
Abstract
Objectives. Chronic nonbacterial osteomyelitis (CNO) is a sterile inflammatory bone disorder with an unpredictable disease course. The objective was to assess clinical and radiological disease activity in children with CNO including response to early-onset pamidronate treatment.
Methods. A single-center retrospective study was conducted of children fulfilling the Bristol Criteria for CNO. At the time of diagnosis, whole-body magnetic resonance imaging (WB-MRI) or local MRI was performed to assess radiological disease activity. Children with multifocal or spinal bone inflammation and clinical disease activity not responding to nonsteroidal antiinflammatory drugs were categorized as having extended CNO. Clinical disease activity was assessed annually.
Results. Fifty-one children were included. Median followup time was 4 years (interquartile range 3–7). Children categorized with extended CNO (n = 32) were treated in an early-onset 2-year pamidronate regimen. In extended CNO, WB-MRI was performed at time of diagnosis, and at years 1 and 2 in 88%, 84%, and 91% of cases, respectively. During the first year, the total number of radiologically active lesions and number of spinal lesions per patient declined (p = 0.01). Clinically inactive disease was recorded in 12/32 children (38%). However, 8/12 children (67%) experienced clinical relapse. In limited CNO (n = 19), 10/19 children (53%) presented with clinically inactive disease after 1 year and did not experience clinical relapse.
Conclusion. Pamidronate might contribute to improvement in clinical and radiological disease activity in extended CNO, especially after 1 year of treatment. However, children with continuously active disease after 2 years of pamidronate treatment were seen.
- CHRONIC RECURRENT MULTIFOCAL OSTEOMYELITIS
- DIPHOSPHONATES
- MAGNETIC RESONANCE IMAGING
- ANTIRHEUMATIC AGENTS
Chronic nonbacterial osteomyelitis (CNO) is a sterile and often multifocal osseous inflammatory disorder. Symptoms include musculoskeletal pain, tenderness, swelling, and limited range of motion of the skeletal sites involved1. Inflammatory comorbidity, for example, synovitis, sacroiliitis, and psoriasis is reported in 30% of patients with CNO. CNO has been suggested as the juvenile form of SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) syndrome and can develop into non-HLA-B27–related spondyloarthropathy2,3,4.
Bone lesions may involve all parts of the skeleton, but have a predilection for growth plate areas of the long tubular bones in the lower extremities, the clavicles, and the vertebrae3,5. Whole-body magnetic resonance imaging (WB-MRI) has been shown to be useful in diagnostics, especially in the assessment of multifocality and clinically silent lesions, as well as in the decision-making process regarding treatment and followup strategy6,7,8,9.
In some cases, CNO may cause only moderate symptoms and be self-limiting. However, in a subset of children, disease activity persists into adulthood. There is a risk of bone deformities such as vertebral fractures, and CNO can lead to persistent pain and disability. Multifocal bone lesions, especially involving the spine, and elevated inflammatory markers indicate clinically challenging disease5,10,11,12.
Treatment of CNO is mainly empirical and may differ among physicians12. Nonsteroidal antiinflammatory drugs (NSAID) are recommended as first-line therapy13,14. NSAID have been reported to control pain in 43–83% of patients3,15. In children with persistent CNO, case reports have suggested that the amino bisphosphonate pamidronate and tumor necrosis factor (TNF)–α inhibitors are effective in patients not responding sufficiently to NSAID16,17. Duration of symptoms before initiation of second-line treatment is often up to 2 years18,19,20.
Pamidronate binds to the surface of bone and becomes internalized into osteoclasts. This reduces normal osteoclast activity because it induces cell apoptosis and aberration of signaling functions of regulatory proteins21. In vitro pamidronate has an antiinflammatory effect, affecting macrophage function and inhibiting secretion of proinflammatory cytokines22,23.
TNF-α inhibitors are used as monotherapy or in combination with pamidronate24,25. TNF-α inhibitors suppress the proinflammatory response. In patients with CNO and inflammatory comorbidity, such as inflammatory bowel disease (IBD) or synovitis, TNF-α inhibitors are often the preferred treatment26.
