
Abstract
Objective. Rheumatoid arthritis (RA) is associated with damage of the articular cartilage and the periarticular bone. While imaging of bone damage has substantially improved in recent years, direct imaging of the articular cartilage of the hand joints in patients with RA is still challenging. The study used T2 mapping of the finger joints to assess cartilage damage in RA.
Methods. Magnetic resonance imaging (MRI) at 3 Tesla was done in 30 patients with RA, and T2 relaxation times visualizing alteration in the collagen network and hydration of articular cartilage were mapped in 6 cartilage regions of the metacarpophalangeal (MCP) joints 2 and 3. Values were related to autoantibody status [anticitrullinated protein antibodies (ACPA), rheumatoid factor (RF)], disease duration, and disease activity as well as sex and age of the patients.
Results. T2 relaxation times could be reliably measured in the 6 regions of the MCP joints. Significantly higher relaxation times indicating more advanced cartilage alterations were observed in the metacarpal heads of ACPA-positive (p = 0.001–0.010) and RF-positive patients (p = 0.013–0.025) as well as those with longer disease duration (> 3 yrs; p = 0.028–0.043). Current disease activity, sex, and age did not influence T2 relaxation times.
Conclusion. These data show that cartilage damage can be localized and quantified in the hand joints of patients with RA by T2 mapping. Further, ACPA and RF positivity as well as disease duration appear to be the crucial factors influencing cartilage damage.
- MAGNETIC RESONANCE IMAGING
- T2 MAPPING
- CARTILAGE
- ANTICITRULLINATED PROTEIN ANTIBODIES
- RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is an inflammatory joint disease characterized by bone and cartilage damage1,2. While bone damage has been extensively characterized by conventional radiography, computed tomography, magnetic resonance imaging (MRI), and ultrasound (US)3–17, the assessment of cartilage damage in RA is in its infancy. To date, only joint space narrowing on conventional radiographs provides indirect evidence for cartilage damage. This is partly because articular cartilage in the hand joints is a rather small layer and therefore challenging to assess. Recent improvements in imaging technologies, such as increased resolution and new analysis modalities, may close this gap and permit direct analysis of articular cartilage of the hand joints. For instance, modern US devices with probes up to 22 MHz allow the depiction of cartilage of metacarpophalangeal (MCP) joints18,19. However, US is particularly user-dependent and has limitations in analyzing cartilage composition20. New MRI techniques such as delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) have also extended our insights into subtle structural changes of cartilage by displaying proteoglycan content after contrast enhancement. Cartilage imaging by dGEMRIC has been demonstrated in knee joints21 as well as MCP joints of patients with RA. In the latter study, the presence of anticitrullinated protein antibodies (ACPA) was associated with the accelerated loss of glycosaminoglycan content within cartilage22,23,24. An additional possibility to assess articular cartilage is T2 mapping by MRI. T2 mapping allows analyzing cartilage hydration and collagen integrity without contrast enhancement. T2 mapping has therefore been demonstrated as a sensitive tool to determine cartilage damage25,26,27. However, T2 mapping, especially of the finger joints, has not yet been used to assess cartilage damage in RA. Therefore, in our study we aimed to (1) introduce T2 mapping based on 3 Tesla (3T) MRI images in patients with RA, (2) quantify cartilage damage in the MCP joints, and (3) relate this damage to demographic and clinical data.
MATERIALS AND METHODS
Patient characteristics
Thirty patients with RA fulfilling the 2010 American College of Rheumatology/European League Against Rheumatism28 criteria of RA were analyzed. The study protocol was approved by the local ethics committee (medical faculty of Friedrich-Alexander-University Erlangen-Nuremberg, ethics approval number 263_12 B) and written informed consent was obtained from all patients. Demographic variables were recorded such as age and sex as well as disease-specific variables such as disease duration, disease activity according to 28-joint count Disease Activity Score using erythrocyte sedimentation rate (DAS28-ESR)29, the presence of rheumatoid factor (RF), and ACPA.
