

Abstract
Objective. To characterize patients with rheumatoid arthritis (RA) by number of poor prognostic factors (PPF: functional limitation, extraarticular disease, seropositivity, erosions) and evaluate treatment acceleration, clinical outcomes, and work status over 12 months by number of PPF.
Methods. Using the Corrona RA registry (January 2005–December 2015), biologic-naive patients with diagnosed RA having 12-month (± 3 mos) followup were identified and categorized by PPF (0–1, 2, ≥ 3). Changes in medication, Clinical Disease Activity Index (CDAI), and work status (baseline–12 mos) were evaluated using linear and logistic regression models.
Results. There were 3458 patients who met the selection criteria: 1489 (43.1%), 1214 (35.1%), and 755 (21.8%) had 0–1, 2, or ≥ 3 PPF, respectively. At baseline, patients with ≥ 3 PPF were older, and had longer RA duration and higher CDAI versus those with 0–1 PPF. In 0–1, 2, and ≥ 3 PPF groups, respectively, 20.9%, 23.2%, and 26.5% of patients received ≥ 1 biologic (p = 0.011). Biologic/targeted synthetic disease-modifying antirheumatic drug (tsDMARD) use was similar in patients with/without PPF (p = 0.57). After adjusting for baseline CDAI, mean (standard error) change in CDAI was −4.95 (0.24), −4.53 (0.27), and −2.52 (0.34) for 0–1, 2, and ≥ 3 PPF groups, respectively. More patients were working at baseline but not at 12-month followup in 2 (13.9%) and ≥ 3 (12.5%) versus 0–1 (7.3%) PPF group.
Conclusion. Despite high disease activity and worse clinical outcomes, number of PPF did not significantly predict biologic/tsDMARD use. This may warrant reconsideration of the importance of PPF in treat-to-target approaches.
The rate of disease progression in patients with rheumatoid arthritis (RA) is dependent on several factors and varies among patients1,2. Factors associated with a poor prognosis in patients with RA predict a more rapid and aggressive disease course. The presence of many poor prognostic factors (PPF) in patients with recent-onset RA has been associated with increased risk of disease progression in both clinical trials and observational studies3,4. However, a single, universal list of PPF does not exist in RA, and there are important distinctions between how these factors are described by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR). Further, even within ACR and EULAR treatment recommendations, the definitions and types of PPF and their relative importance have continued to evolve. The EULAR guidelines (2010, 2013, and 2016) recommend more aggressive management for patients with RA if the treatment target is not achieved with the first conventional synthetic disease-modifying antirheumatic drug (csDMARD) strategy and PPF are present2,5,6. The ACR 2008 guidelines and the 2012 update also took the presence of PPF into consideration, along with disease duration, disease activity, and current medication regimen, when determining the approach to management7,8. However, current (2015) ACR guidelines1 focus on patient disease activity and a treat-to-target method for all patients, regardless of prognosis. Continued research is required to understand whether these modifications in the treatment strategy have improved patient outcomes.
For our study, which was undertaken in US clinical practice from 2005 to 2015, the ACR 2008 guidelines (including the 2012 update) were the primary treatment recommendations in use, because the study ended before the guidelines were updated in 2015. PPF were defined by ACR in 2008 as functional limitation [evaluated by the Health Assessment Questionnaire–Disability Index (HAQ-DI) or similar validated tools], extraarticular disease [Sjögren syndrome (SS), RA lung disease, and/or nodules), seropositivity [rheumatoid factor (RF) or anticyclic citrullinated peptide antibodies], and the presence of radiographic bone erosions8. In contrast, EULAR defined PPF in 2016 as moderate (after csDMARD therapy) to high disease activity according to composite measures; high acute-phase reactant levels; high swollen joint counts; presence of RF and/or anticitrullinated protein antibody, especially at high levels; any combination of the preceding prognostic factors; presence of early erosions; and failure of 2 or more csDMARD6. The 2008 ACR-defined PPF of seropositivity and erosions are also included in the EULAR 2016 definitions, whereas extraarticular disease and functional limitation are not. This further highlights the need for a universal definition for PPF in RA.