Our objective was to investigate the clinical and the radiological disease activity in CNO and to assess the response to early-onset pamidronate treatment.
MATERIALS AND METHODS
A retrospective review was performed of children diagnosed with CNO at a tertiary hospital between 2007 and 2015. The study was conducted at the Department of Pediatrics and Adolescent Medicine, Aarhus University Hospital, Denmark. A systematic search in the hospital clinical database was conducted for the International Classification of Diseases (ICD)-10 code DM86.3 for chronic multifocal osteomyelitis. Approval from the regional ethics committee and the Danish Data Protection Agency was applied for but not needed. The Institutional Review Board approved the study (ref. 2016-04-11-1).
Diagnosis and clinical characteristics
All children fulfilled the Bristol Criteria for CNO27. A multidisciplinary team with attendance from expert pediatric consultant radiologists and consultant pediatric rheumatologists confirmed the diagnoses. Children were categorized as having extended or limited CNO. Children with symmetric multifocal or spinal bone inflammation assessed by MRI and a poor clinical response to NSAID were categorized as having extended CNO.
Data were collected from electronic medical records on age, sex, time of first symptoms, time of diagnosis, comorbidity, concomitant medication [NSAID, antibiotics, glucocorticoids, methotrexate (MTX), pamidronate, TNF-α inhibitors], and laboratory screening [complete blood cell count, erythrocyte sedimentation rate (ESR), liver enzymes, calcium, and antigen HLA-B27 status]. Data also were compiled regarding reviews of histopathological reports from bone biopsies and imaging.
Imaging
To assess bone lesions at time of diagnosis, either WB-MRI, bone scintigraphy, and/or local MRI was performed. WB-MRI was performed with a 1.5 Tesla scanner. WB-MRI short-tau inversion recovery (STIR) was performed in a coronal plane and supplemented by axial or sagittal STIR locally when needed for adequate evaluation of lesions. Sagittal STIR of the spine was performed in cases of spinal involvement. Additional T1-weighted images were performed if indicated on STIR images. Radiologically active bone lesions were defined as areas presenting abnormal, increased signal intensity on STIR images. Radiological remission was defined as no active bone lesions on MRI followup. The imaging findings used were based on reports performed by expert pediatric consultant radiologists. Anatomic sites of bone lesions and skeletal deformations were recorded at the time of diagnosis, and in children with extended CNO after 1 and 2 years. Followup imaging was not systematically performed in limited CNO.
Clinical disease activity
Clinically inactive disease was defined as patients having no experience of symptoms, no reported sign of inflammation, and normal ESR. We defined symptoms as patient- or parent-reported musculoskeletal pain, swelling or limited range of motion of the involved skeletal sites since last followup visit. Physician-reported signs of inflammation were defined as local swelling or heating of the affected skeletal site. Elevated ESR (> 20 mm/h) attributable to CNO was used as a biochemical inflammatory marker. Clinically inactive disease while taking medication was defined as 6 consecutive months of clinically inactive disease while taking medication. Clinically inactive disease while not taking medication was defined as 12 consecutive months of clinically inactive disease while not taking medication. The definitions on the duration of medication (6 or 12 mos, respectively) were chosen with reference to Wallace, et al’s preliminary criteria for inactive disease and clinical remission in juvenile idiopathic arthritis28.
Information on clinical disease activity was assessed from the annual followup visit from the time of diagnosis (± 2 mos). Children presenting continuously clinically inactive disease while not taking medication were no longer followed in the outpatient clinic and were lost to followup.
