
Abstract
Objective. We investigated the association of age and anticyclic citrullinated peptide antibodies (anti-CCP) in subjects without rheumatoid arthritis (RA).
Methods. Serum was tested for anti-CCP3.1 (IgG/IgA) in 678 first-degree relatives (FDR) of patients with RA and 330 patients with osteoarthritis (OA). Individual isotypes (anti–CCP-IgA and anti–CCP-IgG) were also tested in all FDR.
Results. In FDR, increasing age was significantly associated with positivity for anti-CCP3.1 (per year, OR 1.03) and anti–CCP-IgA (per year, OR 1.05) but not anti–CCP-IgG. In FDR and OA subjects, anti-CCP3.1 prevalence was significantly increased after age 50 years.
Conclusion. Increasing age in individuals without RA should be considered in the interpretation of anti-CCP3.1 positivity.
- RHEUMATOID ARTHRITIS
- ANTICYCLIC CITRULLINATED PEPTIDE ANTIBODIES
- AGE
Antibodies to citrullinated protein antigens (ACPA) play an important role in rheumatoid arthritis (RA) pathogenesis and can be detected several years before the onset of inflammatory arthritis (IA) during a preclinical period of autoimmunity1,2. Understanding how ACPA develop in individuals without RA is informative to better delineate RA pathogenesis. Commercial ACPA assays for anticyclic citrullinated peptide antibodies (anti-CCP) detect IgG-ACPA only (CCP2, CCP3) or both IgG-ACPA and IgA-ACPA with the CCP3.1 assay that was developed to add sensitivity in early RA diagnosis3. While IgG-ACPA and IgA-ACPA are both specific for predicting future classifiable RA4, they associate with different RA features, suggesting that different ACPA isotypes can be associated with different aspects of RA pathogenesis5.
When considering factors that could influence ACPA, age is of interest because several autoantibodies are associated with increasing age6,7,8,9, and ACPA positivity is higher in older RA-free women10. However, the influence of age on isotype-specific ACPA has not been thoroughly investigated. Therefore, we evaluated the relationship of IgA-ACPA and IgG-ACPA with age in subjects without RA.
MATERIALS AND METHODS
Study subjects
In this cross-sectional study, we included stored serum from 2 groups: (1) first-degree relatives (FDR) of patients with RA; and (2) subjects with osteoarthritis (OA). Both cohorts had no history of clinically evident IA, therefore meeting no definable criteria for RA. For FDR, 678 were randomly selected from the Studies of the Etiology of RA (SERA) cohort that includes a total of 1754 FDR without a history of IA11. Demographics and smoking history were obtained by questionnaire. For the OA cohort, 330 subjects were included who were previously recruited from Veterans Affairs Medical Centers and 1 academic medical center as a control group in a study examining environmental risk factors for RA12. Medical record review was performed to obtain demographics and smoking history and to exclude the presence of IA. Family history of RA was not obtained.
Ethics
All study-related procedures were approved by the institutional review boards at each site (University of Colorado ethics board approval COMIRB #01-675). Informed written consent was obtained for all subjects for publication of data.
Autoantibody, total Ig, and shared epitope testing
In all subjects, serum was tested for ACPA using commercial CCP3.1 ELISA (IgG/IgA, Inova Diagnostics Inc.). All FDR were also tested for isotype-specific anti–CCP-IgA and anti–CCP-IgG using a CCP3 plate with the respective secondary antibody conjugate (Inova, for research only). For anti–CCP-IgA and anti–CCP-IgG, an in-house standard curve was generated from pooled RA subject serum. Cutoff levels for IgA-ACPA and IgG-ACPA positivity were set at the 98th percentile in a separate set of 126 healthy controls (no FDR with RA, mean age 36 yrs, 81% female).
Additional serum testing had previously been completed on FDR as part of the SERA study11 including testing for CCP2 (IgG, Diastat, Axis-Shield Diagnostics Ltd.) and rheumatoid factor (RF) by nephelometry (Dade-Behring) in all FDR, for anti-CCP3 (IgG, Inova) in a random selection of 338 of the 678 FDR, and for total IgA and IgG (Beckman-Coulter Synchron nephelometry system) in 108 FDR who had previously participated in lung-related SERA studies13. All OA subjects were also tested for anti-CCP3 (IgG, Inova). Positivity for all commercial CCP assays was based on manufacturer recommendations. RF cutoff levels for positivity were set at the 95th percentile in 491 anonymous blood donors. Subjects were also tested for presence of shared epitope alleles using previously described methodologies11.
Statistical analysis
Univariate and multivariate logistic regression was used to determine associations between age as a continuous variable in years and ACPA positivity (Supplementary Data 1 and Supplementary Table 1, available with the online version of this article). We also compared prevalence of ACPA positivity between age groups as a categorical variable (by decade) using chi-square/Fisher’s exact testing, with the youngest decade (18–29 yrs) serving as the referent group. We used Cohen’s κ to compare agreement between assays, McNemar’s test to compare anti-CCP positivity within groups, and Pearson correlation to compare age and total Ig levels. Analyses were completed using SPSS24 (IBM) and SAS9.4 (SAS Institute Inc.).