Limited real-world data, based on studies with small patient numbers, exist on the effect of PPF on treatment decisions and outcomes in patients with newly diagnosed RA9,10. Further, to our knowledge, there are no studies evaluating the proportion of patients with PPF among patients with longer-standing RA.
We had 2 objectives: to characterize a cohort of patients with RA in a typical practice setting based on the number of PPF (defined by the presence of functional limitation, extraarticular disease, seropositivity, and erosive changes), and to evaluate treatment acceleration, clinical outcomes, and work status by number of PPF over 12 months in this cohort.
MATERIALS AND METHODS
Patient population
The Corrona RA registry is an ongoing, independent, prospective, national, observational cohort. Patients are recruited from 169 private and academic practice sites across 40 states in the US, with 656 participating rheumatologists. As of June 30, 2016, the Corrona database included information on about 43,009 patients with RA. Data on 326,613 patient visits and about 145,527 patient-years of followup observation time have been collected. The average length of patient followup is 4.13 years (median 3.33 yrs).
The registry was set up in accordance with the Declaration of Helsinki. All participating investigators were required to obtain full board approval for conducting noninterventional research involving human subjects with a limited dataset. Sponsor approval and continuing review was obtained through a central Institutional Review Board (IRB; New England Independent Review Board, NEIRB No. 120160610). For academic investigative sites that did not receive a waiver to use the central IRB, full board approval was obtained from the respective governing IRB and documentation of approval was submitted to Corrona LLC prior to initiating any study procedures. All registry patients were required to provide written informed consent and authorization prior to participating.
Study population
This analysis included patients diagnosed with RA (excluding early undifferentiated arthritis) by their rheumatologist who were 18 years of age or older and naive to therapy with biologics and/or targeted synthetic DMARD (tsDMARD; tofacitinib was the only approved tsDMARD at the time of this analysis) at the time of enrollment in the Corrona RA registry between January 1, 2005, and December 1, 2015. Eligible patients had a followup visit at 12 months (± 3 mos) and Clinical Disease Activity Index (CDAI) measured at baseline (i.e., enrollment) and at the 12-month followup. Work status was also assessed at both baseline and the 12-month followup. The index date was the date of enrollment.
Measures and data collection
Patients were characterized at baseline for RA prognosis based on the 2008 ACR treatment recommendations7, including functional limitation (based on modified HAQ-DI > 0.5)11,12, extraarticular disease (SS, RA lung disease, and/or nodules), seropositivity (RF and/or anticyclic citrullinated peptide antibodies), and erosions (as per radiograph at enrollment). If patients met none of the 4 criteria, they would be classified as having 0 PPF; similarly, if they had met 1, 2, 3, or 4 criteria they would be classified as having 1, 2, 3, or 4 PPF. Because of sample size limitations, patients were then categorized into groups having 0–1, 2, or ≥ 3 PPF; each of the 4 categories contributed 1 point. Patients with missing information for any factor were excluded from the analysis.
Study outcomes
Baseline characteristics were evaluated and stratified by PPF. To ensure an adequate sample size for statistical analysis, treatment changes over a duration of 12 months (± 3 mos) were investigated. The primary outcome was the process measure of initiating a biologic or tsDMARD by PPF group, as well as the process measure of any treatment acceleration (addition of, or switching to, a csDMARD, and/or initiation of a different biologic or tsDMARD) of medication used at enrollment. Use of biologic/tsDMARD treatment was assessed from baseline to the 12-month followup visit (± 3 mos). Specifically, patients were grouped into “no biologic use” or “use of 1 or more biologic” over the 12-month period (0 or ≥ 1 categories). Secondary outcomes included change in disease activity at 12 months, assessed by the change from baseline in CDAI in all patients, and achievement of low disease activity (LDA)/remission (CDAI ≤ 10) in patients with moderate or high disease activity at baseline. Other secondary outcomes included a dichotomous variable for work status, constructed with “yes” defined as paid full-time or part-time work, and “no” including those patients who were not working or who worked at home or were students, disabled, or retired. Changes in work status from baseline to the 12-month followup were evaluated.