Treatment
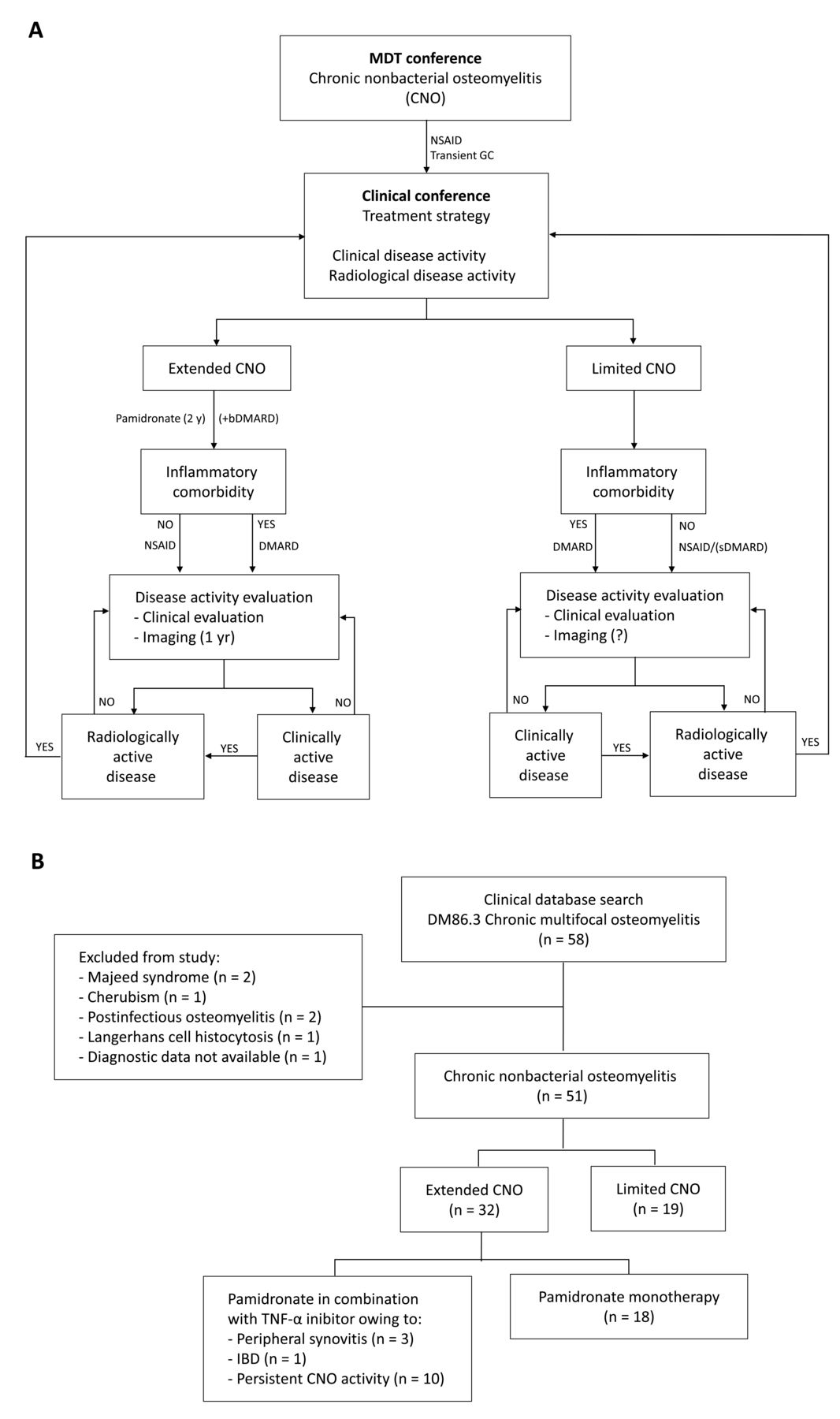
NSAID was the first choice of treatment and was considered a disease-modifying drug. Transient glucocorticoids were sometimes used initially. The decision to change or initiate treatment depended on clinical and radiological disease activity (Figure 1). The decision to initiate or change to second-line treatment was made at a clinical conference with at least 1 consultant pediatric rheumatologist attending. In children categorized with extended CNO, intravenous pamidronate was prescribed for 2 years, 1 mg/kg/day (maximum 60 mg/day) for 3 consecutive days every 3 months, first dose in the first series 0.5 mg/kg/day. Children with extended CNO and persistent clinically active disease and radiologically active disease despite pamidronate treatment were given biological disease-modifying antirheumatic drugs (bDMARD) in combination with pamidronate or as monotherapy. Children with inflammatory comorbidities not responding to synthetic DMARD were treated with bDMARD alone or in combination with pamidronate. The first choice of biological DMARD was a TNF-α inhibitor (Figure 1).
