
Abstract
Objective. To determine whether positive anticentromere antibody (ACA) serology affects the severity of sicca symptoms in patients with primary Sjögren syndrome (pSS).
Methods. Evaluation to detect subjective and objective sicca symptoms included questionnaires, physical examination, and pathology. Cases of pSS were classified according to the 2002 American-European Consensus Group (AECG) criteria. All patients were evaluated for presence of anti-Ro, anti-La, and ACA serology. Patients with pSS were categorized into ACA+ SS and ACA–SS. The groups were compared for measures of severity of oral and ocular sicca.
Results. The pSS group had 446 patients, of whom 26 were ACA+ SS. Subjective ocular sicca measured 7.0 ± 2.4 (out of 10) in ACA+ SS and 6.4 ± 2.6 in ACA–SS (p = 0.197). Objective ocular sicca measured 3.2 mm ± 1.8 mm/5 min in ACA+ SS and 4.2 mm ± 4.4 mm/5 min in ACA–SS (p = 0.038). Subjective oral sicca measured 8.5 ± 1.4 in ACA+ SS and 6.7 ± 2.4 in ACA–SS (p < 0.001). Objective oral sicca measured 0.1 ml ± 0.2 ml/15 min in ACA+ SS and 0.4 ml ± 1.0 ml/15 min in ACA–SS (p < 0.001). Only 35% of ACA+ patients with SS were anti-Ro–positive or anti-La–positive compared with 77% of the ACA–patients with SS (p < 0.001). There was no significant difference in minor salivary gland fibrosis or focus scores between ACA+ SS and ACA–patients with SS.
Conclusion. ACA+ SS is associated with more severe objective ocular sicca and more severe subjective and objective oral sicca compared to ACA–SS. The majority of ACA+ patients with SS meet AECG criteria for pSS despite negative serology for anti-Ro/La antibodies.
- SJÖGREN SYNDROME
- ANTICENTROMERE ANTIBODY
- SICCA SYMPTOMS
- PRIMARY SJÖGREN SYNDROME
The purpose of our study was to determine whether the presence of anticentromere antibodies (ACA) affects the severity of sicca signs and symptoms in patients diagnosed with primary Sjögren syndrome (pSS).
Sjögren syndrome (SS) is a chronic autoimmune disease that mainly affects the exocrine glands1. Sicca symptoms of xerophthalmia (ocular dryness) and xerostomia (oral dryness) are the most prevalent symptoms in SS1. In overlapping autoimmune disorders, there can be a clinical difference in the severity of at least one of the diseases2.
The American-European Consensus Group (AECG) classification criteria for SS defined secondary SS as the presence of signs and symptoms of dry eyes or dry mouth in another well-defined major connective tissue disease3. In 2012, the American College of Rheumatology proposed new classification criteria for SS that challenged the distinction between primary and secondary SS4. The terms primary and secondary regarding SS have been debated because overlap in connective tissue disease is common. It can often be unclear which disease occurred first, or if one was secondary to the other5,6,7. This is as true of SS as it is with any other connective tissue disease. The presence of ACA has been reported in 1.4–10.85% of patients with pSS7,8,9,10. Many of these patients have overlap features of limited cutaneous systemic sclerosis (lcSSc).
MATERIALS AND METHODS
Patients who were found at prescreening to have objective signs of dry eyes or dry mouth, positive anti-Ro or anti-La antibodies, or a history of parotitis were referred to the Multidisciplinary Sjögren’s Clinic at University Health Network, Toronto, Canada, for further evaluation. All patients were evaluated according to a standardized protocol between 1992 and 2014. Evaluation included patients’ global assessment of xerophthalmia and xerostomia on a standardized 10-cm visual analog scale (VAS).
Demographic features were collected for each patient in the study population. Data were collected on subjective and objective xerophthalmia and xerostomia in patients diagnosed with SS.
Xerophthalmia was objectively measured using the Schirmer-I test (S1T)11 and a van Bijsterveld scale for ocular staining using rose bengal or lissamine green12,13.
Unstimulated whole salivary flow (USSF)14 was measured after stopping all anticholinergic or sympathomimetic medication for 24 h. All patients evaluated had a minor salivary gland (MSG) biopsy and the results were assessed by the same pathologist according to a protocol for the presence of focal lymphocytic sialadenitis, and a focus score was assigned. Degree of fibrosis was also graded. A score of 0 meant no fibrosis. A score of 3 meant confluent fibrosis. Extractable nuclear antigens (ENA) and ACA were assayed using the BioPlex Multiplex 2200 test kit, which relies on indirect immunofluorescence.
