
Abstract
Objective. Diffuse idiopathic skeletal hyperostosis (DISH) is characterized by flowing bony bridges on the right side of the spine. Knowledge of the development of these spinal bridges is limited. The current longitudinal computed tomography (CT) study was designed to bridge this gap.
Methods. Chest CT scans from elderly males with 2 scans (interval ≥ 2.5 yrs) were retrospectively included. Using the Resnick criteria, a pre-DISH group and a definite DISH group were identified. A scoring system based on the completeness of a bone bridge (score 0–3), extent of fluency, and location of the new bone was created to evaluate the progression of bone formation.
Results. In total, 145 of 1367 subjects were allocated to the DISH groups with a mean followup period of 5 years. Overall prevalence of a complete bone bridge increased in the pre-DISH group (11.3% to 31.0%) and in the definite DISH group (45.0% to 55.8%). The mean bridge score increased significantly in both the pre-DISH and definite DISH group (p < 0.001). The new bone gradually became more flowing and expanded circumferentially.
Conclusion. Over the mean course of 5 years, the new bone developed from incomplete, pointy bone bridges to more flowing complete bridges. This suggests an ongoing and measurable bone-forming process that continues to progress, also in established cases of DISH.
- DIFFUSE IDIOPATHIC SKELETAL HYPEROSTOSIS
- BONE
- SPINE
- SPIRAL COMPUTED TOMOGRAPHY
Diffuse idiopathic skeletal hyperostosis (DISH) is a mainly radiological diagnosis defined as the presence of flowing ossifications on the anterolateral side of the thoracic spine and is associated with ossification of peripheral entheses such as the tendinous insertions of olecranon, pelvis, patella, and calcaneus (Figure 1)1. In subjects with DISH, clinically significant symptoms such as back pain, reduced range of motion around affected joints, dysphagia, airway obstruction, and reduced lung capacity can occur1,2,3. Further, individuals with DISH have a 4-fold risk of spine fractures, with more unstable fracture patterns and a considerably inferior clinical outcome in comparison to subjects without an ankylotic spine4,5. The most commonly used definition of DISH comprises 3 diagnostic criteria, proposed by Resnick and Niwayama, obtained with conventional radiographic (CR) imaging6. They used the presence of bridging hyperostosis over at least 4 contiguous vertebral bodies, without significant changes in the intervertebral disc height and absence of ankylosis of the facet and sacroiliac joints, to identify definite cases of DISH6. The prevalence of DISH ranges between 2.9% and 42.0% depending on the diagnostic criteria used and demographics of the population analyzed1,7,8,9. Independently of the criteria used, the prevalence of DISH rose with age in previously published studies7,8,9. DISH is associated with obesity, diabetes mellitus, and cardiovascular events, all of which are increasing in the world population, suggesting that the prevalence of DISH might also increase10,11,12. Molecular signaling pathways such as Wingless, nuclear factor-κB, and bone morphogenetic have been suggested to be involved in the formation of new bone in DISH, but at present there is a dearth of solid evidence on the pathogenesis of DISH1.
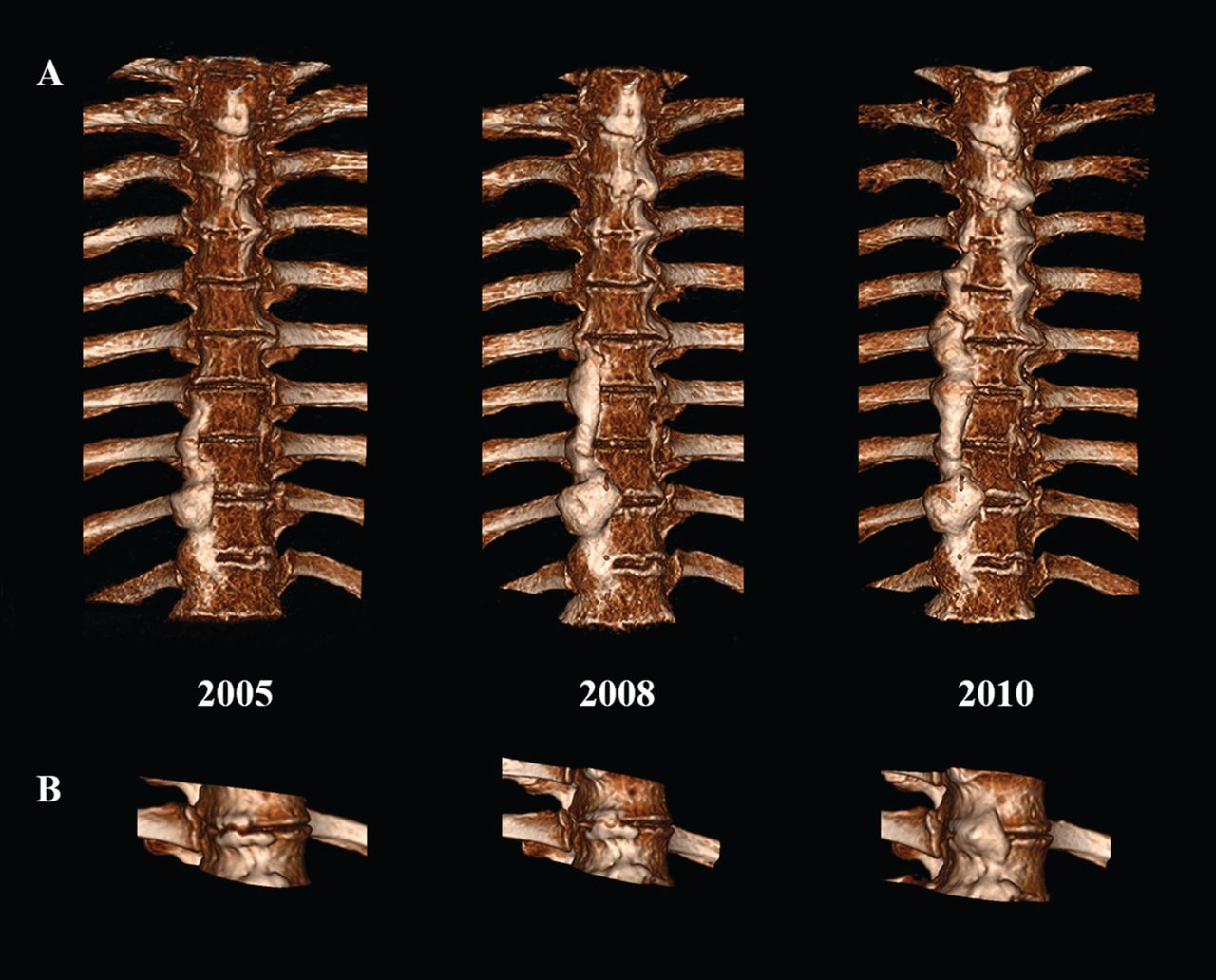
Three-dimensional reconstruction of thoracic computed tomography scans demonstrating the progressive ossification in DISH. A. The 3 reconstructed scans (T2–T11) show the increase in hyperostosis over time in a man from age 60 to 65. The subject was placed in the group with definite DISH, based on the presence of at least 3 contiguous bridges in both scans in 2005 and 2010. B. The stages of the developing new bone bridge are shown in a single segment (T8–T9) in a man from age 67 to 72. The bridge was incomplete in 2005 and scored as osteophytes ≥ 2 mm between the bony structures. In 2008 the osteophytes were almost in contact and in 2010 the bridge was completely fused. DISH: diffuse idiopathic skeletal hyperostosis.