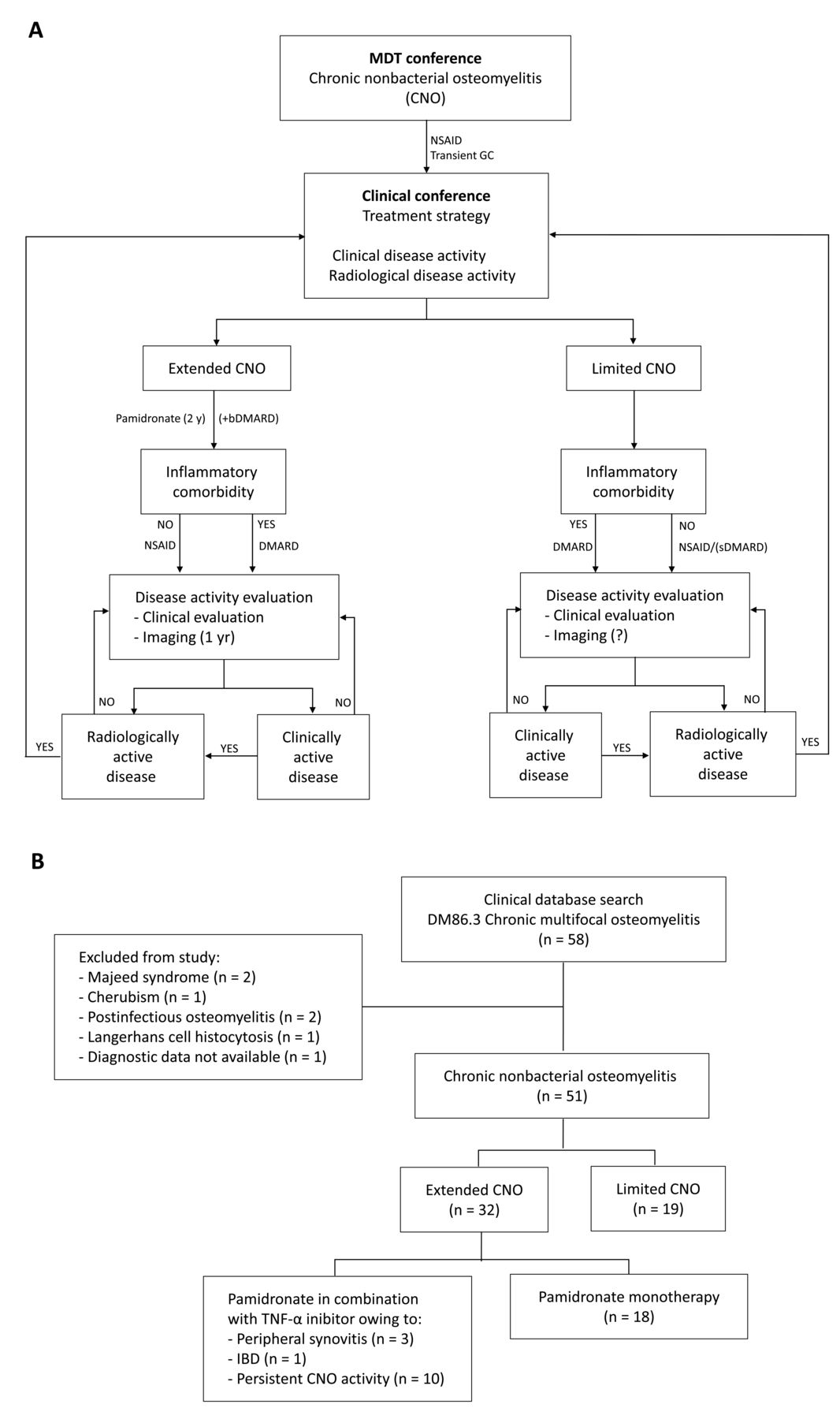
A. Suggested management of chronic nonbacterial osteomyelitis (CNO). The diagnosis of CNO was confirmed at a multidisciplinary team (MDT) conference. First choice of treatment was nonsteroidal antiinflammatory drugs (NSAID) with or without transient glucocorticoids (GC). Treatment strategy was decided at a clinical conference. Children categorized with extended CNO were treated with pamidronate for 2 years. Children with inflammatory comorbidities were treated with synthetic disease-modifying antirheumatic drugs (sDMARD) or biological DMARD (bDMARD) alone or in combination with pamidronate. Children with extended CNO and persistent clinical disease activity and radiological disease activity despite pamidronate treatment were given bDMARD in combination with pamidronate or as monotherapy. In extended CNO, clinical evaluation was performed every 3 months and radiological evaluation following 1 year of treatment or if clinically indicated. B. Results from systematic search in clinical database, ICD-10 code DM86.3, chronic multifocal osteomyelitis. Children included met the Bristol Criteria for CNO. Children were categorized as extended or limited CNO. Treatment strategy follows the algorithm suggested in panel A. TNF: tumor necrosis factor; IBD: inflammatory bowel disease; ICD-10: International Classification of Diseases, 10th ed.
Statistics
Statistical analyses were performed using Stata 14 (StataCorp). Normally distributed data were presented as mean (95% CI). Data not being normally distributed were log-transformed, checked for normality, and presented as geometric mean (95% CI). Data not normally distributed were presented as median (1st–3rd quartile). Categorical variables were reported as numbers (percentage) and compared using unpaired/paired