Statistical analysis
Baseline differences between PPF groups in treatment acceleration, disease activity, and work status were evaluated through chi-square tests for categorical variables and Wilcoxon rank-sum tests for continuous variables because of the skewed nature of the data. Logistic regression models (unadjusted and adjusted for age, sex, duration of RA, and baseline CDAI) evaluated the association of PPF with receipt of biologics/tsDMARD as well as any treatment acceleration. Linear regression models (unadjusted and adjusted for baseline CDAI) evaluated the effect of PPF on change in CDAI. Logistic regression models (unadjusted and adjusted for baseline CDAI) evaluated the effect of PPF category on LDA/remission in patients with moderate or high disease activity at baseline.
The relationship between PPF groups and work status was investigated at baseline and the 12-month followup using chi-square tests. A frequency-matching approach (coarsened exact matching) was used to match patients across PPF categories according to age group (18–44, 45–54, 55–64, 65–74, ≥ 75 yrs), because the relationship between PPF category and work status could be driven by age difference (retirees are generally older). The sample size for each age category was the size of the smallest PPF category. To assess whether the relationship between work status at baseline and followup differed according to number of PPF, the Cochran–Mantel–Haenszel test was performed for all patients.
RESULTS
Patient disposition and baseline characteristics
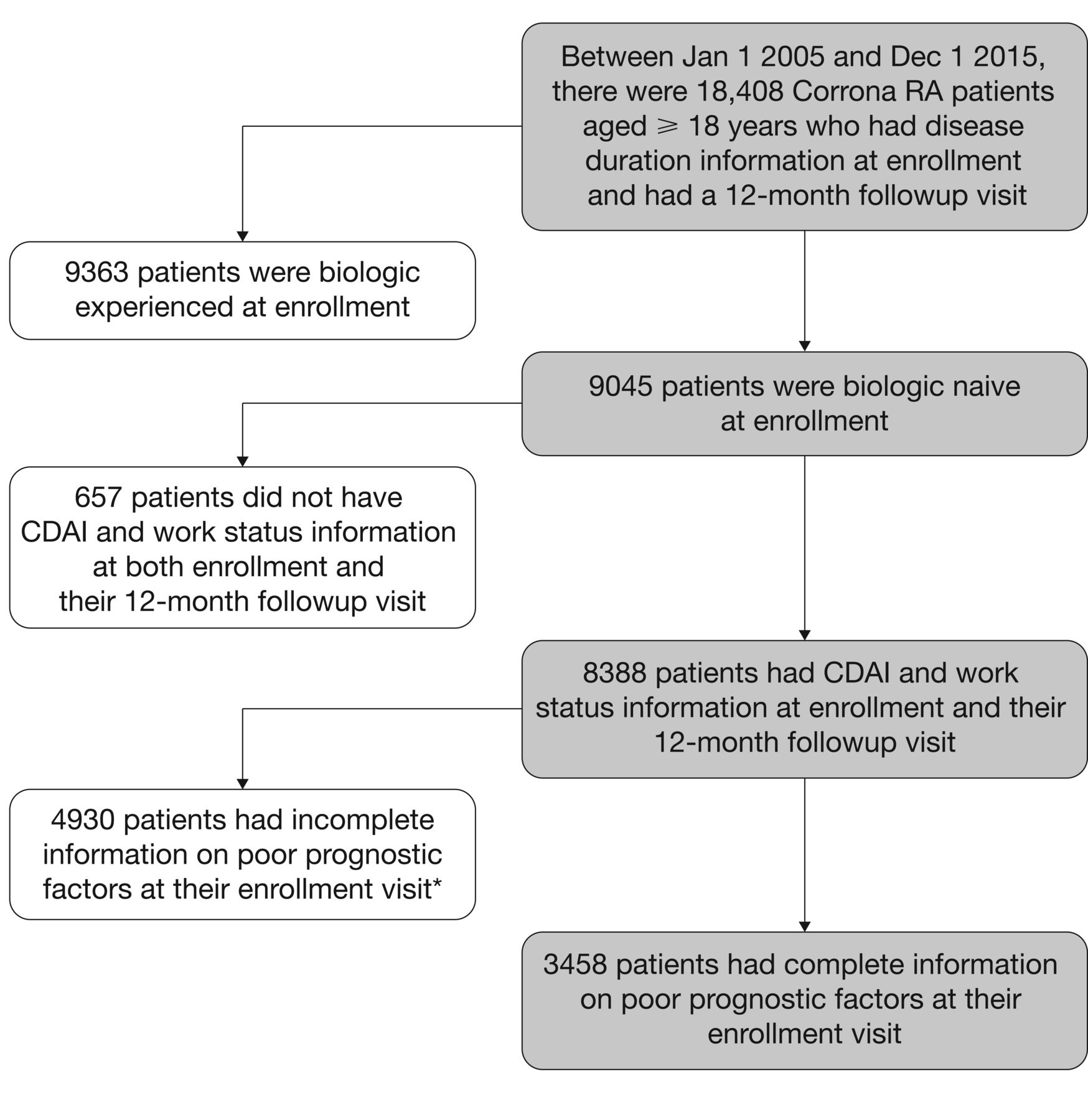
Of the 18,408 patients aged 18 years or older who were enrolled in the Corrona RA registry from January 1, 2005, through December 1, 2015, and had disease duration information at enrollment and a 12-month followup visit, 3458 met the selection criteria (Figure 1). Of these, 1489 (43.1%), 1214 (35.1%), and 755 (21.8%) were categorized into prognosis groups of 0–1, 2, or ≥ 3 PPF, respectively. Baseline demographic data and clinical characteristics indicated that patients with a greater number of PPF were older, had a longer duration of RA, and had higher CDAI compared with those with fewer PPF (Table 1). Of note, an additional 4930 patients had incomplete information on PPF at