
Abstract
Objective. Renal thrombotic microangiopathy (TMA) is an uncommon pathological finding in lupus nephritis (LN), and its clinical significance remains to be defined.
Methods. Twenty-four patients with lupus nephritis (LN) and renal TMA were selected from a retrospective review of 677 biopsy-proven LN patients, and compared with 48 LN controls without TMA (1:2 ratio) matched according to demographics and treatments.
Results. Renal TMA was noted in 3.5% of kidney biopsies of LN. TMA was associated with a higher prevalence of anti-Ro (45.8% vs 18.8%; p = 0.016), higher Systemic Lupus Erythematosus Disease Activity Index scores (21.4 ± 8.5 vs 10.8 ± 2.3; p < 0.001), lower estimated glomerular filtration rate (eGFR; 16.8 ± 11.7 ml/min vs 77.8 ± 28.6 ml/min; p < 0.001), and a higher percentage of patients who required dialysis (37.5% vs 2.1%; p < 0.001) at the time of kidney biopsy. Activity and chronicity indices [median (range)] were higher in the TMA group [11 (2–19) and 3 (1–8), respectively, compared with 7 (0–15) and 1 (0–3) in controls; p = 0.004 and p < 0.001; respectively]. Patients with TMA showed inferior 5-year renal survival and higher incidence of chronic kidney disease at last followup (70% and 66.6%, respectively, compared with 95% and 29.2% in controls; p = 0.023 and 0.002, respectively). The TMA group also showed lower median eGFR compared with controls [50.1 (IQR 7–132) ml/min vs 85.0 (IQR 12–147) ml/min; p = 0.003]. Five-year patient survival rate was similar between the 2 groups (87% and 98% in TMA and control group, respectively; p = 0.127).
Conclusion. TMA in kidney biopsy was associated with more severe clinical and histological activity, and significantly inferior longterm renal outcome in LN.
- LUPUS NEPHRITIS
- THROMBOTIC MICROANGIOPATHY
- OUTCOMES
Lupus nephritis (LN) is a severe organ involvement in systemic lupus erythematosus (SLE), and an important cause of chronic kidney disease (CKD) and mortality1,2. Histological confirmation of LN is based on the International Society of Nephrology and Renal Pathology Society (ISN/RPS) 2003 Classification, which largely focuses on glomerular lesions and recommends that renal vascular lesions be reported as separate entries3. Renal vascular lesions are recognized in LN and previous studies have suggested that inclusion of these pathological features in LN classification might have additional prognostic value4. Thrombotic microangiopathy (TMA) is an important renal vascular lesion characterized by endothelial cell swelling, lumen narrowing, or thrombi formation in the interlobular arteries, arterioles, and glomerular capillaries5. Renal TMA in LN may or may not be associated with thrombogenic autoantibodies such as lupus anticoagulant (LAC) or antiphospholipid antibodies (aPL)5. Renal TMA has been associated with unfavorable renal outcomes in classical hemolytic uremic syndrome (HUS) secondary to infections, atypical HUS due to complement cascade defects, thrombotic thrombocytopenic purpura (TTP), and malignant hypertension (HTN)6,7, but reported findings in patients with LN have been variable and inconclusive, likely attributed to the limited experience owing to small sample size4,8,9. The pathogenesis of LN is multifactorial involving both genetic and acquired abnormalities in immune-mediated inflammatory processes, and the disease manifestations and response to treatment vary considerably between patients and are subject to the effect of race and environmental factors2,10,11. Asian patients with SLE have a higher prevalence of LN, but data from some Asian populations show that treatment response and prognosis are favorable in most patients, provided that diagnosis is not delayed and treatment is administered before extensive irreversible renal damage1,12–18. One previous study from Taiwan reported the clinical characteristics and short-term patient survival data of systemic TMA in 25 SLE patients, with complete renal remission rate of 44%19. Another report from mainland China showed poor renal outcomes in LN patients with renal TMA, but the study population included patients with TTP, antiphospholipid syndrome, malignant HTN, and systemic sclerosis (SSc)9. While it is generally perceived that renal TMA is a significant finding, there is relatively little systematic analysis of renal TMA in patients on LN because of the low incidence, especially with regard to clinico-pathological correlations and longterm renal survival.