Image acquisition
All patients underwent MRI imaging of MCP joints 2 and 3 of the clinically most affected hand. Imaging was performed with a 3T whole-body scanner (VERIO; Siemens Healthcare) using two 4 cm–diameter surface coils (1 volar, 1 dorsal) to perform high-resolution imaging of both MCP joints, and to enable parallel imaging techniques. Patients had to lie down in a prone position with the hand being fixed with the thumb up in a brace to avoid movement artifacts. The MR protocol started with morphological sequences to ensure correct positioning of the coronal sequences. Then, a multi-echo, spin-echo sequence with 6 echoes for T2 mapping was used (Figure 1A). The repetition time was 1200 ms, the echo times were 15.8 ms, 31.4 ms, 47.4 ms, 63.2 ms, 79.0 ms, and 94.8 ms, and the flip angle was 180°. The imaged area consisted of 10 slides with a slice thickness of 1.5 mm and a field of view of 100 × 100 mm. The corresponding pixel matrix was 384 × 384, and the voxel size was 0.26 × 0.26 × 1.5 mm. The interpolated voxel size was 0.13 × 0.13 × 1.5 mm, and the bandwidth 200 Hz/Px.

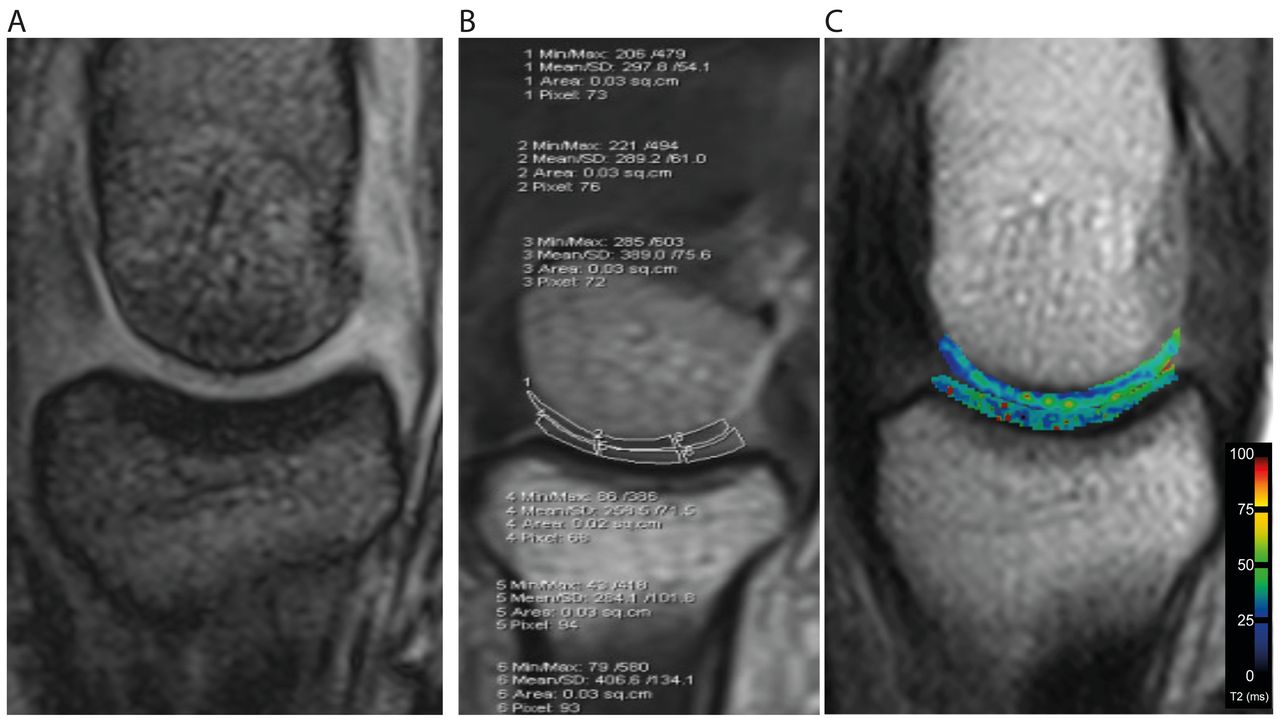{kind=link}
3 Tesla magnetic resonance imaging with T2 mapping. A. Enlarged morphological image of metacarpophalangeal (MCP) joint 2. B. Articular cartilage of the MCP joint was divided into 6 regions of interest (medial, central, and lateral region of the metacarpal head and the phalangeal base). C. T2 map (hybrid image) composed of the regional T2 relaxation times of MCP joint cartilage.