For our purposes we counted each of the CREST manifestations [calcinosis, Raynaud phenomenon (RP), esophageal dysmotility, sclerodactyly, and telangiectasia] as a “feature” of lcSSc. All patients were evaluated for CREST manifestations by history and physical examination. Radiographs of the hands were performed in all patients. The protocols of our study adhered to the Declaration of Helsinki.
We used the AECG criteria to classify pSS3. Patients who met the pSS classification for primary SS were further categorized into ACA+ SS and ACA–SS. Groups were compared to determine differences in the prevalence of sicca symptoms, severity of sicca symptoms, and serological markers including IgG quantification and anti-Ro and anti-La antibodies.
A 2-tailed Student t test with heterogeneous variance was used to evaluate statistical significance when comparing differences between groups. A p value < 0.05 was considered statistically significant. All statistical analyses were conducted using SAS 9.3.
Ethics approval was received from the University Health Network Research Ethics Board at the University of Toronto for our study with submission number 19-5454.0. Patients’ written consent was waived because patient data was anonymized and no personal details could be identified.
RESULTS
Of 609 patients evaluated at the Multidisciplinary Sjögren’s Clinic, 446 met the AECG classification criteria for pSS. Within the pSS group, there were 26 patients with positive ACA serology. These 26 patients (5.8% of pSS group) were designated as ACA+ SS. There were 420 patients without ACA (94.2% of pSS group) and these were designated as ACA–SS.
The demographic characteristics of the 2 patient groups (ACA+ SS, ACA–SS) are summarized in Table 1. The process for patient enrollment is illustrated in Figure 1.

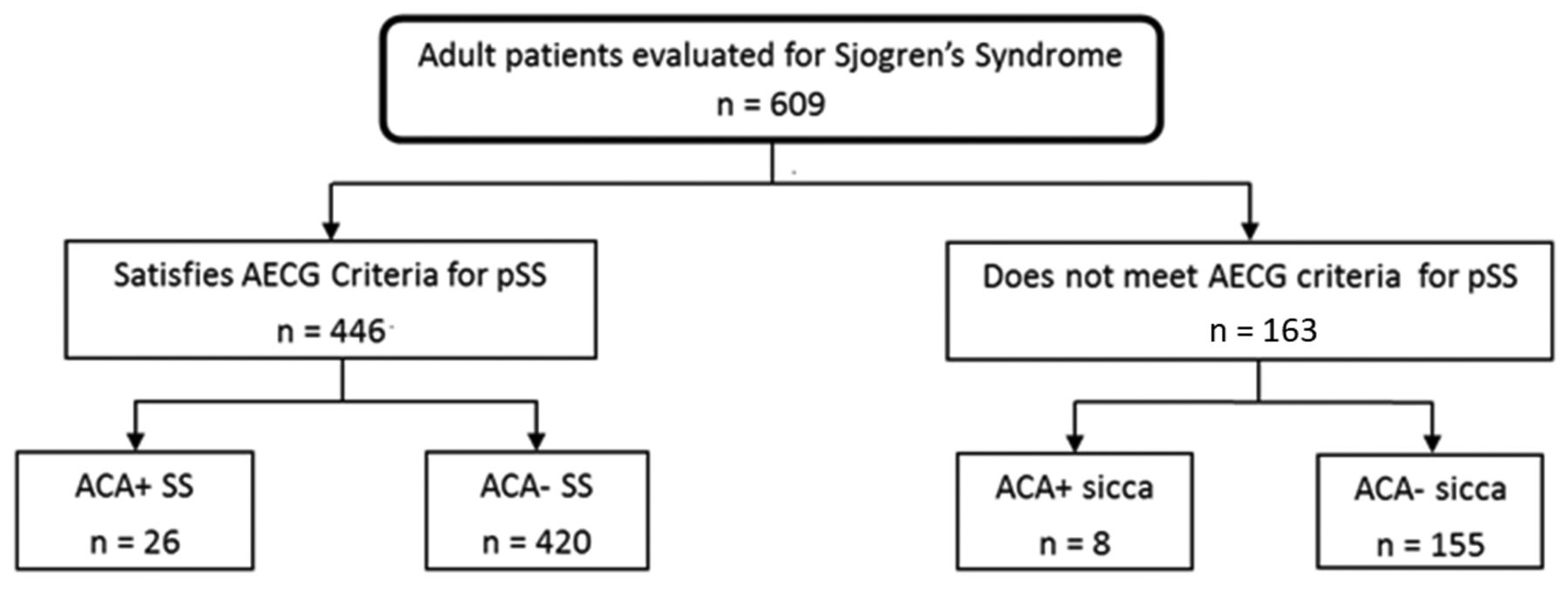{kind=link}
Flowchart for patient enrollment. AECG: American-European Consensus Group; SS: Sjögren syndrome; pSS: primary SS; ACA: anticentromere antibody.