Currently, the most frequently used criteria for DISH are dichotomous (presence of DISH yes/no), despite the growth of bone being an ongoing process13,14. To gain more insight into the early stages and pathogenesis of DISH, information on the natural course of the development and progression of DISH is necessary. We hypothesize that not only the formation of a bone bridge is a continuous process, as shown by Yaniv, et al, but also the fluency of the new bone formation and the circumferential bone size will likely increase over time15. Further, after fulfillment of the criteria by Resnick and Niwayama, bone will likely continue to form and remodel; however, clear data on this specific group are lacking. For this reason, a retrospective longitudinal study was performed using a new extended classification system to identify morphological changes on computed tomography (CT) scans of the thoracic spine of subjects with (pre-)DISH.
MATERIALS AND METHODS
Chest CT scans were extracted from our Picture Archiving and Communication Systems (PACS IDS7, 17.3, Sectra AB) and analyzed anonymously in an in-house built viewer (IX Viewer, Image Science Institute). This retrospective anonymous research does not require informed consent of the subjects in our country and permission for our study was granted by the institutional review board (correspondence number #17/164).
Collection of CT scans
Inclusion criteria were male sex (because that is associated with higher incidence of DISH9), the availability of a minimum of 2 chest CT scans obtained between 2004 and 2011, and with an interval of at least 2.5 years (to ensure change over time in this slow progressive disease15). Exclusion criteria were age under 50 years at the time of the first scan and poor CT scan quality. The CT scans were obtained with 16-64 detector CT scanners (Philips Medical Systems). The scans were acquired with a variety of protocols, but all CT scans were of acceptable quality and were stored as axial reconstructions in a slice thickness below 1 mm.
Identification of groups
First, for each subject the most recent CT scan in the longitudinal set was analyzed for the presence of DISH by 2 independent observers. Disagreement on the diagnosis was solved in a consensus meeting between the observers. DISH was established according to the Resnick and Niwayama criteria with careful assessment of fusion of the apophyseal joints to differentiate between DISH and ankylosing spondylitis (AS) because images of the sacroiliac joints, normally used for this differentiation, were not available6. All subjects without signs of DISH in the last CT scan were excluded from further analysis. If DISH was confirmed at the last scan, the first scan was subsequently similarly evaluated for the presence of DISH. This resulted in 2 groups: (1) a group with “pre-DISH,” consisting of subjects without DISH on the first CT, but with DISH on the last CT; and (2) a group with “definite DISH,” with DISH on both the first and the last CT.
CT evaluation
Strict criteria were defined to identify the morphological changes between the first and last scan. Changes observed in a pilot study of 10 randomly selected subjects from the group with pre-DISH in combination with data from previous articles describing a classification system for DISH were used to propose 3 characteristic DISH variables on CT15,16: (1) the presence and completeness of a bony bridge between the cranial and caudal vertebral bodies (bridge score); (2) the fluency of the new bone formation between the cranial and caudal vertebral bodies (flow score); and (3) the circumferential extent of the new bone formation in relation to the intervertebral disc and cranial and caudal vertebral bodies in the axial view (Figure 2 and Figure 3). All levels included on the CT scans were assessed segment by segment (i.e., 2 vertebral bodies with their intervertebral disc). The presence and completeness of a bone bridge could be scored in the sagittal and coronal plane as 0 = no bridge, 1 = osteophytes with ≥ 2 mm distance between 2 bony structures, 2 = osteophytes with < 2 mm distance between 2 bony structures or connected in a maximum of 2 sagittal/coronal CT slices, or 3 = completely fused bone bridge (slice thickness 1 mm; Figure 2). A loose calcified particle not connected to an incomplete bone bridge was noted in the pilot study and was also described in the scoring system by Yaniv, et al15. The role of these loose particles remains unknown and because the new bone formation was not completely fused, the presence of these calcifications was scored as a 1.