Image analysis
T2 maps were obtained using a pixel-wise, mono-exponential, non-negative least squares fit analysis. To avoid possible partial-volume effects, both layers were evaluated together. Region-of-interest (ROI) analysis was performed in both cartilage surfaces of the MCP joints. The ROI were applied manually and the T2 values for each ROI were calculated automatically by the computer. The distal cartilage layer of the metacarpal bone and the proximal cartilage layer of the proximal phalanx were analyzed by one imaging expert extensively trained in musculoskeletal MRI (GHW; > 10 yrs of experience) in consensus with 1 orthopedic surgeon (NR; 5 yrs of experience; Figure 1A and Figure 1B). Two consecutive central slides covering MCP2 and MCP3 were analyzed. To detect possible regional differences within joints, 3 ROI (medial, central, and lateral) were assessed on coronal correlated slices (Figure 1A).
For reliability measurements, 10 randomly selected patients were assessed on the basis of supplementary example measurements undertaken by the same observer and by a second independent one. Every assessor selected the slices anew at each assessment. The additional T2 data were collected by 2 independent (AK, NR) investigators for all ROI. This was used to quantify the interreader and the intrareader reliability regarding the intraclass correlation coefficient. During a patent application, one of the authors established the method for the used coil. At that time, there were both duplicate acquisitions and duplicate analyses. Because the method had already been established and was proved to be reliable before, we did not perform duplicate acquisitions.
All analyses were performed on a Leonardo Workstation (Siemens Healthcare). Rheumatoid Arthritis Magnetic Resonance Imaging Scoring (RAMRIS) totals were evaluated for MCP joints 2 and 3.
Statistical analysis
Collection, organization, and analysis were done by SPSS software for statistics (IBM SPSS 21.0, IBM Corp.). Categorical variables are presented as numbers and percentages, and continuous variables are provided as mean ± SD.
Assumptions of normally distributed continuous variables were tested using quantile-quantile plots as well as the Kolmogorov-Smirnov and Shapiro-Wilk test. After testing for Gaussian distribution, Mann-Whitney U tests or t tests for independent samples were applied as appropriate. T2 mapping values were compared between RA patients younger than 50 years and those older than 50 years. Also, a comparison was done between patients having RA for < 3 years and those having it longer, as well as a comparison between patients in remission and those not (remission being defined as DAS28-ESR < 2.6). Further, T2 values of patients who were autoantibody-positive were compared to values of autoantibody-negative patients. Analyses for interreader reliability were performed using an intraclass correlation coefficient (ICC). Analyses for testing the differences in the RAMRIS scores between MCP2 and MCP3 were performed using a Wilcoxon test. P values ≤ 0.05 were considered statistically significant.
RESULTS
Patient characteristics
Thirty patients with RA (21 women, 9 men) with a mean age of 53.5 ± 12.8 years were included. The disease duration was 5.8 ± 5.8 years and disease activity was 3.3 ± 1.6 units, measured by DAS28-ESR. Fourteen patients were ACPA- and 15 RF-positive. Age, sex, and disease duration were comparable between the ACPA-positive and ACPA-negative group.
Resolution evaluation
Mean numbers of pixels for the evaluated ROI were 80.4 ± 20.0 (medial metacarpal head), 91.6 ± 17.3 (central metacarpal head), 77.8 ± 30.3 (lateral metacarpal head), 83.0 ± 25.0 (medial phalangeal base), 92.0 ± 22.3 (central phalangeal base), and 77.6 ± 31.7 (lateral phalangeal base). We obtained these high values through the ultrahigh resolution of our technique.
T2 mapping in the MCP joints
We separately analyzed the T2 values in the medial, central, and lateral compartments of the second and third MCP joints. Results did not display any statistically significant difference between MCP2 and MCP3 joints, indicating consistent results in the various joint regions within individual patients. We therefore pooled results by calculating the average T2 values of the metacarpal cartilage and the phalangeal cartilage for MCP2 and MCP3 joints in all further analyses.
Reliability measurements revealed an ICC of 0.915 for the interreader reliability and 0.905 for the intrareader reliability.