MATERIALS AND METHODS
We performed a retrospective study on patients with biopsy-proven LN from 2 centers, at Queen Mary Hospital, Hong Kong, and Peking Union Medical College Hospital, Beijing, China, respectively, to identify patients with features of TMA in the kidney biopsy that showed LN, and to examine the clinico-pathological associations and the outcomes of LN patients with renal TMA.
Patients
The case records and kidney biopsy slides of all patients with biopsy-proven LN who were under the care of the 2 centers during the period of January 2002 to December 2016 were reviewed. The diagnosis of SLE was according to the revised American College of Rheumatology classification20, and that of LN was according to the 1982 World Health Organization classification for LN until 2004, then the ISN/RPS 2003 classification afterward3. Kidney biopsies prior to 2004 were reviewed and reclassified according to the ISN/RPS 2003 classification. Patients with kidney biopsies showing both LN and renal TMA (as described below) were selected. Considering that patient and renal survival can be affected by patient demographics, duration of followup after kidney biopsy, class of LN, as well as induction and maintenance treatments, we reviewed all LN patients and selected non-TMA LN patient controls in 1:2 ratio according to the matching of these variables. Patients were excluded if they had chronic viral hepatitis infection, other concomitant autoimmune diseases, active malignancy, or pregnancy. Data retrieval and analysis was approved by the institutional review boards of the 2 institutes (approval no. UW11-115).
Assessment of renal histopathology
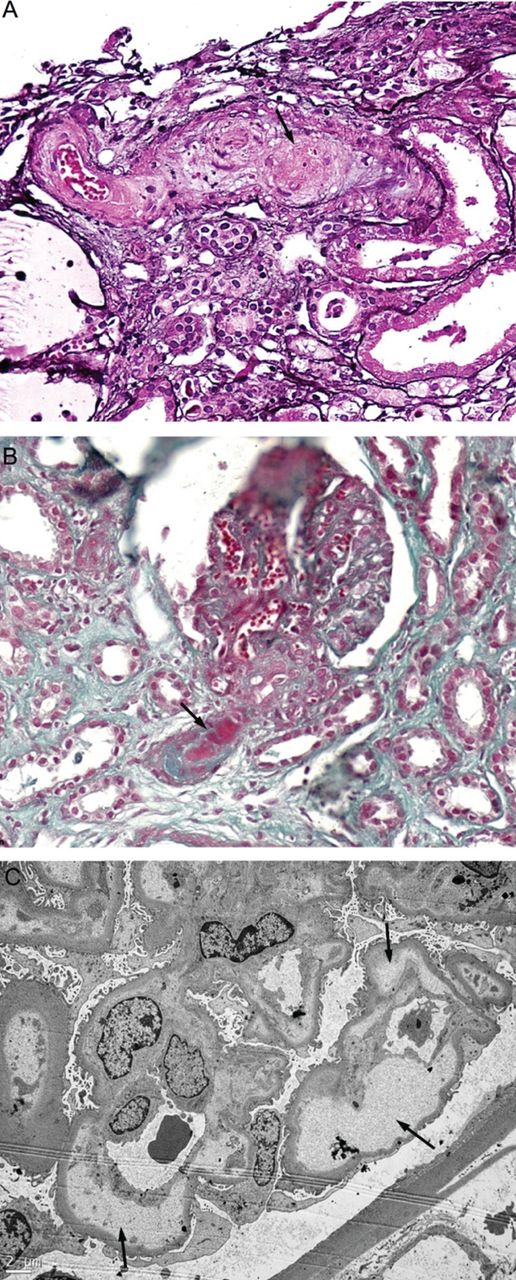
Renal biopsy specimens were examined with light microscopy, immunofluorescence, and electron microscopy by 2 independent pathologists, and reported according to the ISN/RPS 2003 classification. All histological findings were reevaluated and verified by a third independent renal pathologist at Queen Mary Hospital, Hong Kong. Renal TMA was defined as endothelial cell swelling, lumen narrowing or obliteration, and thrombi formation in interlobular artery, arteriole, and glomerular capillary lesions upon examination by light microscopy (Figure 1A and 1B) using H&E, silver, and Masson’s trichrome staining. Swelling of glomerular endothelial cells and their detachment from glomerular basement membrane and widening of the subendothelial space were confirmed by electron microscopy (Figure 1C).