Computed tomography (CT) and artist drawings as examples of the presence and completeness of a bone bridge and the degree of flow of the hyperostosis. The presence and completeness of a bridge was scored as 0 = no bridge; 1 = osteophytes with ≥ 2 mm between 2 bone structures or presence of a loose calcified particle between the 2 vertebral bodies anterior of the intervertebral disc; 2 = osteophytes with < 2 mm between 2 bone structures or connected in maximum of 2 CT slices; 3 = completely fused bone bridge in more than 2 CT slices (slice thickness 1 mm). The degree of flow was scored as 1 = sharp angle of the hyperostosis; 2 = ambiguous sharp/blunt angle of the hyperostosis; 3 = flowing wide angle of the hyperostosis.
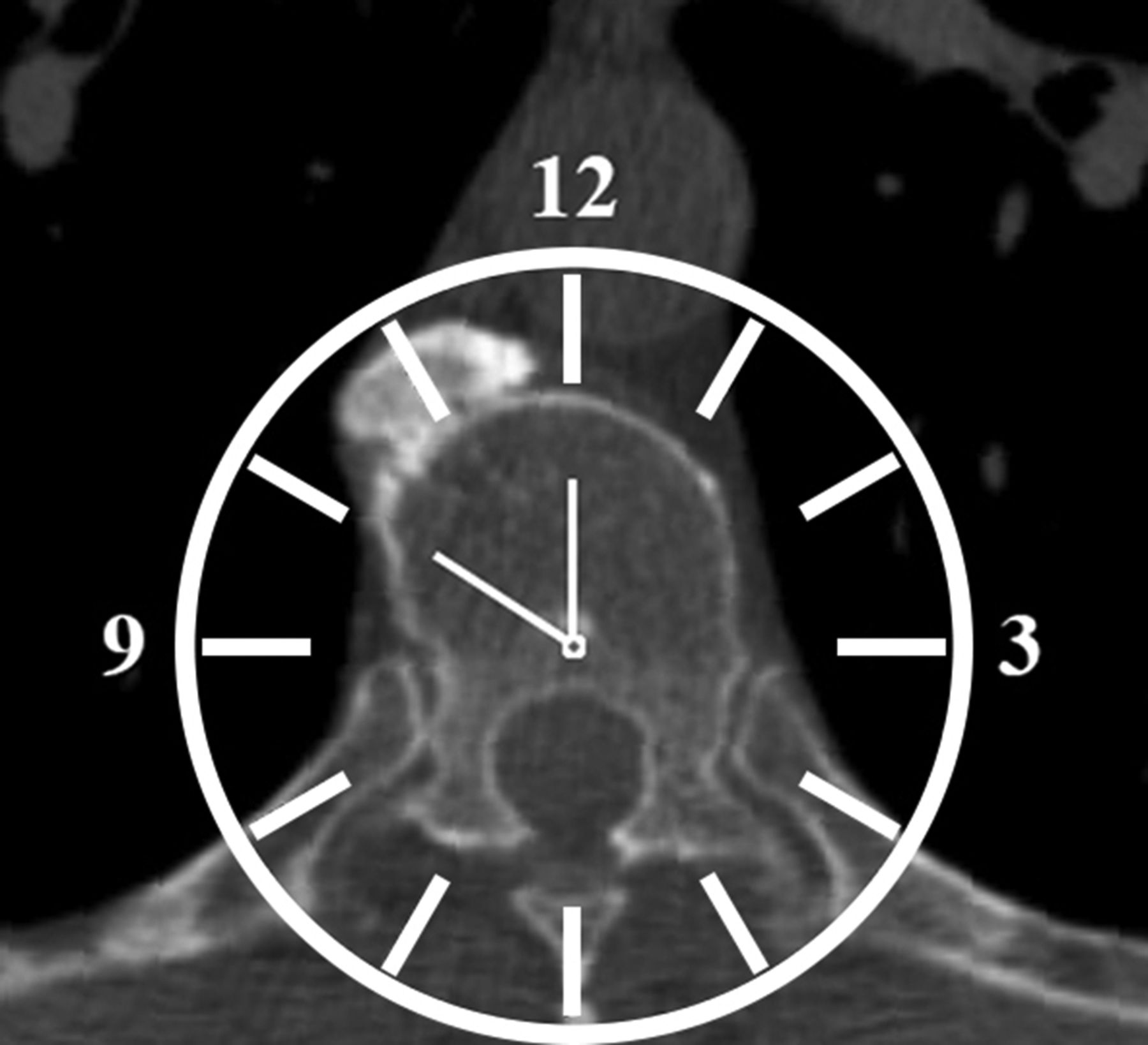
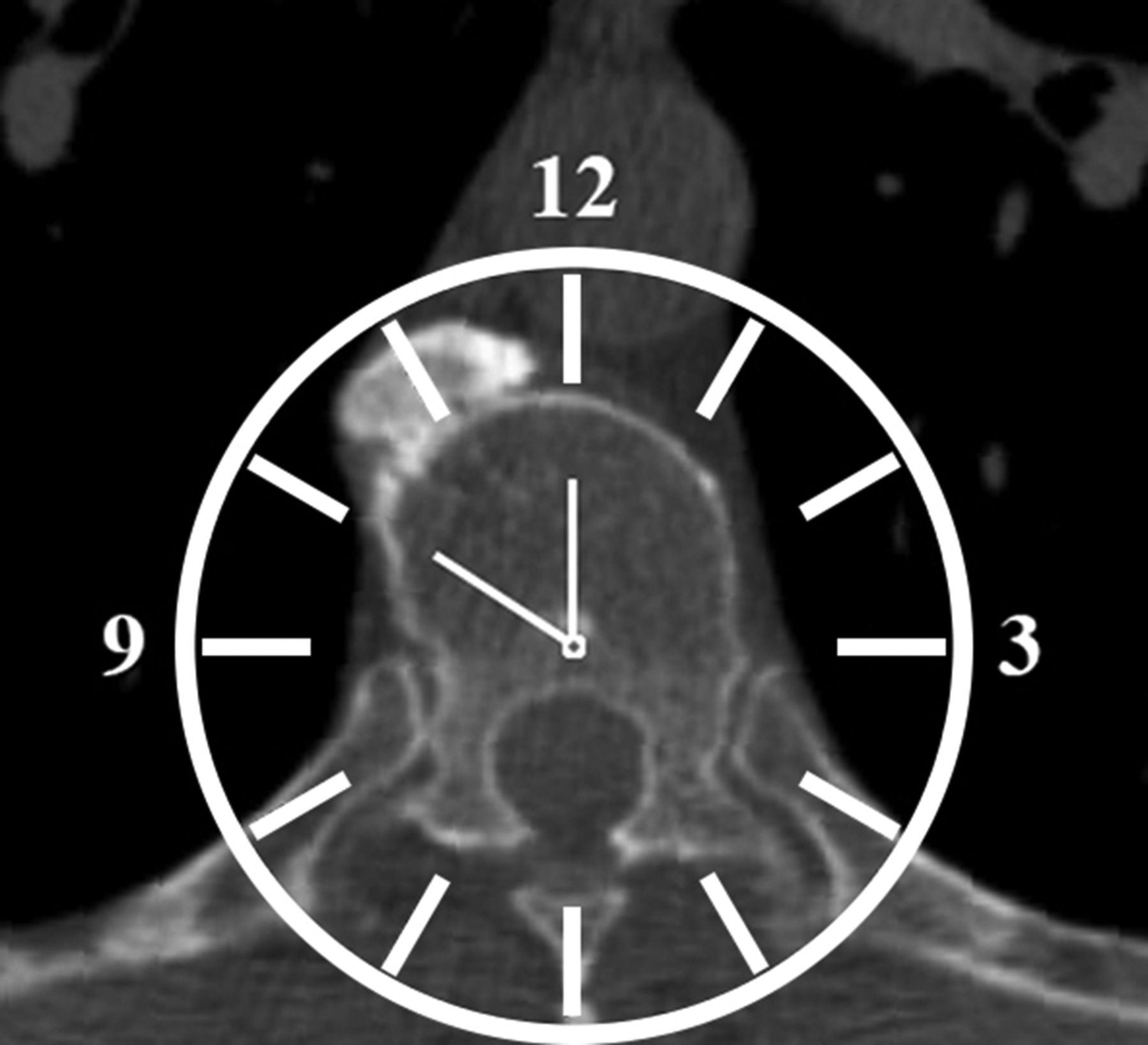
Axial computed tomography image with analog clock overlay to evaluate the circumferential extent of the ossification by pointing the clock hands to the extremes of the newly formed bone. The clock overlay was used at every segment with new bone formation. The 3- and 9-h marks were aligned with the anterior boundary of the costovertebral joints. The clock hands were placed at the extremes of the new bone formation — in this specific example, at the 10- and 12-h marks, away from the aorta (hour marks 11.5 to 13).
The degree of flow was evaluated in the sagittal and coronal plane and scored as 1 = sharp angle of the hyperostosis, 2 = ambiguous sharp/blunt angle of the hyperostosis, or 3 = flowing wide angle of the hyperostosis (Figure 2).
