration. Cancer Chemother Pharmacol 1982; 8: 93–8
Marcus M, Tse FL, Kleinberg SI. The bioavailability of two commercial preparations of allopurinol tablets. Int J Clin Pharmacol Ther Toxicol 1982; 20: 302–5
Guerra P, Frias J, Ruiz B, et al. Bioequivalence of allopurinol and its metabolite in two tablet formulations. J Clin Pharm Ther 2001; 26: 113–9
Hande K, Reed E, Chabner B. Allopurinol kinetics. Clin Pharmacol Ther 1978; 23: 598–605
Lartigue-Mattei C, Chabard JL, Ristori JM. Kinetics of allopurinol and its metabolite oxypurinol after oral administration of allopurinol alone or associated with benzbromarone in man: simultaneous assay of hypoxanthine and xanthine by gas chromatography-mass spectrometry. Fundam Clin Pharmacol 1991; 5: 621–33
Kitt TM, Park GD, Spector R, et al. Reduced renal clearance of oxypurinol during a 400 calorie protein-free diet. J Clin Pharmacol 1989; 29: 65–71
Elion GB, Yü T, Gutman AB, et al. Renal clearance of oxipurinol, the chief metabolite of allopurinol. Am J Med 1968; 45: 69–77
Hande KR, Noone RM, Stone WJ. Severe allopurinol toxicity: description and guidelines for prevention in patients with renal insufficiency. Am J Med 1984; 76: 47–56
Moriwaki Y, Yamamoto T, Tsutsumi Z, et al. Effects of angiotensin II infusion on renal excretion of purine bases and oxypurinol. Metabolism 2002; 51: 893–5
Yamamoto T, Moriwaki Y, Takahashi S, et al. Effects of pyrazinamide, probenecid, and benzbromarone on renal excretion of oxypurinol. Ann Rheum Dis 1991; 50: 631–3
Yamamoto T, Moriwaki Y, Takahashi S, et al. Effect of losartan potassium, an angiotensin antagonist, on renal excretion of oxypurinol and purine bases. J Rheumatol 2000; 27: 2232–6
Yamamoto T, Moriwaki Y, Takahashi S, et al. Effect of fenofibrate on plasma concentration and urinary excretion of purine bases and oxypurinol. J Rheumatol 2001; 28: 2294–7
Yamamoto T, Moriwaki Y, Takahashi S, et al. Effect of frusemide on renal excretion of oxypurinol and purine bases. Metabolism 2001; 50: 241–5
Yamamoto T, Moriwaki Y, Takahashi S, et al. Effect of norepinephrine on the urinary excretion of purine bases and oxypurinol. Metabolism 2001; 50: 1230–3
Emmerson BT, Gordon RB, Cross M, et al. Plasma oxipurinol concentrations during allopurinol therapy. Br J Rheumatol 1987; 26: 445–9
Peterson GM, Boyle RR, Francis, et al. Dosage prescribing and plasma oxipurinol levels in patients receiving allopurinol therapy. Eur J Clin Pharmacol 1990; 26: 419–21
Day RO, Miners JO, Birkett DJ, et al. Allopurinol dosage selection: relationships between dose and plasma oxypurinol and urate concentrations and urinary urate excretion. Br J Clin Pharmacol 1988; 26: 423–8
Ichida K, Hosoyamada M, Hisatome I, et al. Clinical and molecular analysis of patients with renal hypouricemia in Japan: influence of URAT1 gene on urinary urate excretion. J Am Soc Nephrol 2004; 15: 164–73
Iwanaga T, Kobayashi D, Hirayama M, et al. Involvement of uric acid transporter in increased renal clearance of the xanthine oxidase inhibitor oxypurinol induced by a uricosuric agent, benzbromarone. Drug Metab Disp 2005; 33: 1791–5
Williams KM, Stocker SL, McLachlan AJ, et al. Investigating pharmacokinetic and pharmacodynamic interaction between allopurinol and probenecid in healthy subjects [abstract]. Intern Med J 2006; 36: A39
Reinders MK, van Roon EN, Houtman PM, et al. Biochemical effectiveness of allopurinol and allopurinol-probenecid in previously benzbromarone-treated gout patients. Clin Rheumatol. Epub 2007 Feb 17