sample Student’s t test or the Wilcoxon signed-rank test, respectively. Fisher’s exact test was used for comparison of nonpaired dichotomous data and McNemar’s test for comparison of paired dichotomous data. P values < 0.05 were considered statistically significant.
RESULTS
Diagnosis and clinical characteristics
We reviewed 58 medical records. Seven children were excluded from analysis because of missing diagnostic information (n = 1) or misclassification (n = 6; Figure 1). Bacterial osteomyelitis was initially suspected in 7/51 children (14%) with CNO.
A WB-MRI was performed in 39/51 children (76%) at time of diagnosis. In children without a WB-MRI, a bone scintigraphy combined with local MRI was performed in 3/51 children (6%) or a local MRI alone in 9/51 children (18%). A bone biopsy was performed in 38/51 children (75%), all excluding infection, malignant, and benign tumors (Table 1).
Diagnostic characteristics of children with chronic nonbacterial osteomyelitis (CNO).
The diagnosis of CNO was confirmed in 51 children; 32/51 children (63%) were categorized as having extended CNO and 19/51 (37%) as having limited CNO (Figure 1). Median clinical followup time was 4 years (3–7). Diagnostic characteristics are listed in Table 1).
Inflammatory comorbidity was present in 15/51 children (29%; Table 1). A first-degree relative with autoinflammatory disease was reported in 5/51 children (10%): IBD (n = 2), juvenile idiopathic arthritis (n = 1), ankylosing spondylitis (AS; n = 1), and psoriasis (n = 1).
At the time of diagnosis, 11/51 children (22%) were transitorily treated with glucocorticoids. MTX was prescribed in 9/51 children (18%) during the course of the disease. Except for 1 child with concomitant IBD, all children were treated with NSAID initially and as needed (Table 1).