To describe the circumferential location of the bone in the axial view, an analog clock overlay was used with the 3- and 9- h marks aligning the anterior boundary of the costovertebral joints, resulting in the 12-h mark being midsagittal at the ventral top of the vertebral body (Figure 3). The location of new bone in the axial plane was scored with a projection of multiple slices (adjusted slice thickness 8–10 mm), including the intervertebral disc and both endplates of the adjacent vertebral bodies. The extent of the circumferential ossification was described by drawing in clock hands at the extremes of the newly formed bone using half an hour precision (Figure 3).
Two observers used these newly developed measurements to independently score a random sample of 25 CT scans from the pre-DISH group at random timepoints to test interobserver reliability. All CT scans from both groups were subsequently blinded for scan date (i.e., first or last) and scored by a single observer.
Statistical analyses
All data analyses were performed using R statistical software (R version 3.3.2, R Foundation for Statistical Computing). The interobserver reliability was calculated using intraclass correlation coefficients measuring interrater consistency and agreement per scoring measure using the irr package version 0.8417. The distribution of the 4 scoring outcomes for the presence and completeness of a bone bridge and degree of flow were calculated per subject. The mean bridge and flow score per subject was compared between the first and last timepoint using a paired t test in both the pre-DISH and definite DISH group after careful assessment of the distribution of the data using histograms, the Shapiro-Wilk test, and Q-Q plots. The extent of the circumferential new bone formation was compared between the 2 timepoints also using a paired t test per group. Posthoc sample size testing was performed for the paired data using the pwr package version 1.2-118.