Autoantibody status influences T2 relaxation times
Regarding ACPA status, the average T2 relaxation time was higher in ACPA-positive patients with RA in the vicinity of medial (41.3 ± 15.3 ms vs 29.6 ± 7.4 ms; p = 0.010), central (43.8 ± 14.6 ms vs 28.4 ± 10.9 ms, p = 0.001), and lateral metacarpal heads (45.6 ms ± 13.8 vs 32.0 ± 8.6 ms, p = 0.008). T2 relaxation times were higher in the central (29.9 ± 13.0 ms vs 22.5 ± 10.1 ms, p = 0.014) and lateral (37.0 ± 15.9 ms vs 28.8 ± 12.6 ms, p = 0.039) ROI of the phalangeal bases (Table 1). T2 relaxation times of metacarpal heads in RF-positive patients showed a similar pattern of cartilage damage, showing higher T2 values compared to RF-negative patients with RA (Table 1).
T2 relaxation times in the articular cartilage of patients with RA based on inflammatory disease activity and autoantibody status.
Disease duration of RA affects T2 mapping variables
Patients having RA for more than 3 years showed significantly higher T2 relaxation times compared to those patients with shorter disease duration. Significant differences were observed in the medial (40.1 ± 13.0 ms vs 30.1 ± 8.2 ms; p = 0.028), central (40.1 ± 13.3 ms vs 30.6 ± 9.4 ms; p = 0.043), and lateral ROI of metacarpal heads (43.6 ± 19.1 ms vs 32.4 ± 8.9 ms; p = 0.036). In the vicinity of phalangeal bases, significantly higher relaxation times were found in the medial (32.2 ± 20.4 ms vs 23.7 ± 8.1 ms; p = 0.009) and lateral (35.8 ± 16.9 ms vs 29.3 ± 11.3 ms; p = 0.04) compartment (Table 2).
T2 relaxation times in the articular cartilage of patients with RA based on disease duration, age, and sex.
Disease activity of RA and T2 mapping
We compared T2 relaxation times in patients in remission (DAS28 < 2.6) versus those without remission. In all ROI, no statistically significant difference was found between remission and non-remission patients (Table 2). Regarding the correlation of T2 relaxation times with RA disease activity, we also found no significant correlation in any of the 6 regions investigated (correlation coefficients between −0.227 and −0.031).
T2 relaxation time regarding sex and age
T2 relaxation times in younger patients (< 50 yrs) did not differ compared to older patients (> 50 yrs). No differences were found for the comparison of female and male patients (Table 2).
The comparison of the RAMRIS criteria between MCP2 and MCP3 for synovitis, erosions, and edema did not show statistically significant differences (synovitis MCP2 0.964 vs MCP3 0.928, p = 0.8497; erosions 1.750 vs 1.671, p = 0.515; and edema 0.428 vs 0.356, p = 0.665). The total MCP score of 3.143 vs 2.993 did not show a statistically significant difference either (p = 0.512).
DISCUSSION
Our study demonstrates the feasibility of T2 mapping of the articular cartilage of the second and third MCP joints in patients with RA. We performed a comprehensive analysis of cartilage changes at 6 different regions of the MCP joints. T2 relaxation times were higher in seropositive than seronegative patients with RA, indicating more severe cartilage damage in autoantibody-positive patients. The second factor influencing cartilage damage was disease duration, while no effects were found for the current disease activity or the age and sex of the patients.
RA is characterized by synovial inflammation that results in progressive destruction of articular cartilage as well as adjacent bone. ACPA and RF are known to be associated with increased bone damage and a more aggressive disease course30,31. Although the mechanisms leading to cartilage degradation are still not completely understood, the production of matrix cleaving enzymes by synovial inflammatory tissue is a central mechanism of cartilage degradation. A decrease in proteoglycans, changes of the collagen network, and a subsequent increase of cartilage permeability and water content are the earliest demonstrable changes in cartilage damage. These changes can be localized and quantified by new MR techniques such as T2 relaxation time mapping32. In the area where the bone comes into direct contact with the synovium, the contact area is larger in the proximal part of the joint33. The metacarpal head has more extensive contact on the surface with the synovium than the phalangeal base because of its outer shape. This could be a reason for the slightly higher average T2 values in the metacarpal head than in the phalangeal base. In early arthritis, the metacarpal head is affected more often than the phalangeal base34.