enrollment (3588 patients had no seropositive status information and 1342 patients had incomplete other PPF at enrollment). These 4930 patients were demographically similar to the group of 3458 patients with PPF; 74% of the 3458 with PPF were female compared with 75% of those without prognostic information. Mean age [SD; 59.0 (13.2) vs 60.1 (13.5) yrs] and baseline disease activity as measured by the CDAI [9.0 (16.9) vs 8.6 (14.8)] were also similar between these 2 groups. Median (interquartile range) disease duration was slightly shorter in the group with PPF: 2 (7) versus 3 (9) years.

Criteria for study inclusion. Of note, 4930 patients had incomplete information on PPF at enrollment. Of these, 3588 patients had no seropositive status information and 1342 patients had incomplete information on other PPF at enrollment. Among the 1342 patients with incomplete PPF, the majority (1315 of the 1342 patients) had erosive disease information missing, 22 were missing functional limitation, and 5 were missing functional limitation and erosive disease. CDAI: Clinical Disease Activity Index; RA: rheumatoid arthritis; PPF: poor prognostic factors.
Baseline demographic data and clinical characteristics.
Change in treatment acceleration from baseline to 12-month followup by number of PPF
The proportion of patients with biologic treatment during the 12-month followup period was lowest in the group with 0–1 PPF and highest in the group with 3+ PPF. In the 0–1, 2, and ≥ 3 PPF groups, respectively, 20.9%, 23.2%, and 26.5% of patients received 1 or more biologic (p = 0.011). In the 0–1, 2, and ≥ 3 PPF groups, respectively, 38.5%, 40.6%, and 41.7% of patients initiated treatment with any DMARD (p = 0.30).
Adjusted analyses controlling for age, sex, duration of RA, and CDAI showed that there was no statistically significant relationship between PPF category and the ability to predict biologic/tsDMARD use at the 12-month followup (≥ 3 PPF vs 0–1 PPF: OR 1.08, 95% CI 0.85–1.37; p = 0.57; Figure 2A). The proportion of patients with any treatment acceleration from baseline to the 12-month followup was similar between PPF groups, with no significant relationship between PPF category and treatment acceleration in both unadjusted and adjusted models (Figure 2B).