RESULTS
The search in PACS yielded 1367 subjects (mean age 60.0 yrs at the first scan, ± 5.6) with at least 2 CT scans with a mean interval of 5.0 years (range 2.5–7.4) between the first and last scan. The CT scans were obtained for various reasons not related to clinical complaints associated with DISH. After assessment for the presence of DISH using the Resnick and Niwayama criteria on all scans, a total of 55 subjects (mean age 62.2 yrs, ± 5.8) were allocated to the pre-DISH group and 90 subjects (mean age 63.2 yrs, ± 6.3; p = 0.347) to the definite DISH group6. The overall prevalence of DISH was 6.6% at the first CT scan and 10.6% at the last CT scan. The levels C7 to L1 were selected for further analyses because these levels were present on both CT scans in more than 60% of the cases per group. The levels T2 to T11 were present on all CT scans. In the pre-DISH group, segment C7–T1 was visible in 69%, segment T1–T2 in 92%, segment T11–12 in 94%, and segment T12–L1 in 78% in the first and last CT scan of the cases. In the definite DISH group, segment C7–T1 was visible in 87%, segment T1–T2 in 100%, segment T11–12 in 93%, and segment T12–L1 in 62% in the first and last CT scan of the cases. The interrater reliability and agreement was calculated per scoring measure based on 318 segments in 25 CT scans and ranged from 0.6 to 0.9, corresponding to a moderate to good reliability and agreement (Table 1).
Results of interrater reliability using the intraclass correlation coefficient for a 2-way model based on the outcomes of 2 independent observers using the new scoring system on 25 CT scans (318 segments).
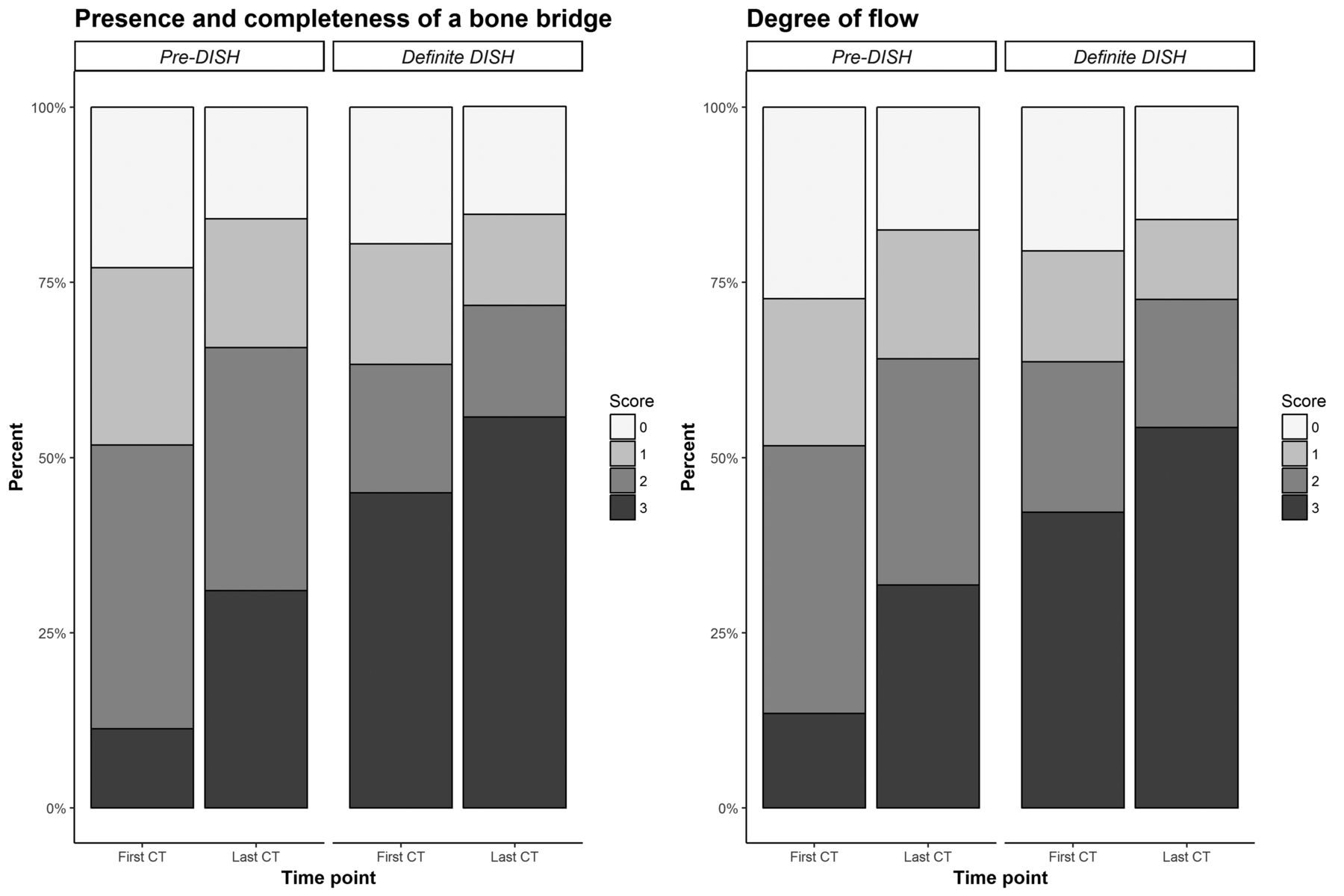
The overall distribution of the 4 scoring outcomes for the presence and completeness of a bone bridge and the degree of flow are presented in Figure 4. In the group with pre-DISH, the overall mean prevalence of segments with a complete bone bridge increased from 11.3% (77/681 segments) to 31.0% (209/674 segments) between the first and last scan. The mean prevalence of segments with bridge scores 0, 1, or 2 decreased. The mean bridge scores of all included segments increased significantly from 1.4 at the first scan to 1.8 at the last scan (p < 0.001, 95% CI 0.34–0.49). In the group with definite DISH, the same development occurred and the mean prevalence of segments with a complete bone bridge increased from 45.0% (513/1140 segments) to 55.8% (635/1139 segments; Figure 4). The mean bridge score increased from 1.9 at the first scan to 2.1 at the last scan (p < 0.001, 95% CI 0.15–0.32).