Representative images of renal thrombotic microangiopathy characterized by (A) mucoid intimal thickening in an interlobular arteriole (arrow; silver stain, original magnification ×400); (B) thrombosis in an afferent arteriole (arrow; Masson’s trichrome, original magnification ×400); and (C) subendothelial space expansion (arrows) by subendothelial cells and flocculent material (electron micrograph, original magnification ×4000)
Immunosuppressive protocol and adjunctive therapies
Patients with active Class III/IV ± V LN were treated with prednisolone plus either cyclophosphamide (CYC) or mycophenolate mofetil (MMF; available since 1998) under standard induction and tapering protocols13. The period of induction referred to the first 6 months after the commencement of immunosuppressive treatments. Prednisolone was initiated at 0.8–1 mg/kg/day and tapered by 5 mg/day every fortnight to reach 5–7.5 mg/day after about 6 months. CYC was given orally at 1.5–2 mg/kg/day for 6 months. MMF was commenced at 1.5–2 g/day and the dose remained unchanged for 6 months if tolerated. Anti-CD20 therapy was not used. Plasmapheresis was used only in patients who showed clinical evidence of systemic TMA (as defined by the presence of thrombocytopenia and evidence of microangiopathic anemia). Maintenance immunosuppression comprised low-dose prednisolone (5–7.5 mg/day) and either azathioprine (AZA) or MMF. MMF dose was 1–1.5 g/day during the first 6 months of maintenance immunosuppression, and then gradually reduced according to clinical status. The dose of AZA was 2 mg/kg/day during the first 6 months of maintenance immunosuppression, and then gradually reduced according to clinical status. Subsequent rate of dose tapering for the immunosuppressive medications varied between patients depending on clinical stability and prior history of disease relapse. Hydroxychloroquine and renin-angiotensin blocking agents, as well as treatment of hypertension and dyslipidemia, were standard.
Followup schedule and outcome measures
Patients were seen at 2- to 14-week intervals depending on their clinical status. These variables were monitored at every visit: blood pressure, complete blood picture, renal and liver biochemistry, anti-dsDNA (measured by ELISA; BioRad), complement C3 levels (measured by nephelometry; Beckman Coulter), anti-Ro (detected by Ouchterlony double-gel immunodiffusion and Western blotting), aPL (measured by commercially available ELISA assays; QUANTA Lite), LAC (determined by dilute Russell’s viper venom test), proteinuria, and clinically significant events. Glucose and lipid profile were measured every 6 months. Complete renal remission (CR) was defined as reduction in urine protein excretion to < 0.5 g/day together with improved or stable renal function; the latter indicated by a serum creatinine level not higher than 115% of baseline value. Partial renal remission (PR) was denoted by a decrease in urine protein excretion by ≥ 50% and in the subnephrotic range, together with improved or stable renal function.
Statistical analysis
Continuous variables were expressed as mean (± SD) or median (range), and compared with Student t test or Mann-Whitney U test where appropriate. Categorical variables were expressed as frequency (percentage), and analyzed using chi-square test or Fisher’s exact test where appropriate. Patient and renal survival rates were estimated by Kaplan–Meier method. Risk factors for renal failure were analyzed by multivariate Cox regression analysis. All statistical analyses were performed by SPSS 24.0 (IBM Corp.), and p values of 0.05 (2-tailed) were considered statistically significant.
RESULTS
Patients and clinical characteristics
We reviewed a total of 677 patients with kidney biopsy showing LN and identified 26 cases with renal TMA. Two cases were excluded because the reevaluation of their histology did not show convincing evidence of renal TMA, and we did not identify additional TMA cases upon reevaluation of all kidney biopsies. Therefore, 24 patients (3.5%) showing renal TMA and 48 matched non-TMA controls were included in the analysis (Table 1). The duration of followup in TMA and non-TMA patients was 48.6 ± 31.5 months and 49.2 ± 23.8 months, respectively.
Clinical characteristics of lupus nephritis (LN) patients with or without renal thrombotic microangiopathy.