Yü T, Gutman AB. Effect of allopurinol (4-hydroxypyrazolo(3,4-d)pyrimidine) on serum and urinary uric acid in primary and secondary gout. Am J Med 1964; 37: 885–98
Garyfallos A, Magoula I, Tsapas G. Evaluation of the renal mechanisms for urate homeostasis in uremic patients by probenecid and pyrazinamide test. Nephron 1987; 46: 273–80
Ruffer C, Zorn G, Henkel E, et al. Influence of benzbromarone on the pharmacokinetics and pharmacodynamics of oxipurinol. Arzneim Forsch 1982; 32: 1149–52
Müller FO, Schall R, Groenewoud G, et al. The effect of benzbromarone on allopurinol/oxypurinol kinetics in patients with gout. Eur J Clin Pharmacol 1993; 44: 69–72
Mertz DP, Eichhorn R. Does benzbromarone in therapeutic doses raise renal excretion of oxipurinol? Klin Wochenschr 1984; 62: 1170–2
Walter-Sack I, de Vries JX, von Bubnoff A, et al. Biotransformation and uric acid lowering effect of benzbromarone in patients with liver cirrhosis - evidence for active benzbromarone metabolites? Eur J Med Res 1995; 1: 16–20
Takahashi S, Moriwaki Y, Yamamoto T, et al. Effects of combination treatment using anti-hyperuricaemic agents with fenofibrate and/or losartan on uric acid metabolism. Ann Rheum Dis 2003; 62: 572–5
Sica DA, Gehr TWB, Ghosh S. Clinical pharmacokinetics of losartan. Clin Pharmacokinet 2005; 44: 797–814
Feher MD, Hepburn AL, Hogarth MB, Ball SG, Kaye SA. Fenofibrate enhances urate reduction in men treated with allopurinol for hyperuricaemia and gout. Rheumatology 2003, 42, 321–5
Jones MR, Baker BA, Matthew P. The effect of colesevelam HCl on single dose fenofibrate kinetics. Clin Pharmacokinet 2004; 43: 943–50
Leary WP, Reyes AJ, Wynne RD, et al. Renal excretory actions of frusemide, of hydrochlorothiazide and of the vasodilator flosequinan in healthy subjects. J Int Med Res 1990; 18: 120–41
Yamamoto T, Moriwaki Y, Takahashi S. Effect of ethanol on metabolism of purine bases (hypoxanthine, xanthine, and uric acid). Clin Chim Acta 2005; 356: 35–57
Choi HK, Atkinson K, Karlson EW, et al. Alcohol intake and risk of incident gout in men: a prospective study. Lancet 2004; 363: 1277–81
Gibson T, Rodgers AV, Simmonds HA, et al. Beer drinking and its effect on uric acid. Br J Rheumatol 1984; 23: 203–9
Yamamoto T, Moriwaki Y, Takahashi S, et al. Ethanol as a xanthine dehydrogenase inhibitor. Metabolism 1995; 44: 779–85
Kaneko K, Fujimori S, Ishizuka I, et al. Effect of ethanol on the metabolism of the hyperuricemic agents allopurinol and benzbromarone. Clin Chim Acta 1990; 193: 181–6
Ralston SH, Capell HA, Sturrock RD. Alcohol and response to treatment of gout. BMJ 1988; 296: 1641–2
Bianchi R, Vitali C, Clerico A, et al. Uric acid metabolism in normal subjects and in gouty patients by chromatographic measurement of 14C-uric acid in plasma and urine. Metabolism 1979; 28: 1105–13
Berg H. Examination of the effectiveness and tolerance of long term urate lowering treatment. Z Gesamte Inn Med 1990; 45: 719–20
Kelley EE, Trostchansky A, Rubbo H, et al. Binding of xanthine oxidase to glycoaminoglycans limits inhibition by oxypurinol. J Biol Chem 2004; 279: 37231–4
Day RO, Miners J, Birkett DJ, et al. Relationship between plasma oxipurinol concentrations and xanthine oxidase activity in volunteers dosed with allopurinol. Br J Clin Pharmacol 1988; 26: 429–34
Birkett DJ, Miners J, Day RO. 1-Methylxanthine derived from theophylline as an in vivo biochemical probe of allopurinol effect. Br J Clin Pharmacol 1991; 32: 238–41