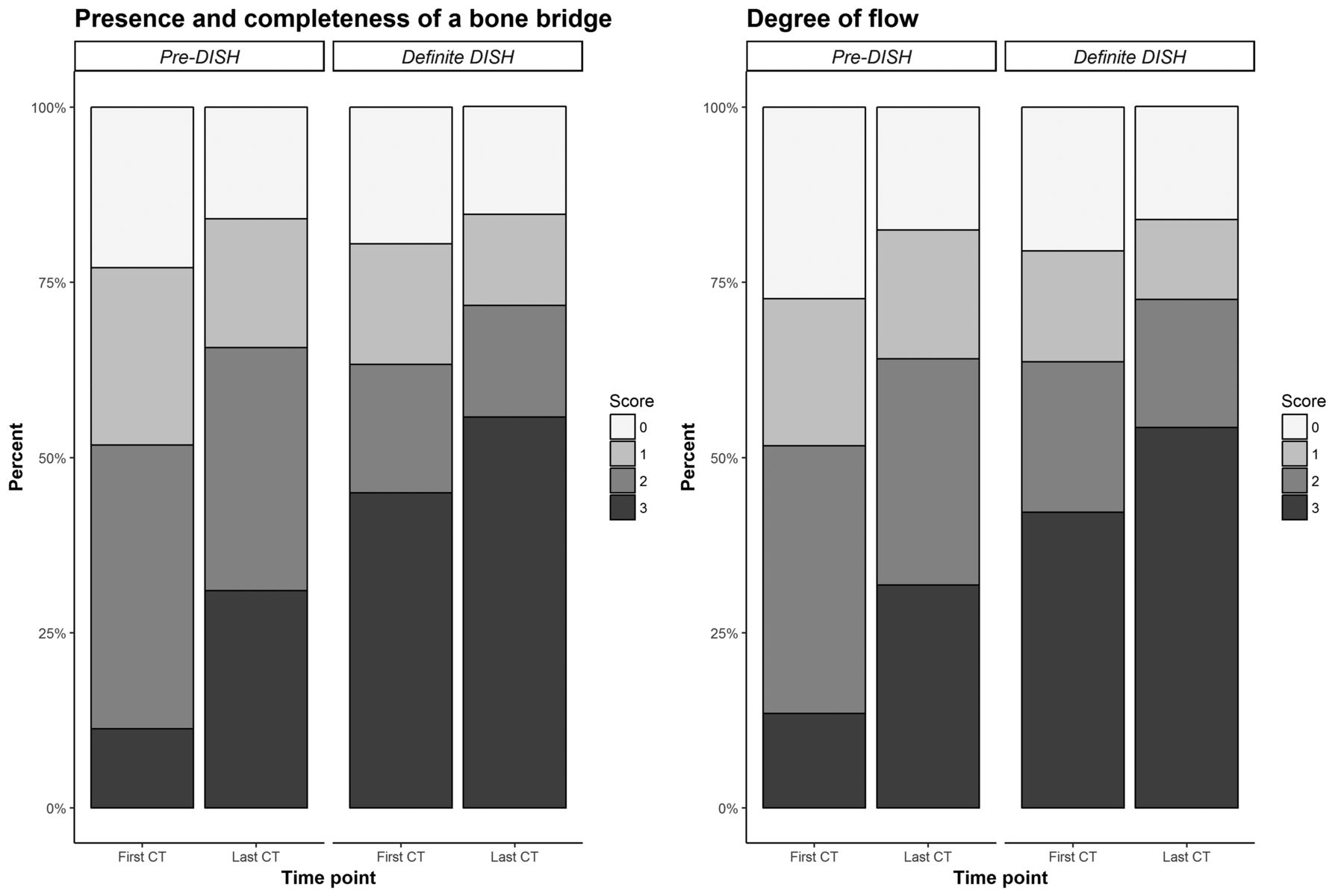
Results of the scoring system for the measures “presence and completeness of a bone bridge” and “degree of flow”. In the graphs, the distribution of the 4 different scoring outcomes is presented for segments C7–T1 to T12–L1 in both groups at the first and last timepoint. A clear increase in score 3, “completely fused bone bridge” (left graph) and “flowing wide angle of the hyperostosis” (right graph), was present in both groups. The scores 0, 1, and 2 all decreased over time. The scoring was performed per segment and not in a consecutive order, thus explaining the high prevalence of score 3 in not only the definite DISH group, but also the pre-DISH group. DISH: diffuse idiopathic skeletal hyperostosis; CT: computed tomography.
The prevalence of a flowing wide angle increased from 13.5% (92/681 segments) to 31.8% (214/674 segments) in the pre-DISH group and from 42.2% (481/1140 segments) to 54.3% (618/1139 segments) in the definite DISH group (Figure 4). The sharp angle and ambiguous sharp/blunt angles scores decreased over time in both groups. The mean flow score increased in the group with pre-DISH from 1.4 at the first CT to 1.8 at the last CT (p < 0.001, 95% CI 0.31–0.51) and from 1.9 to 2.1 (p < 0.001, 95% CI 0.17–0.34) in the group with definite DISH.