Logistic regression analysis of (A) biologic/tsDMARD initiation during the 12-month followup according to poor prognostic factor category, and (B) any treatment acceleration from baseline to 12-month followup according to poor prognostic factor category (0–1, n = 1489; 2, n = 1214; ≥ 3, n = 755). * p value was calculated based on an overall likelihood ratio test of the effect of poor prognosis on biologic use by 12-month followup. † Adjusted for age, sex, duration of RA, and CDAI. ‡ Addition of, or switching to, a conventional synthetic DMARD, and/or initiation of a biologic or tsDMARD. CDAI: Clinical Disease Activity Index; RA: rheumatoid arthritis; tsDMARD: targeted synthetic disease-modifying antirheumatic drug.
Change in disease activity from baseline to 12-month followup by number of PPF
After adjusting for CDAI at baseline, the mean (standard error) change in CDAI from baseline to the 12-month followup was −4.95 (0.24), −4.53 (0.27), and −2.52 (0.34) for the 0–1, 2, and ≥ 3 PPF groups, respectively (p < 0.001). Patients with moderate and/or severe disease activity at baseline (n = 1611) with ≥ 3 PPF were about half as likely to reach LDA/remission at the 12-month followup as patients with 0–1 PPF (OR 0.46, 95% CI 0.36–0.60; p < 0.001; Figure 3). After adjusting for CDAI at baseline, results remained similar (OR 0.51, 95% CI 0.39–0.66; p < 0.001) because the LDA/remission assessment included only patients with moderate and/or severe disease activity.
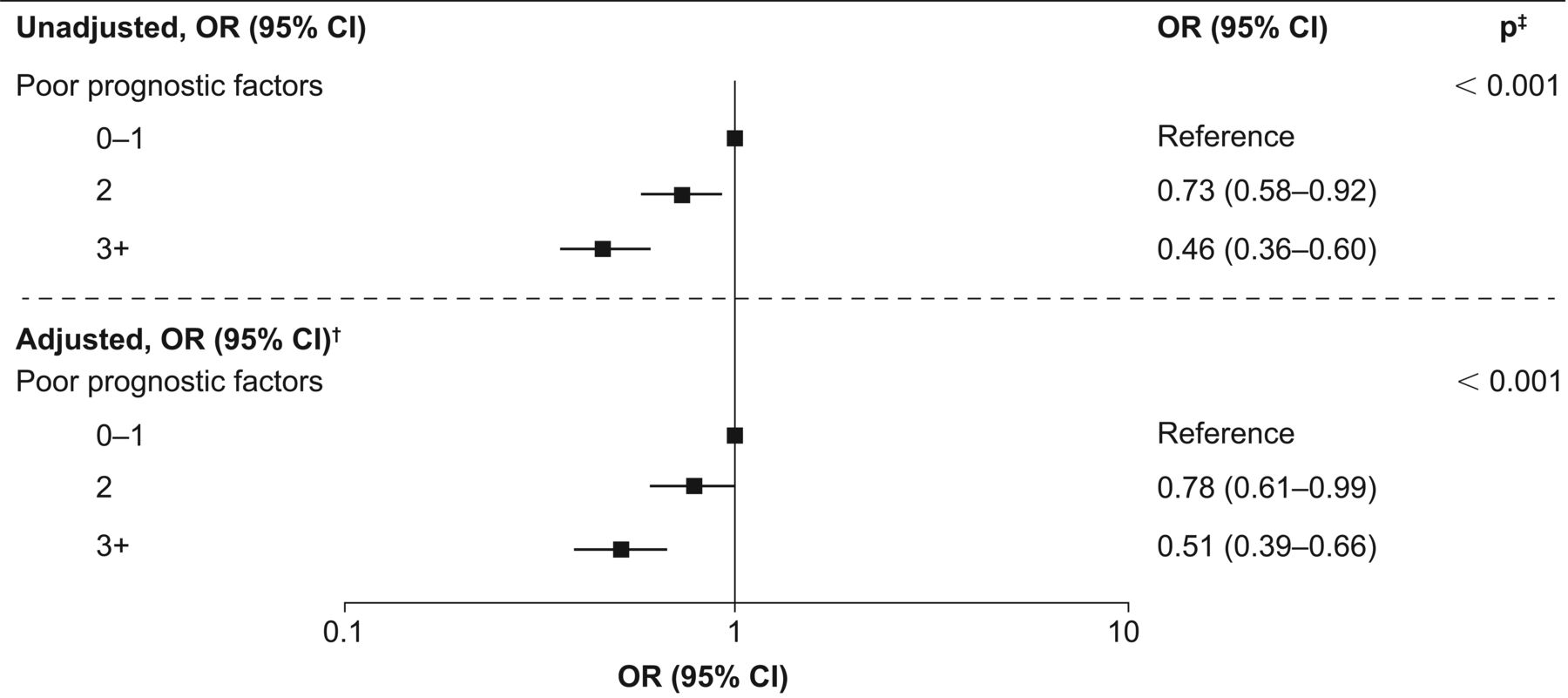
Logistic regression analysis of achievement of LDA/remission during the 12-month followup by number of PPF, among patients who had moderate and/or severe disease activity at baseline (0–1 PPF, n = 547; 2 PPF, n = 594; ≥ 3 PPF, n = 470). † P value was calculated based on an overall likelihood ratio test of the effect of poor prognosis on achievement of LDA/remission during the 12-month followup. ‡ Adjusted for CDAI at baseline. CDAI: Clinical Disease Activity Index; LDA: low disease activity; PPF: poor prognostic factors.
Change in work status from baseline to 12-month followup by number of PPF
At baseline, 46.6%, 43.7%, and 37.0% of patients with 0–1, 2, and ≥ 3 PPF, respectively, reported working full-time or part-time. At the 12-month followup, these figures were 44.8%, 40.8%, and 35.6%, respectively. After adjusting for age at baseline, a lower proportion of patients in the worst prognosis category were working full-time or part-time compared with those in the best prognosis category (p < 0.001 at baseline and p = 0.001 at followup; Table 2).