Children with extended CNO were treated with pamidronate (Figure 1). Mean time from diagnosis to start of pamidronate treatment was 1.8 (0.9–3.6) months. The median duration of pamidronate treatment was 24 (22–27) months. Side effects of pamidronate were mild, transient, and typically only present during the first treatment series. Reported side effects were flu-like symptoms (11/32), headache (3/32), arthralgia (1/32), abdominal pain (1/32), and asymptomatic hypocalcemia (1/32). Pamidronate was discontinued in 1 child with high fever (40.5°C), but reintroduced 1 year later without side effects.
A TNF-α inhibitor was prescribed in 4/32 children (13%) with extended CNO and persisting inflammatory comorbidity (peripheral synovitis, n = 3, and IBD, n = 1) and in 10/32 children (31%) with persistent disease activity despite pamidronate treatment. Mean time from start of pamidronate to start/add-on of TNF-α inhibitors was 12 (10–25) months. Children with inflammatory comorbidity responded well to TNF-α inhibitors. In 7/14 children (50%) treated with TNF-α inhibitors, it was necessary to switch to a second TNF-α inhibitor. Three children changed to a third biological DMARD; TNF-α inhibitors in 2 cases and tocilizumab (interleukin 6 receptor antagonist) in the third case.
Spinal involvement was found in 2/19 children (11%) with limited CNO (Table 2). One boy was HLA-B27–positive with a family history of AS. He was treated with a TNF-α inhibitor. One boy was initially treated with glucocorticoids and continued taking MTX. Clinical and radiological evaluation showed a good treatment response.
Anatomical distribution of bone lesions in children with extended and limited chronic nonbacterial osteomyelitis (CNO).
Imaging
In children with extended CNO, a WB-MRI was performed after 1 and 2 years in 84% and 91% of cases, respectively. Local MRI was performed in children who did not have a WB-MRI. One child with extended CNO did not have followup MRI after 1 year.
At the time of diagnosis, the median number of radiologically active bone lesions in all children was 5 (2–8) lesions per patient (LPP; Table 1). The tibia was the most common anatomical site involved (47% of the children) followed by the femur (43%; Table 2).
Extended CNO
In extended CNO, a followup MRI was conducted after 1 year [median 12 (11–16) mos] and after 2 years [median 24 (22–26) mos]. The total number of radiologically active bone lesions declined over the first year from median 6 LPP (4–9) to 2 (0–7; p = 0.01). Radiological remission was achieved in 7/31 children (23%) after 1 year, but out of these children, 3/7 (43%) showed new radiologically active lesions after 2 years. After 2 years, 10/31 children (32%) were in radiological remission. A further reduction in number of radiologically active lesions from Year 1 to Year 2 was not detected. New radiologically active lesions developed in 19/31 children (61%) during the first year and in 17/31 (55%) during the second year (Figure 2). There was a trend toward a decreasing number of radiologically active bone lesions in the pelvis (p = 0.09) and at the sacroiliac joints (p = 0.06) and an increase of metatarsal lesions (p = 0.06).

Radiological disease activity in extended CNO (n = 32). Children categorized with extended CNO were treated with pamidronate. MRI was performed at time of diagnosis, and at years 1 and 2. A. Number of bone lesions per patient (LPP) was assessed at time of diagnosis, and at years 1 and 2. A significant reduction in number of bone lesions during Year 1 was found using the Wilcoxon signed-rank test, p = 0.04. B. Number of new bone lesions per patient (LPP) developed from time of diagnosis to Year 1, and from years 1 to 2. CNO: chronic nonbacterial osteomyelitis; MRI: magnetic resonance imaging.
Spinal lesions
Spinal lesions were seen in 13/51 children (25%; Table 2). Median number of spinal lesions was 3 (1–4), max. 9 LPP. Erosions of the vertebral plates were seen in 5/13 (38%). Spinal lesions were predominantly seen in the thoracic spine (86%) but also in the cervical (7%) and lumbar spine (7%). Two of the children with spinal involvement had spinal deformation, 1 with kyphosis and 1 with pronounced scoliosis. In children undergoing diagnostic WB-MRI, we detected asymptomatic spinal lesions in 2/39 (5%). In extended CNO, the number of spinal lesions was significantly reduced following the first year of pamidronate treatment (p = 0.01). New spinal lesions were detected in 2/32 children (6%) with extended CNO.