Our data support this concept, suggesting that longer exposure of the cartilage to RA-related synovitis leads to more pronounced changes. Even more interesting, the data also indicate that autoimmunity, as evidenced by ACPA and RF, augment cartilage degradation in RA. This finding is of particular clinical importance because autoimmunity develops years before the onset of arthritis35,36,37. It also extends imaging data that show bone and subclinical inflammatory changes in ACPA-positive individuals without the presence of RA12,13,38,39. It is currently unclear whether ACPA or RF can directly induce metabolic changes in chondrocytes or whether autoimmune-based cartilage damage develops as the consequence of underlying bone loss or subclinical inflammation, which are found in predisease individuals. Markovics, et al postulate that human cartilage proteoglycans (PG) might be subjected to citrullination under inflammatory conditions40. Citrullinated PG could provide a local source for local citrulline autoantigens in the rheumatoid joint and might partly explain direct effects of ACPA on cartilage.
Cartilage hyper-hydration measured by T2 mapping may be a reversible process. Hence, T2 mapping could serve as a specific instrument to detect and monitor cartilage alterations early in patients with RA. Thus the investigation of the cartilage layer of these pre-RA patients would be of great interest and could influence existing therapeutic algorithms. Further, it will be interesting to correlate changes in T2 values with the serum levels of serum cartilage biomarkers, different inflammatory cytokines, or different therapeutic approaches in future studies.
Because of the very thin cartilage layer of the MCP joints, it was very challenging to draw the ROI, and the surfaces of the second and third MCP are slightly bigger than those of the MCP4 and MCP5 joints. We intended to achieve a first overview and had to develop a protocol with realistic scan time and good image quality. The second and third MCP could be placed in the very center of the coil, reducing the risk of artifacts. Additionally, patients with highly active disease had difficulty keeping their hand still during the scan. Because of the extensive scan time, we reduced the number of slices, to shorten the scan times. At higher field strengths such as 7T it could be possible to reduce the scan time. This will be a topic for future studies in which all MCP joints will be investigated.
In our cohort of patients, we could not see a marked difference between the second and third MCP joints when looking at the RAMRIS scores. Hence, we did not examine the MCP2 and MCP3 separately. In the current study we specifically aimed to develop a rather objective and quantitative method for cartilage and joint assessment, which we see as a supplementary investigation with a specific focus on cartilage, to avoid semiquantitative assessments such as RAMRIS that assess cartilage indirectly by the presence of synovitis, erosions, and joint space narrowing. The lack of a marked difference between MCP2 and MCP3 regarding the RAMRIS scores in our cohort could be caused by the relatively small number of patients. In future studies with larger patient cohorts, the separate analysis of the metacarpal joints will enable an even more differentiated view of the changes in cartilage and other joint structures.
Because it is technically not easy to scan MCP joints 2–4 in a single acquisition session, we assessed the systemic effect of RA in 2 of the most affected joints in RA. We chose the second and third MCP joints because they could be placed in the very center of the coil that leads to a reduced risk of artifacts. Because of the very thin cartilage layer of the MCP joints, it was challenging to draw the ROI on the surface. The second and third MCP joints are slightly larger than the fourth and fifth MCP joints.
Our approach with pooled values for the second and third MCP joints is based on our opinion that the cartilage damage is evoked by the systemic effects of RA. Moreover, it is important to restate that the aim of our study was to visualize the early onset of cartilage damage in RA patients with positivity for anticyclic citrullinated peptide antibodies prior to the occurrence of irreversible damage such as joint space narrowing, erosion, synovitis, etc.
Our study has some limitations. It is a small cross-sectional study and thus prohibits drawing conclusions about the progression or reversibility of cartilage lesions. Such studies, however, will be necessary to judge the sensitivity to change of cartilage damage in RA. Nonetheless, these data support the concept that assessment of T2 relaxation times reflects disease-specific changes of the cartilage in RA, which are influenced by disease duration and presence of autoimmunity. The lack of adjustment between systemic disease characteristics and T2 mapping values can be seen as a limitation and will be a topic for future investigation.
Our study demonstrated that T2 mapping is a feasible procedure to directly detect cartilage alterations in RA patients. T2 mapping thereby allows accurate measuring of hydration changes and collagen fiber damage in the cartilage. The data also show that disease duration and presence of autoantibodies appear to be the main drivers for cartilage damage in RA.
Footnotes
This project was supported in part by the Interdisciplinary Center for Clinical Research at the University Hospital of the FAU (ELAN P005) and by the Emerging Fields Initiative (EFI) of the FAU and the STAEDTLER Stiftung (EFI_Verbund_Med_05_MIRACLE to GK, MLP, and AK).
- Accepted for publication July 30, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.