Work status (full-time or part-time vs all other categories) at baseline and 12-month followup by poor prognosis category after adjusting for age.
The proportion of patients whose work status changed over time (baseline to 12-mo followup) differed according to the number of PPF (Cochran–Mantel–Haenszel test; p < 0.001).
The proportion of patients working both at baseline and at the 12-month followup visit was highest (92.6%) in those with 0–1 PPF compared with the 2 and ≥ 3 groups (86.1% and 87.5%, respectively; Figure 4).

Work status (full-time or part-time vs all other categories) at baseline and 12-month followup by poor prognosis category (n = 3458).
In the less favorable PPF groups (2 and ≥ 3), higher proportions of patients were working at baseline but not at the 12-month followup (13.9% and 12.5%), compared with those in the best prognosis group (7.3%; Figure 4).
DISCUSSION
In this population of adult patients with RA, who were biologic- and tsDMARD-naive at enrollment into the Corrona registry, the number of PPF (based on ACR 2008 guidelines) did not influence treatment decisions. However, a greater number of PPF was associated with worse clinical outcomes, as well as lowered ability to work, at 12 months. In adjusted analyses, the changes in both CDAI and LDA/remission from baseline to the 12-month followup were significantly lower in patients with a greater number of PPF compared with those with 0–1 PPF. In addition, the proportion of patients with RA in full-time or part-time employment was directly associated with the number of PPF.
This was the largest real-world study to date, to our knowledge, to evaluate PPF in patients with RA. These results highlight the burden of PPF in patients with RA and the importance of evaluating these factors even in an established disease, which is common practice in other therapeutic areas such as cardiovascular disease. Our results suggest that, despite the worse outcomes in patients with a greater number of PPF, the presence of these factors did not significantly predict treatment accelerations in connection with the initiation of biologics or the addition/switching of therapies.