Comparison between ACA+ SS and ACA–SS.
An additional 8 patients with ACA positivity were assessed in the Multidisciplinary Sjögren’s Clinic because of complaints of dry eyes or mouth. These patients did not satisfy the AECG classification criteria for pSS. There was no statistically significant difference in the prevalence or severity of sicca symptoms among ACA+ patients regardless of whether criteria for pSS were met.
Among the 446 patients with pSS, on a VAS, the mean severity of ocular sicca symptoms was 7.0 ± 2.4/10 in patients with ACA+ SS and 6.4 ± 2.6/10 in patients with ACA–SS (p = 0.197; Table 1). The mean S1T in patients with ACA+ SS was 3.2 mm ± 1.8 mm/5 min and in patients with ACA–SS, 4.2 mm ± 4.4 mm/5 min (p < 0.05). However, there was no difference in the mean van Bijsterveld score between ACA+ SS (5.7 ± 2.2/9) and ACA–SS (5.6 ± 2.3/9; p = 0.232).
On a VAS, the mean score for severity of oral sicca symptoms was 8.5 ± 1.4/10 in patients with ACA+ SS and 6.7 ± 2.4/10 in patients with ACA–SS (p < 0.001; Table 1). The mean value for USSF was 0.1 ml ± 0.2 ml/15 min for ACA+ SS and 0.4 ml ± 1.0 ml/15 min for ACA–SS. While this difference is statistically significant (p < 0.001), there is an overlap in SD between the 2 groups. Similarly, a greater number of patients with ACA+ SS had a focus score > 1 (92%) compared with ACA–patients with SS (84%). This difference was also highly significant (p < 0.001; Table 1). However, there was no statistically significant difference in the mean focus score between the ACA+ SS (focus score 5.5) and ACA–SS (focus score 4.0) groups. There was no significant difference in either the mean fibrosis score or the duration of xerophthalmia or xerostomia between the ACA+ SS and ACA–SS groups.
The CREST features in patients with ACA+ SS were not very severe or prevalent. Among patients with ACA+ SS, 58% had 2 or fewer stigmata of CREST syndrome, with RP and sclerodactyly being the predominant findings. Clinically, as expected, RP was more prevalent among patients with ACA+ SS (88%) than patients with ACA–SS (28%). This difference was highly significant (p < 0.001). There were no statistically significant differences between the 2 groups regarding extraglandular features such as dental problems (decayed, missing, or filled teeth), parotitis, parotid gland swelling, lymphoma, vasculitis, or hypothyroidism.
Serological differences
Elevated IgG was seen in 24% of the patients with ACA+ SS and 57% of the patients with ACA–SS (p < 0.001). There was a significant difference in the level of IgG between the ACA+ SS (12.4 g/l) and ACA–SS (19.4 g/l) groups (p < 0.001). Only 35% of the patients with ACA+ SS had positive serology for anti-Ro or anti-La antibodies compared with 77% of the patients with ACA–SS (p < 0.001). Nonetheless, these ACA-positive patients met the AECG classification criteria for pSS, mainly based on an abnormal MSG biopsy.
DISCUSSION
The presence of overlapping autoimmune diseases is not uncommon in patients who are being evaluated for SS. There is no doubt that 2 overlapping autoimmune diseases influence one another. SSc (defined by clinical features such as sclerodactyly) overlapping with pSS (SSc-SS) was characterized by milder SSc, with a lower severity and prevalence of sclerodactyly, lung fibrosis, and systemic involvement7. In a French cohort, Salliot and colleagues found that among the SSc-SS group (n = 20), there was a greater frequency of RP, objective xerophthalmia, peripheral neuropathy, arthritis, and additional autoimmune disorders, especially primary biliary cholangitis, compared to the SS group7. Similar to the ACA+ SS group in our study, they found that their patients with SSc-SS had a statistically significantly lower prevalence of specific autoantibodies including rheumatoid factor, anti-Ro, and anti-La compared to patients with SS7. In their cohort, SSc-SS overlap also displayed a classic SS phenotype with recurrent salivary gland enlargement, purpura, fatigue, arthralgia, and leukocytopenia7,8.