Patients with TMA showed a higher seroprevalence rate for anti-Ro antibodies (45.8%), compared with 18.8% in non-TMA controls (p = 0.016). There was no difference in the seroprevalence of anti-La, anticardiolipin antibodies, and LAC between the 2 groups (p > 0.05 for all). In addition, patients with renal TMA showed higher serum creatinine and lower eGFR levels at presentation (397.7 ± 192.4 μmol/l and 16.8 ± 11.7 ml/min, respectively) compared with non-TMA controls (94.4 ± 38.7 μmol/l and 77.8 ± 28.6 ml/min, respectively; p < 0.001 for both). More patients with renal TMA required acute hemodialysis at presentation of active nephritis compared to the non-TMA group (37.5% and 2.1%, respectively; p < 0.001). Renal TMA patients also had higher SLEDAI scores (21.4 ± 8.5, compared with 10.8 ± 2.3 in non-TMA controls). The TMA groups also showed lower C3 at presentation (40 ± 20 mg/dl, compared with 50 ± 20 mg/dl in non-TMA patients; p = 0.018), while the levels of anti-dsDNA antibodies were similar between the 2 groups (p = 0.387). LN patients with renal TMA also showed lower hemoglobin, leukocyte, and platelet counts compared with non-TMA controls (p < 0.001, 0.03, and < 0.001, respectively; Table 1).
Renal histopathological features
The median scores of activity index, leukocyte infiltration, fibrinoid necrosis/karyorrhexis, and interstitial infiltrates were higher in the renal TMA group compared with the non-TMA group (p = 0.004, 0.005, 0.011, and < 0.001, respectively; Table 2). The median scores of chronicity index, interstitial fibrosis, and tubular atrophy were also higher in the renal TMA group compared with non-TMA controls (p < 0.001 for all; Table 2). We did not identify any case with other features of SLE vasculopathy within the group of 24 patients with renal TMA and the 48 control patients included in this study.
Renal histological features in lupus nephritis (LN) patients with or without thrombotic microangiopathy on kidney biopsy.
Clinical outcomes
The short-term and longterm clinical outcomes were summarized (Table 3). LN patients with TMA achieved comparable CR rate compared with non-TMA controls (8.3% vs 6.3% and 25.0% vs 20.8%, at 6 and 12 months, respectively; p = 0.743 and 0.690, respectively). The TMA group had lower PR rate at 6 months compared with non-TMA controls (8.3% vs 29.2%; p = 0.045), but the difference at 12 months did not reach statistical significance (12.5% vs 33.3%, p = 0.07). Mean time-to-CR and time-to-PR in the TMA group was 11.8 ± 6.6 months and 8.2 ± 7.3 months, respectively, compared with 9.0 ± 5.0 months and 6.5 ± 5.6 months, respectively, in non-TMA patients (p = 0.28 and 0.55, respectively). Four patients suffered systemic TMA and all were treated with plasmapheresis. Their serum creatinine, eGFR, anti-dsDNA, C3, and SLEDAI score at presentation were 378.8 ± 226.2 μmol/l, 21.2 ± 17.4 ml/min/1.73m2, 180.0 ± 161.7 IU/ml, 36.3 ± 18.9 mg/dl, 24.0 ± 10.6, respectively (compared with 401.5 ± 191.4 μmol/l, 16.0 ± 10.6 ml/min/1.73m2, 114.5 ± 116.5 IU/ml, 35.0 ± 21.4 mg/dl, 20.9 ± 8.3, respectively, in patients not treated with plasmapheresis; p = 0.835, 0.431, 0.478, 0.909, and 0.52, respectively). Among the 4 patients treated with plasma-pheresis, one reached CR at 12 months, and there was no apparent effect of plasmapheresis on renal or patient survival.
Clinical outcomes of lupus nephritis patients with or without renal thrombotic microangiopathy (TMA).