Clinical disease activity
In extended CNO, at Year 1, 12/32 children (38%) presented with clinically inactive disease while taking medication, but 5/12 children (42%) experienced clinical relapse at Year 2 and 8/12 (67%) had clinical relapse in the followup period (Figure 3). Relating radiological disease activity to clinical disease activity was not possible. The number of children presenting clinically inactive disease and radiologically active disease was 8/12 (67%) after 1 year and 10/14 (71%) after 2 years. Tapering medication in children with extended CNO often led to clinical relapse if persistent radiological activity was present.

{kind=link}
{kind=link}
{kind=link}
Clinical disease activity assessed from time of diagnosis to Year 7. Numbers above columns are the number of children assessed. A. Children with extended CNO were treated with pamidronate (n = 32). Median followup duration was 4 years (4–6). B. Children with limited CNO were not treated with pamidronate (n = 19). Median followup duration was 3 years (3–7). Lost to followup indicates children dropped from followup after having continuous clinically inactive disease while not taking medication. CNO: chronic nonbacterial osteomyelitis.
Among children with limited CNO, at Year 1, 10/19 (53%) presented with clinically inactive disease while taking medication. At Year 2, 10/16 children (63%) presented with clinically inactive disease while not taking medication and had no clinical relapse in the followup period (Figure 3).
The overall proportion of children with clinically active disease decreased during the followup period. However, at Year 5, second-line pharmaceuticals were still used in 8/14 children (57%) with extended CNO and in 3/8 children (38%) with limited CNO.
We recorded the following complications not related to inflammatory disease: chronic pain syndrome (persistent symptoms, no physician-reported sign of inflammation, normal ESR, and radiological remission; n = 4), symptoms of depression (n = 2), chronic abdominal pain (n = 1), and persistent headache (n = 1).
DISCUSSION
CNO can cause persistent pain, disability, and bone deformations. Our study suggests that early-onset treatment with pamidronate in children with extended CNO may improve the clinical course and radiological outcome.
Our study introduces a standardized 2-year pamidronate treatment regimen in patients with extended CNO. Previous studies have been reporting more than 2 years’ duration of symptoms before initiation of second-line treatment18,19,20. Improvement in clinical and radiological disease activity was found to be most pronounced in the first year, but with a continuously improving trend. However, in a fraction of the children, clinical relapse and new radiologically active bone lesions developed during the treatment. This indicates that CNO is an ongoing relapsing disease, and although pamidronate may be effective, we observed pamidronate failures and biologics were a necessary supplement to pamidronate to treat persisting active CNO and synovitis. Tapering medication in children with extended CNO often led to clinical relapse if children were still radiologically active.
It was not possible to predict radiological disease activity from the clinical disease activity. This confirms the findings described in a 12-month WB-MRI followup study by Beck, et al13. That study found that 41% of children with CNO showed radiological relapses, but 67% of them were clinically silent. Voit, et al8 conducted a longterm WB-MRI followup study of children with CNO (> 10 yrs). That study found that 24% of the children were radiologically active although presenting clinically inactive disease.
When scoring disease activity in our present retrospective study, only information regarding absence or presence of symptoms was available. Because data on physician’s global score and patient/parent-reported outcomes measures were not available, quantification of disease activity could not be recalled. Thus, the data were not sufficient to assess partial improvement or worsening of clinical disease activity. Use of the PedCNO (PedCNO30, PedCNO50, PedCNO70) score has been suggested in scoring disease activity in CNO in prospective studies12. PedCNO refers to a set of 5 outcome variables: ESR, number of radiological active bone lesions, severity of disease estimated by the physician, severity of disease estimated by patient or parent, and the Childhood Health Assessment Questionnaire13. Systematic recording of physician’s global and pain score might be helpful to recognize chronic disease not related to inflammation, such as chronic pain syndrome.