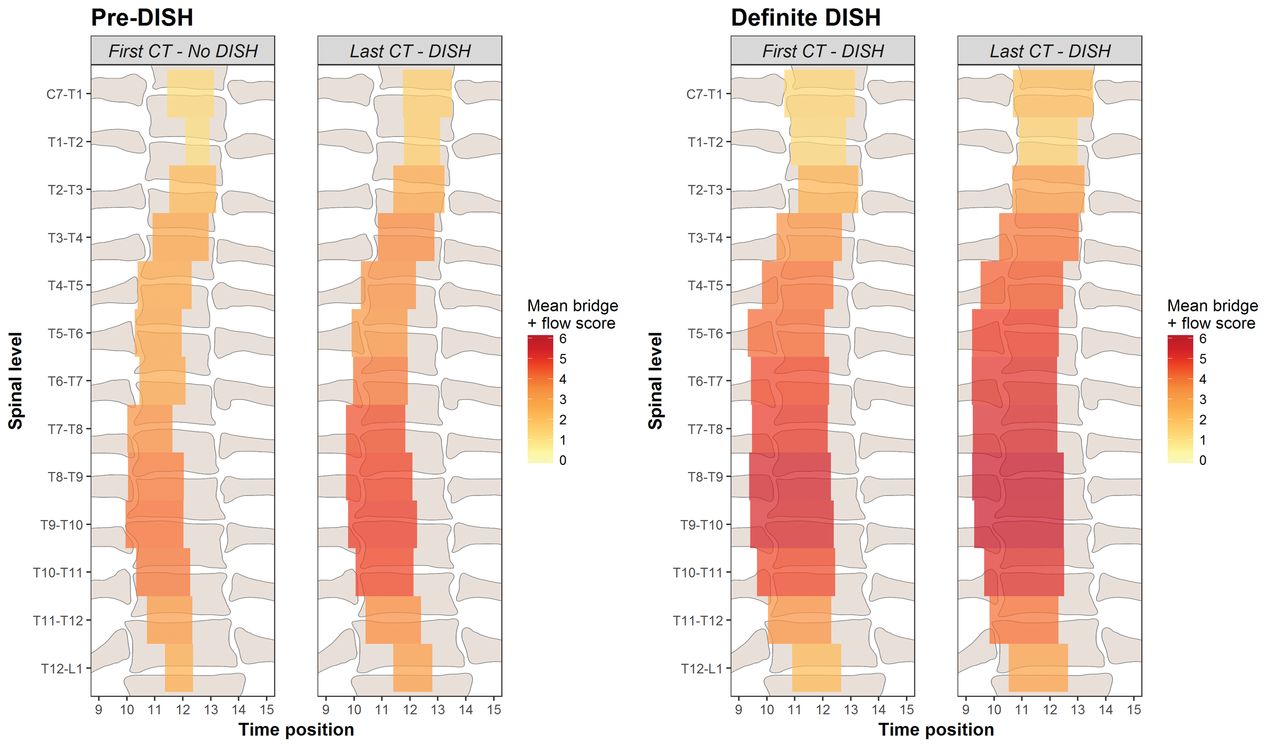
The center of the newly formed bone at the levels T3 to T12 was in both groups located on average between the 9 and 12-h mark of the clock overlay, indicating an asymmetrical formation of the bone mass toward the right side of the spine (Figure 5). For the segments C7–T1, T1–T2, T2–T3, and T12–L1, the center of the new bone approximated the 12-h mark of the clock. The mean extent of the circumferential hyperostosis increased over time at every segment with an overall mean of 1.7 h at the first scan and 2.0 h at the last scan in the pre-DISH group (p < 0.001, 95% CI 0.15–0.42) and 2.5 h and 2.8 h in the definite DISH group (p < 0.001, 95% CI 0.19–0.42). The posthoc power calculation of all paired t tests performed showed adequate power (n = 6 to 28 pairs).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Visualization of the results using the new scoring system in subjects with pre-DISH or definite DISH. The graphs show the mean circumferential extent of the new bone formation using the clock overlay per segment. The color of each segment was based upon the mean score of the bridge and flow score combined with the darker red color, indicating a more flowing complete bridge. The new bone extent was shifted to the right side at segments T3–T4 to T11–T12. In both groups, an increase in all 3 scoring measures was present, demonstrating the progressive character of DISH. DISH: diffuse idiopathic skeletal hyperostosis; CT: computed tomography.
A visual representation of the extent of newly formed bone for the pre-DISH and definite DISH group at the first and last scan is presented in Figure 5. The score on the presence and completeness of a bridge and the degree of flow were combined in this illustration because of their high correlation (Pearson correlation coefficient 0.96; p < 0.001, 95% CI 0.95–0.97), and our presumption that both the bridge score and the flow score reflect progression of the DISH ossification process. Segments T8–T9 and T9–T10 had the most complete and most fluent bridging with the largest circumferential extent of the new bone formation in both the pre-DISH and definite DISH group.
DISCUSSION
In our current study, morphological changes of DISH were investigated over a mean followup period of 5 years in subjects with pre-DISH and subjects with definite DISH using chest CT scans. The amount of newly formed bone in spinal DISH increases consistently over time and has been clearly visualized using the newly developed scoring system on CT. The new bone formation appears to start with bony outgrowths of the upper and lower vertebral body, and over time these outgrowths connect and subsequently remodel to form complete and rounded bridges. The visual characteristics of the bridging ossifications evolved from a sharp angle to a blunt angle and finally to a fully flowing form, while becoming broader in the axial plane.