RESULTS
Anti-CCP3.1 and age in FDR
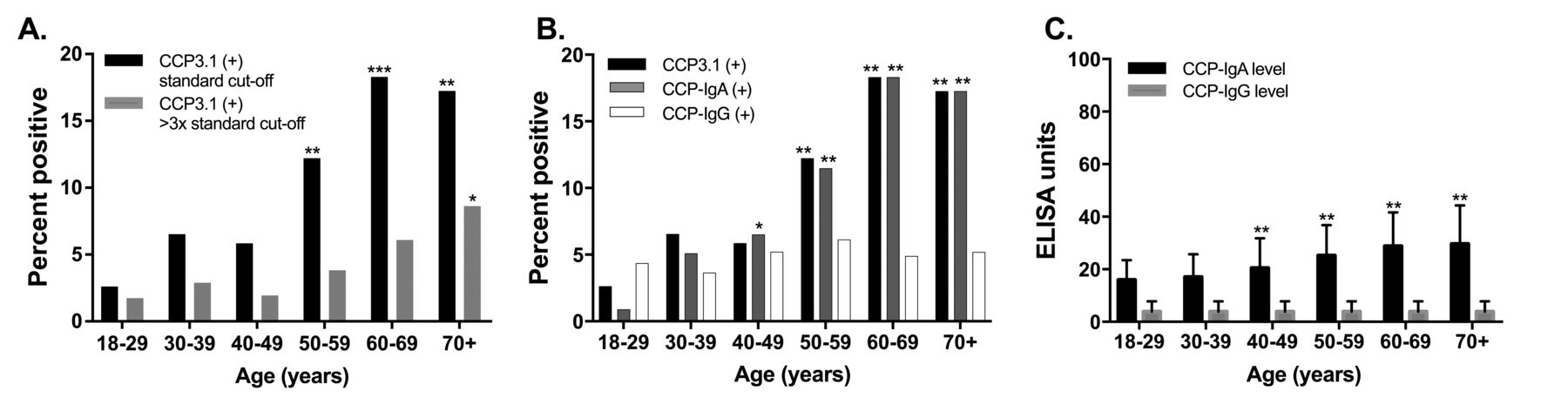
Subject demographics are in Table 1. In FDR, 62/678 (9.1%) were anti-CCP3.1–positive. There was a significant association between anti-CCP3.1 positivity and increasing age (OR 1.04, 95% CI 1.02–1.05) that remained significant in the adjusted model (Table 2). Compared to the 18- to 29-year-old referent group, anti-CCP3.1 positivity was more prevalent in all age groups ≥ 50 years (i.e., 50–59, 60–69, and ≥ 70 yrs; Figure 1A; Supplementary Table 2, available with the online version of this article). To account for the low prevalence of positivity in 18- to 29-year-olds, we also performed comparisons using a larger referent group of 18- to 39-year-old FDR and found similar results (Supplementary Table 3, available with the online version of this article). When stratified by sex, anti-CCP3.1 was associated with age in both women (1.03, 95% CI 1.01–1.05) and men (OR 1.07, 95% CI 1.02–1.11).

{kind=link}
Anti-CCP positivity and levels by age group in SERA FDR. A. The percentage of FDR with anti-CCP3.1 positivity at standard cutoff levels (black bars) and at 3× the standard cutoff level (gray bars) by age group. B. The percentage of FDR with anti-CCP3.1 positivity (black bars), anti–CCP-IgA positivity (gray bars) and anti–CCP-IgG positivity (white bars) by age group. C. The median level (IQR) for anti–CCP-IgA (black bars) and anti–CCP-IgG (gray bars) by age group. * P < 0.05. ** P < 0.01 comparing each outcome to the same outcome in the 18- to 29-year-old reference age group. The total number of FDR included in each age group includes n = 115 for 18–29 years, n = 138 for 30–39 years, n = 154 for 40–49 years, n = 131 for 50–59 years, n = 82 for 60–69 years, and n = 58 for ≥ 70 years. SERA: Studies of the Etiology of Rheumatoid Arthritis; anti-CCP: anticyclic citrullinated peptide antibodies; FDR: first-degree relatives; IQR: interquartile range.
Subject characteristics.
Associations of age and ACPA positivity in SERA FDR.
IgA-ACPA, IgG-ACPA, and age in FDR
In FDR, 58/678 (8.6%) were anti–CCP-IgA–positive and 33/678 (4.9%) were anti–CCP-IgG–positive. Similar to anti-CCP3.1, anti–CCP-IgA positivity was associated with increasing age overall (OR 1.04, 95% CI 1.03–1.06; Table 2) and in both women (OR 1.04, 95% CI 1.02–1.06) and men (OR 1.09, 95% CI 1.04–1.15). Compared to the referent group, anti–CCP-IgA was more prevalent in FDR in all age groups ≥ 40 years (i.e., 40–49, 50–59, 60–69, and ≥ 70 yrs; Figure 1B; Supplementary Table 2, available with the online version of this article). There was no association between anti–CCP-IgG and age (Table 2). There was good agreement between anti-CCP3.1 and anti–CCP-IgA or anti–CCP-IgG positivity (κ = 0.68).