The anatomical distribution of bone lesions in our study confirms findings from previous studies3,6,29. Bone lesions in the spine, pelvis, and anterior chest wall link CNO to SAPHO syndrome and non-HLA-B27–related spondyloarthropathies2,4,30. We observed spinal lesions in 25% of all children with CNO. The number of radiologically active vertebral lesions was reduced following pamidronate treatment. This confirms previous findings of pamidronate response to spinal lesions in CNO19,27,31,32. Vertebral collapse is a known complication of CNO caused by osteolysis of the vertebral body30. We found that pamidronate treatment may induce resolution of spinal bone inflammation and may thereby prevent vertebral collapse. Pamidronate has also been shown effective in improving clinical outcome in AS33 and in SAPHO syndrome34,35.
However, pamidronate showed no antiinflammatory effects on synovitis. Oral pamidronate has been tested in placebo-controlled clinical trials to treat synovitis in rheumatoid arthritis (RA)36,37. Although 1 study reported improvement in RA disease activity and erosion score, this was not confirmed by subsequent studies. Our study suggests that children with CNO and synovitis not responding to synthetic DMARD may benefit from TNF-α inhibitors.
WB-MRI has been shown to be of superior specificity and sensitivity compared to other whole-body imaging tools such as radiograph series, whole-body bone scintigraphy, and 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) alone or as the functional component of FDG-PET/CT6,29,38,39. WB-MRI should encompass the entire body, but visualization of hands and elbows can be technically difficult. However, the feet always fit into the field of view and are a frequent site of involvement, occurring in 35% of the children. The spine should be visualized using sagittal STIR to assess active inflammation, and if necessary, also a T1-weighted sequence to assess structural changes.
Although children with CNO may initially present with involvement of single sites, new skeletal foci may occur during the course of disease. Radiological disease burden will not only depend on the number of active inflammatory bone lesions, but also on chronic structural inflammatory changes such as hyperostosis and osseous deformation, lesion size, and anatomic site. Zhao, et al have previously described an MRI grading system to score bone inflammation40. Further, Arnoldi, et al have suggested a radiological index score for CNO for standard reporting of WB-MRI in CNO41. This index score includes these radiological aspects and may also be valuable for radiological reporting of longitudinal changes in CNO.
In limited CNO, 53% of the children presented with clinically inactive disease while taking medication at Year 1 and 63% of the children presented with clinically inactive disease while not taking medication at Year 2. This indicates that limited CNO is often self-limiting and that children commonly experience only 1 acute attack, which can be sufficiently treated with NSAID. Children with extended CNO were more likely to be diagnosed using WB-MRI than children with limited disease. This may lead to underestimation of the actual number of bone lesions in limited CNO and thus the severity of CNO. Children categorized as having extended CNO at the time of diagnosis may have had a spontaneous clinical improvement and radiological resolution without pamidronate treatment. This might favor the treatment effects of pamidronate, and we interpret this as potential risk of bias and confounding by indication.
It was not possible retrospectively to assess the radiological activity in children with limited CNO, and a fraction of the children may have been radiologically active at followup although presenting with clinically inactive disease. Repeated imaging in limited CNO would have been a strength.
The following limitations of our study need to be considered. First, the definition of extended CNO is not validated and the treatment strategy reflects current treatment practice in our institution. Second, the study is a retrospective case series and the assessment of clinical data is based on medical records and imaging reports. Third, the distribution of bone lesions by MRI was interpreted from reports performed by pediatric radiologists and has not been assessed blinded to clinical information.
Our study introduces pamidronate treatment earlier in the disease course than previously suggested in CNO. We found that pamidronate might contribute to improving clinical and radiological disease activity in CNO. However, relapse was rather frequent. Persistent CNO should be treated and needs longterm followup to detect progressive disease. Further studies are needed to develop appropriate clinical and radiological outcome measures and to assess treatment response in an appropriate placebo-controlled study design.
Footnotes
Aarhus University has financially supported this work.
- Accepted for publication March 26, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.