Birkett DJ, Miners JO, Valente L, et al. 1-methylxanthine derived from caffeine as a pharmacodynamic probe of oxypurinol effect. Br J Clin Pharmacol 1997; 43: 197–200
Fuchs P, Haefeli WE, Ledermann HR, et al. Xanthine oxidase inhibition by allopurinol affects the reliability of urinary caffeine metabolic ratios as markers for N-acetyltransferase 2 and CYP1A2 activities. Eur J Clin Pharmacol 1999; 54: 869–76
Hamanaka H, Mizutani H, Nouchi N, et al. Allopurinol hyper-sensitivity syndrome: hypersensitivity to oxypurinol but not allopurinol. Clin Exp Dermatol 1998; 23: 32–4
Braden GL, Warzynski MJ, Golightly M, et al. Cell-mediated immunity in allopurinol-induced hypersensitivity. Clin Immunol Immunopathol 1994; 70: 145–51
Emmerson BT, Hazelton RA, Frazer IH. Some adverse reactions to allopurinol may be mediated by lymphocyte reactivity to oxypurinol. Arthritis Rheum 1988; 31: 436–40
Pichler WJ, Tilch J. The lymphocyte transformation test in the diagnosis of drug hypersensitivity. Allergy 2004; 59: 809–20
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron 1976; 16: 31–41
Hung S, Chung WH, Liou LB, et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc Nat Acad Sci 2005; 102: 4134–9
Vazquez-Mellado J, Morales EM, Pacheco-Tena C, et al. Relation between adverse events associated with allopurinol and renal function in patients with gout. Ann Rheum Dis 2001; 60: 981–3
Becker MA, Schumacher HR, Wortmann RL, et al. Febuxostat compared with allopurinol in patients with hyperuricemia and gout. New Engl J Med 2005; 353: 2450–61
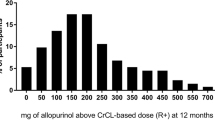
Dalbeth N, Kumar S, Stamp L, et al. Dose adjustment of allopurinol according to creatinine clearance does not provide adequate control of hyperuricaemia in patients with gout. J Rheumatol 2006; 33: 1646–50
Dalbeth N, Stamp L. Allopurinol dosing in renal impairment: walking the tightrope between adequate urate lowering and adverse events. Semin Dial. Epub 2007 Apr 17
Zhang W, Doherty M, Bardin T, et al. EULAR evidence based recommendations for gout. Part II: management. Report of a task force of the EULAR Standing Committee For International Clinical Studies Including Therapeutics (ESCISIT). Ann Rheum Dis 2006; 65: 1312–24
Elion GB, Benezra FM, Beardmore TD, et al. Studies with allopurinol in patients with impaired renal function. Adv Exp Med Biol 1980; 122A: 263–7
Sarawate CA, Brewer KK, Yang W, et al. Gout medication treatment patterns and adherence to standards of care from a managed care perspective. Mayo Clin Proc 2006; 81: 925–34
Thompson GR, Duff IF, Robinson WD, et al. Long term uricosuric therapy in gout. Arthritis Rheum 1962; 5: 384–96
Emmerson BT. The use of the xanthine oxidase inhibitor, allopurinol, in the control of hyperuricaemia, gout and uric acid calculi. Aust Ann Med 1967; 16: 205–14
Acknowledgements
The authors gratefully acknowledge the help of Dr Pal Pacher and Associate Prof. J.B. Ziegler for help with references on allopurinol and Prof. K. Turnheim for the supply of his experimental data. No sources of funding were used to assist in the preparation of this review. The authors have no conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Day, R.O., Graham, G.G., Hicks, M. et al. Clinical Pharmacokinetics and Pharmacodynamics of Allopurinol and Oxypurinol. Clin Pharmacokinet 46, 623–644 (2007). https://doi.org/10.2165/00003088-200746080-00001
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003088-200746080-00001