Anti-CCP2, anti-CCP3, RF, and total Ig in FDR
Using commercial CCP assays that detect only IgG reactivity, 19/678 (2.8%) FDR were anti-CCP2–positive and 19/388 (4.9%) were anti-CCP3–positive. There was no association between age and anti-CCP2 or anti-CCP3 positivity in FDR (p = 0.63 and p = 0.43, respectively). In addition, 41/678 (6.0%) FDR were RF-positive, and again with no association between age and positivity (p = 0.26). There was also no association between age and level of total IgG or total IgA (p = 0.27 and p = 0.42, respectively).
Anti-CCP in OA subjects
To investigate whether the association of anti-CCP3.1 and age was specific to FDR, we studied a separate cohort of older subjects with OA. There was a trend toward an association between anti-CCP3.1 positivity and increasing age in OA subjects (OR 1.04, 95% CI 1.0–1.07).
Further, anti-CCP3.1 was more prevalent than anti-CCP3 positivity in OA subjects ≥ 50 years [25/275 (9.1%) vs 11/275 (4.0%), p < 0.01], but not in OA subjects < 50 years [3/55 (5.5%) vs 3/55 (5.5%), p = 1.0]. In addition, FDR ≥ 50 years were more likely than OA subjects ≥ 50 years to be anti-CCP3.1–positive [41/271 (15.1%) vs 25/275 (9.1%), p = 0.03].
DISCUSSION
We identified a significant association between anti-CCP3.1 positivity and increasing age in subjects without RA, which appears to be driven by anti–CCP-IgA. While both FDR and OA subjects ≥ 50 years had increased anti-CCP3.1 positivity, this association was stronger in FDR, suggesting that other familial or shared environmental components may contribute to ACPA development in older subjects. In contrast to prior reports10,14, we identified a significant association between anti-CCP3.1 and age in both women and men, suggesting that the higher prevalence of ACPA in older individuals may be more generally related to aging rather than a hormonal effect specific to women. While our study focused on subjects without RA, we did not identify a similar association between anti-CCP3.1 and increasing age in SERA subjects with established RA (data not shown), although it could be that this relationship is masked by the high prevalence of anti-CCP3.1 positivity in RA. It is of interest that an association between anti-CCP secretory IgA and increasing age has been described in subjects with early-classified RA15, although this study did not specifically exclude the possibility of anti-CCP secretory IgM16.
Several features of aging could potentially contribute to ACPA development including the accumulation of oxidative posttranslational protein modifications and increased self-reactive IgA that are not always associated with tissue injury7. Older individuals also have increased dysfunctional terminally differentiated B cells hypothesized to secrete antibodies in response to chronic antigen stimulation by persistent viruses or autoantigens17. Autoantibodies in older individuals may also have regulatory functions such as targeting senescent cells for clearance to maintain homeostasis and balance the wear and tear of aging18.
Regarding the clinical effect of our findings, our data highlight the importance of considering age in the interpretation of anti-CCP3.1 in subjects without IA. While not all clinical laboratories use CCP3.1, some of the largest reference laboratories (e.g. Lab-Corp) currently use CCP3.1, supporting clinical relevance of our findings. Further, because assay specificity is based on performance within a disease-free population, the specificity of anti-CCP3.1 for RA would be decreased in older individuals. In addition, elderly-onset RA may differ in antibody profiles compared to those with younger onset. Regarding the effect of our findings on RA pathogenesis, our findings align with the hypothesis that early ACPA generation may begin at an IgA-predominant mucosal site13,19,20. However, autoreactive IgA may also be less pathogenic than IgG7, and IgA-ACPA alone may be less predictive of developing classified RA4.
Caveats to our study include the cross-sectional design and lack of RA family history in OA subjects that would be needed to confirm that age was responsible for the increased ACPA prevalence independent of RA family history. Further, because our OA cohort members were chosen based on their older mean age, it included a limited number of younger individuals for comparison. In addition, because IgG-ACPA is more predictive of developing RA1, IgG-ACPA–positive non-RA subjects may more rapidly develop classified RA, resulting in lower IgG-ACPA positivity in older non-RA cohorts. As expected, we found good agreement between anti-CCP3.1 (IgG/IgA) positivity and the individual isotypes anti–CCP-IgA or anti–CCP-IgG positivity. We assume that the increased anti-CCP3.1 positivity in OA subjects ≥ 50 years was driven by IgA-ACPA, but individual IgA-ACPA testing should be performed to confirm. Future studies are also needed to evaluate associations of age and secretory IgA-ACPA, to determine specific epitopes targeted by ACPA in older individuals, and to establish the performance of anti-CCP3.1 positivity to predict future classified RA in older individuals.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors thank all the subjects who participated in this study.
Footnotes
M. Mahler is an employee of Inova Diagnostics.
This work was supported by the US National Institutes of Health (NIH; grant numbers AR066712, AI110503, AI101981, and T32AR007534), and a Rheumatology Research Foundation Resident Research Preceptorship Award. Contents are the authors’ sole responsibility and do not necessarily represent official NIH views.
- Accepted for publication April 1, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.