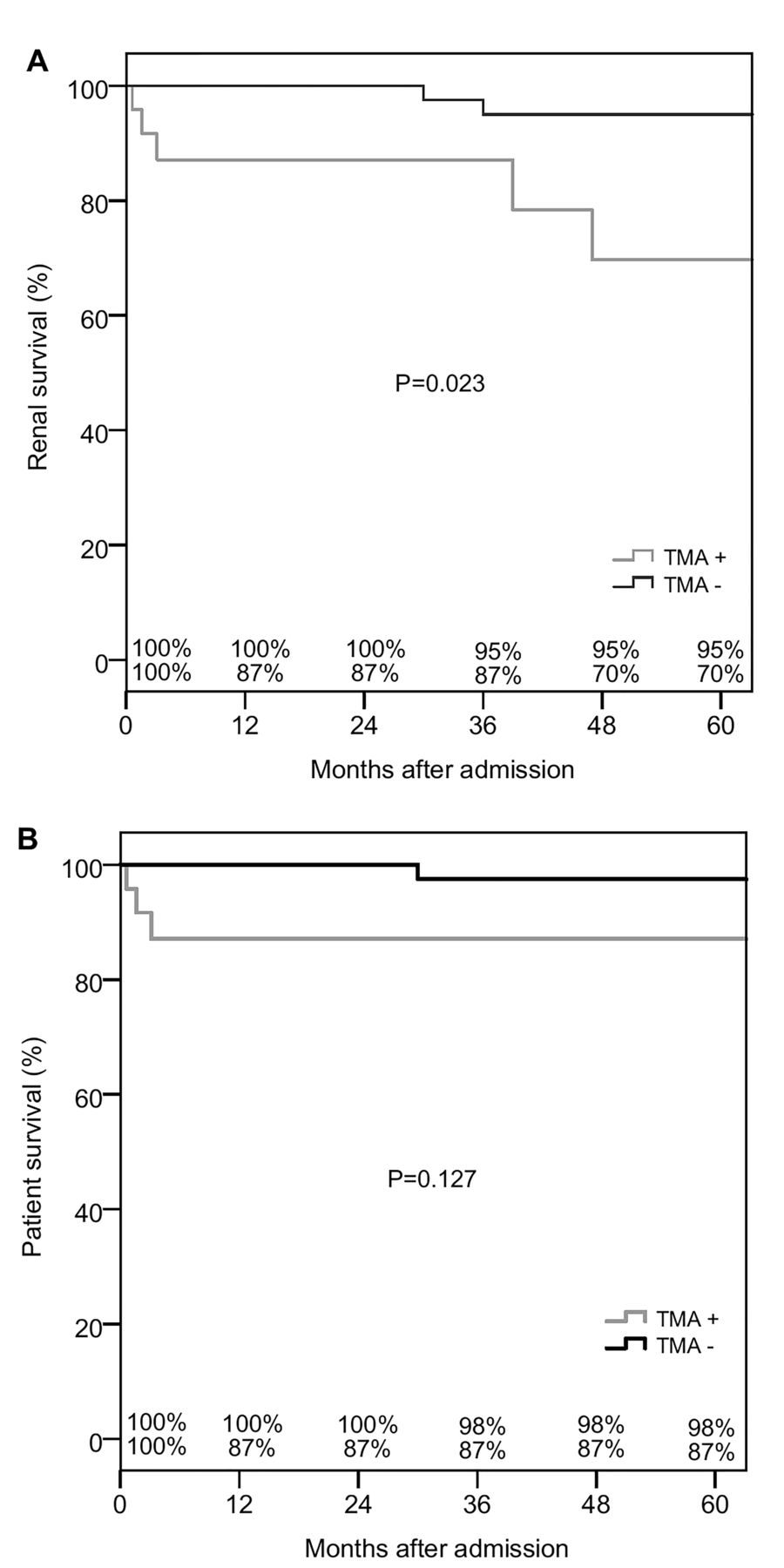
LN patients with renal TMA showed inferior renal survival rate and a higher occurrence rate of stage 3 or above CKD at last followup (70% at 5 yrs, and 66.6%, respectively, compared with 95%, and 29.2% in non-TMA controls; p = 0.023 and 0.002, respectively; Figure 2A). The TMA group also showed lower median eGFR value at last followup compared with non-TMA controls (50.1 ml/min, IQR 7–132 ml/min, vs 85.0 ml/min, IQR 12–147 ml/min; p = 0.003; Table 3). Univariate analyses showed that renal TMA (HR 9.702, 95% CI 1.596–58.96; p = 0.014) and histological activity (HR 1.183, 95% CI 1.004–1.394; p = 0.044) were risk factors for renal failure but not chronicity and SLEDAI score at presentation (HR 1.245 and 1.046, 95% CI 0.917–1.690 and 0.981–1.116, respectively; p = 0.161 and 0.169, respectively). Multivariate analyses further demonstrated that only renal TMA was an independent risk factor for renal failure (HR 7.164, 95% CI 1.077–47.64; p = 0.042) after adjusting for histological activity and chronicity, and SLEDAI scores at presentation. Anti-dsDNA titer at presentation and serum creatinine at 1 year showed inverse relationships with renal survival during followup in the TMA group (r = −0.628 and −0.540, respectively; p = 0.001 and 0.006), but not in non-TMA patients (r = −0.121 and −0.265 respectively; p = 0.541 and 0.086). Renal survival during followup was not associated with age, sex, induction, or maintenance immunosuppressive regimen, serum creatinine, proteinuria, C3 level, anti-Ro seropositivity, activity index, chronicity index, hemoglobin level, leukocyte and platelet counts, and SLEDAI at presentation (p > 0.05 for all). Three patients with renal TMA died during followup: 2 of pneumonia and 1 from serial complications following thrombocytopenia-associated bleeding after renal biopsy. Two patients without renal TMA died, one because of myocardial infarction and the other from dialysis-related peritonitis. Patient survival rate after 5 years was similar between renal TMA and non-TMA patients (87% and 98%, respectively; p = 0.127; Figure 2B).