ACA is positive mainly in patients with SSc who have CREST features15 and has been detected in 50–96% of CREST syndrome patients9. The prevalence of ACA in SS has been reported as 1.4–10.85%7,8,9,10. In our cohort, positive ACA was seen in 5.8% of our patients with pSS. We have demonstrated that among pSS patients who are also ACA+, there is more severe dryness of the eyes as measured by the S1T, subjective xerostomia on VAS, and objective loss in saliva production (USSF). More patients with ACA+ SS had a focus score > 1 than did patients with ACA–pSS.
Previous studies have shown that patients with ACA+ SS have a lower prevalence of anti-Ro or anti-La antibodies16,17,18 compared with ACA–SS19,20. Among patients with SSc-SS, there is a 21–33% prevalence of positive anti-Ro antibodies2,16,18. Other groups have found that about 60% of their SSc patients with sicca symptoms were positive for anti-Ro antibodies2,17. Our results show a similar prevalence of anti-Ro or anti-La antibodies in 35% of patients with ACA+ SS.
The lower prevalence of anti-Ro and anti-La antibodies in the ACA+ SS group indicates that many of these patients depended upon the finding of a positive MSG biopsy to meet the AECG classification criteria. These are overlap cases and many would have been missed if classification as pSS depended upon the finding of anti-Ro/La antibodies (i.e., it is necessary to do the MSG biopsy to diagnose many ACA+ patients as having SS).
Avouac, et al notes that in biopsy samples from 50 (55%) of 91 patients with SSc and sicca complaints, they observed fibrotic lesions (considered mild in 13, moderate in 17, and severe in 20), and samples from 18 of the 91 patients (20%) had a focus score ≥ 12. Even though there is more fibrotic MSG involvement in patients with SSc with sicca2, patients with ACA+ SS are dry because of true inflammation in the salivary glands. Our results did not show a significant difference in MSG fibrosis between patients with ACA+ SS and patients with ACA–SS. We found a significantly higher proportion of patients with ACA+ SS with focus score ≥ 1 (92% vs 84%). However, there did not appear to be a difference between the focus scores of the patients with ACA+ SS and those with ACA–SS.
This raises major questions about the essential difference between progressive SSc and ACA+ lcSSc, where the overlap with SS is more frequent than would be expected, and the MSG biopsy pathology is more like SS than like SSc.
Sicca syndrome is common in SSc (60%) and is associated with salivary fibrosis7, more severe disease, and a higher mortality rate2. Abnormalities of collagen gene transcription may be responsible for tissue and vascular fibrosis, causing glandular fibrosis in SSc2,21. The pathology in the patients with ACA+ SS does not seem to follow this morphology.
A limitation of comparing the patients with ACA+ SS and those with ACA–SS in our study is that there are relatively few patients with ACA+ SS. Thus, each patient with ACA+ SS represents a greater fraction of the overall ACA+ SS group. However, our results show that there is a highly significant difference in severity of sicca symptoms and objective severity between the 2 groups.
Our findings indicate that the presence of ACA is associated with more severe xerostomia symptoms in patients diagnosed with pSS. ACA+ SS is associated with objective measures of more profound xerostomia and xerophthalmia compared to ACA–SS. Further, there is a higher prevalence of RP and a lower prevalence of anti-Ro and anti-La serology in patients with ACA+ SS. Aside from a difference in RP prevalence, there were no statistically significant differences in extraglandular manifestations between the 2 groups.
Last, the majority of patients with ACA+ SS meet the AECG criteria for pSS despite having negative serology for anti-Ro or anti-La antibodies. This may suggest that anti-Ro or anti-La serology may be less useful when trying to diagnose pSS in ACA+ patients. In view of evolving potential therapeutic tools for SS, and the finding of inflammatory rather than fibrotic pathology in ACA+ SS, our study also highlights the importance of doing an MSG biopsy in ACA+ patients with objective evidence of decreased salivary flow, decreased S1T, or abnormal van Bijsterveld staining. We take note of the essential difference in pathology of the MSG biopsy in ACA+ patients with sicca complaints compared to progressive SSc patients with similar sicca symptoms.
Footnotes
This project was made possible with the support of the Sjögren’s Society of Canada Summer Student Research Grant.
- Accepted for publication September 27, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.