The newly formed bone mass was evidently located more to the right side of the thoracic spine for the segments T3 to T12. The location of the new bone formation in DISH is assumed to be limited by the presence and/or pulsations of large vessels such as the left-sided aorta in the thoracic region19. Our results confirmed this finding, although the circumferential bone growth was extending equally in both the left and right direction over time (Figure 5). The new bone formation was less extensive in the anterior direction at the location of the aorta compared to the contralateral location where no large vessels were present, but a quantitative analysis of the spatial characteristics of the newly formed bone was not performed in the current study19. The scoring measures “presence and completeness of a bridge” and “fluency of the new bone formation” were almost perfectly correlated. A complete bridge was commonly observed with a fluent shape. A possible explanation for this correlation may be the biomechanical changes that occur in the ankylosed spine5. Bone is continuously remodeling under the influence of biomechanical loading as described by Wolff’s law20. In the unaffected spine, the compressive loading pattern is equally distributed throughout each intervertebral disc and vertebral body resulting in predominantly vertical arranged trabeculae21. With the presence of a completely fused bridge, the axial loading will likely be distributed over the elastic intervertebral disc and the new bony bridge. Subsequently it can be hypothesized that this bony bridge may act as a load-sharing structure and will remodel in a vertical direction, producing the characteristic flowing shape.
Potential assessment techniques to study progression of DISH have been previously described. First, a comprehensive scoring system for DISH with acceptable interrater reliability was described by Mata, et al in 199816. Anteroposterior and lateral radiographs (CR) of the complete spinal column, ankles, knees, elbows, shoulders, and pelvis from subjects with DISH and subjects with spondylosis were assessed using categorical and continuous measures. The categorical measurement described the presence and completeness of a bridge (similar to the current study) and rated no ossification present, ossification without bridging, ossification present with incomplete bridging of the disc space, and complete bridging of the disc space by ossification16. Actual results from use of this scoring system were not published, most likely because this scoring system was designed for CR instead of CT imaging. Second, cervical and lumbar radiographs of 141 DISH patients and 146 patients with ankylotic spondylitis were studied by Baraliakos, et al at 2 timepoints within 6 years22. Equal progression measured using modified Stoke Ankylosing Spondylitis Spine Score was seen between the DISH and AS group, and the angles of bone spurs in the DISH population were more often over 45° compared to the AS population (in general angle < 45°). Finally, the natural course of bridging osteophyte formation in DISH was described by Yaniv, et al, who performed a retrospective analysis of CT scans from 26 patients in 201415. Six developmental stages were described in their scoring system and all available CT scans were appraised per vertebral unit for the presence of new bone formation. Fluency or remodeling of the bone and circumferential growth of the bone were not included in their scoring system. The presence of a loose calcified particle between the 2 vertebral bodies was noticed and the authors classified this phenomenon as calcification of the anterior longitudinal ligament. In the present study, a loose calcified particle was also separately recorded, but owing to the low prevalence and the natural course of fusion of the particle with the surrounding new bone over time, this scoring result was merged with the presence of osteophytes (Figure 2). The origin of these isolated particles remains unknown, but possible explanations could be calcification/ossification of the anterior longitudinal ligament, calcification/ossification of the anterior part of the anulus fibrosus, or segregation of a bone particle from an osteophyte.
The new scoring system used in our present work was derived from earlier publications and expert opinion15,16. The overall interrater reliability based on 25 CT scans (corresponding to 318 segments) showed an acceptable outcome for further use. Intraobserver reproducibility was not evaluated in the current study, because the interpretation of the scoring system between observers was suspected to be a more important issue than a repetitive measurement by a single observer. The quality of the intervertebral disc, facet joints, and sacroiliac joints were not included in the new scoring system despite being part of the Resnick and Niwayama criteria6. However, these criteria were primarily designed to distinguish certain advanced cases of DISH from other spinal pathologies such as AS and spondylosis deformans. Subjects with exclusion criteria were already omitted from our population with DISH. In our current study, only the thoracic spine was included because DISH is most frequently present in this region of the spine. The co-occurrence of DISH and AS has been described in the literature, and the lack of clinical information and imaging of the sacroiliac joint in our present study could have resulted in cases with both conditions being included23. However, the subjects in our study have a mean age of over 60 years and in cases with AS, longstanding presence of this condition would most likely have visibly affected the apophyseal joints and intervertebral discs.
Based upon the present results, the group with definite DISH should perhaps be referred to as a group with progressive DISH, because in this group a significant increase was found in the mean bridge score, the mean flow score, and the mean extent of the new bone formation over time (Figure 4 and Figure 5). The results of the new scoring system showed that in both the pre-DISH and definite/progressive DISH group, the process of generating new bone is ongoing and continuous. The dichotomous criteria for DISH as proposed by Resnick and Niwayama do not address this progressive character and might be too strict, including only cases of advanced DISH. Many (less strict) sets of criteria have been proposed in literature, but could not be used in our present study owing to limitations in the imaging performed or the lack of validation, and new criteria (with inclusion of an early stage of DISH) are suggested to be useful for future diagnostic and research purposes14. The current observations can contribute to further studies on the pathogenesis of DISH. In the phase prior to a complete bone bridge, especially when the bridge is almost complete, the new bone and surrounding tissues should be analyzed on a histological and cellular level to understand the principles of the pathogenesis of the new bone formation in DISH.
The clinical status of the included subjects is not included in our present study because the aim of our study was primarily to describe radiological changes seen over time in subjects with DISH. With the development of new and early radiological criteria for DISH, the rate of new bone formation in DISH may be studied in relation to patient characteristics, clinical symptoms, and biomarkers.
The results of our study show that DISH is a progressive condition with an ongoing increase in the overall prevalence of complete bridges and development of broader, more fluent bony bridges. The outcomes support the need for the development of classification criteria for DISH with consecutive phases to describe more accurately the progressive character of this condition.
- Accepted for publication January 19, 2018.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.