{kind=link}
{kind=link}
(A) Renal and (B) patient survival rates of lupus nephritis patients with or without renal thrombotic microangiopathy (TMA).
DISCUSSION
Renal TMA is associated with unfavorable short- and longterm renal outcomes in patients presented with classical and atypical HUS, TTP, and hypertensive crisis6. LN is an important cause of acute kidney injury and CKD in Asia1,11, but there are few data on the prevalence of renal TMA and its effect on clinical outcomes. Renal TMA features have been reported in 0.5–9% of Japanese and white patients with LN, and up to 24% in a report from China9,21,22,23,24. In our retrospective study we included a big sample size of 677 patients with biopsy-proven LN, and the results show that renal TMA is relatively uncommon, occurring at a prevalence of about 3.5%. Though uncommon, the data show that the detection of renal TMA is of clinical significance, because it is associated with more severe disease and histological evidence of kidney injury at presentation, and also portends a less favorable longterm renal prognosis. A retrospective study from China had reported more aggressive renal presentation in LN patients with TMA9, but had included patients with antiphospholipid syndrome, malignant HTN, and SSc with heterogeneous management, and thus the effect of renal TMA on longterm outcomes in LN patients could not be discerned. In our present study we included LN patients (with the renal TMA features confirmed by a third-party pathologist) and non-TMA LN patients matched for important clinical and treatment characteristics as controls in the analysis of longterm clinical outcomes. Our finding of a higher requirement for acute hemodialysis at presentation was not reported in other series. The higher rate of anti-Ro seropositivity (45%) in the TMA group in our series, compared with non-TMA controls (18%) and also the data from an earlier report, is intriguing25. Further studies are required for reconfirmation and to investigate whether this is of pathogenic significance. In this context, a study in Mexico reported that 39% of LN patients with TMA were seropositive for anti-Ro8. Associations between anti-Ro antibodies and cutaneous vasculitis, TTP, renal involvement, and pulmonary HTN in SLE have been reported25,26,27. The relationship between anti-Ro antibodies and TMA, however, remains poorly understood, and the putative effects of anti-Ro on endothelial cells (e.g., accelerated endothelial cell apoptosis with increased vascular intimal thickness) might have contributed to the increased risk of TMA28,29,30.
Our current data demonstrated that LN patients with renal TMA showed inferior longterm renal prognosis compared with non-TMA patients despite the similar initial short-term response rates. The data suggest that this is likely related to the more severe chronic renal damage already present at baseline in TMA patients, since the 2 groups did not differ in their subsequent renal flare rates (data not shown), as we and others have highlighted the adverse effect of renal flares on longterm renal survival31,32,33,34,35. In our current study, LN patients with renal TMA had a renal survival rate of 70% after 5 years, which may appear non-inferior or more favorable than the results from other investigators6,7,8, but is clearly inferior to the renal prognosis that we reported previously1. The association between longterm renal outcome and serum creatinine at 1 month not only underscores the importance of early diagnosis and prompt initiation of effective induction treatment, but also provides a useful prognostic tool that could prompt thorough reassessment of the adequacy of response, including a repeat kidney biopsy, if deemed necessary. The limited experience with plasmapheresis, given in highly selected patients, does not allow drawing conclusions on its effect. The limitations of this study include its retrospective features and the different healthcare settings of the 2 centers. Notwithstanding, our data were derived from a big series of 677 biopsy-proven LN cases and the histological features were independently reevaluated by a third-party pathologist, and thus should represent a fairly accurate real-world experience of this uncommon condition, providing clinically important information to clinicians.
Renal TMA is an uncommon finding in LN but is associated with more severe clinical and histopathological renal disease, and inferior longterm renal outcomes.
- Accepted for publication February 13, 2019.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.