While the underlying mechanisms that result in patients with PPF having worse clinical outcomes are unknown, they warrant further investigation. In the meantime, providers may wish to reconsider how they approach treatment decisions for patients with PPF (e.g., it may be appropriate to follow these patients more closely than patients without PPF). Current treatment guidelines recommend treating patients to achieve a specific target, such as remission or LDA1,2,5,6; in line with this treat-to-target approach, physicians should routinely assess disease activity and adjust therapy until the specific target is achieved. As our results indicate, attainment of LDA was inversely associated with the number of prognostic factors. It may be beneficial to consider the use of prognostic factors to guide treatment decisions. Further, providers should engage patients in conversations about PPF and how they may wish to tailor their RA care based on this information.
A strength of this study is that Corrona is the largest national US registry in RA that contains both patient- and provider-reported measures and represents a typical practice setting in the United States. This was a real-world cohort of patients with varying durations of RA; hence, findings are more generalizable compared with controlled studies. However, given the observational nature of the design, there will likely be unmeasured confounding. In addition, operationalization of some of the outcome variables, such as work status, might underestimate the full productivity of patients with RA, because this study focused on full-time or part-time paid work only and classified patients working at home and students as “not working.” Corrona is a US registry, and it is possible that the results may differ in other countries13 and international registries.
Additionally, this study focused on only a subset of PPF, because there is not a widely accepted consensus definition14. The definitions of PPF in RA differ by region and therefore the introduction of further confounding is a possibility. The PPF investigated in our study were based on ACR 2008 definitions, because the study was conducted in the United States, with a study end date of December 2015. As a result, these were the treatment guidelines being used in clinical practice during the study period. It will be important to perform a similar analysis on guideline updates, to confirm the generalizability of these findings and compare with EULAR treatment recommendations.
The significant differences observed among patients based on the number of PPF (including age, sex, race, work status, smoking status, disease duration, prior number of csDMARD, and disease activity) deserve further study. Further, the study included only patients with a followup visit at 12 months, and additional analyses will be required to understand the effect of PPF on longterm treatment outcomes. Finally, this study excluded 4930 patients owing to a lack of documented data related to PPF; however, these patients were similar to the population with PPF included in the analyses regarding sex, age, median disease duration, and mean baseline disease activity.
Adjusted analyses showed that a greater number of PPF was not associated with a greater likelihood of biologic/tsDMARD initiation or any treatment acceleration (biologic, tsDMARD, or csDMARD). These findings suggest that the presence of PPF does not notably influence clinicians’ treatment decisions. This strategy warrants reconsideration because patients with a greater number of PPF had worse outcomes (including reduction in CDAI and achievement of LDA/remission) and were less likely to be in full-time or part-time work compared with those with fewer PPF in adjusted analyses. As the definition of a treat-to-target approach in RA evolves, providers may wish to consider incorporating the number of PPF into their conversations with patients regarding their treatment plan.
Acknowledgment
Professional medical writing and editorial assistance was provided by Claire Line, PhD, and Catriona McKay, PhD, at Caudex and was funded by Bristol-Myers Squibb.
Footnotes
Full Release Article. For details see Reprints and Permissions at jrheum.org
Sponsored by Corrona LLC. Corrona LLC has been supported through contracted subscriptions in the last 2 years by AbbVie, Amgen, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Crescendo, Eli Lilly and Co., Genentech, GSK, Horizon Pharma USA, Janssen, Momenta Pharmaceuticals, Novartis, Pfizer, Roche, and UCB. Bristol-Myers Squibb provided funding for the completion of the analysis and the development of the manuscript. EA, SEC, SK, and LR have stock options/bond holdings in Bristol-Myers Squibb. JMK has stock options/bond holdings in Corrona LLC and has received research grants from AbbVie, Lilly, Novartis, and Pfizer. LRH has stock options/bond holdings in Corrona LLC.
- Accepted for publication March 21, 2018.
Free online via JRheum Full Release option








{kind=link}
{kind=link}
{kind=link}
{kind=link}