
Abstract
Objective. Rates of total knee arthroplasty (TKA) and total hip arthroplasty (THA) remain high for patients with rheumatoid arthritis (RA), who are at risk of flaring after surgery. We aimed to describe rates, characteristics, and risk factors of RA flare within 6 weeks of THA and TKA.
Methods. Patients with RA were recruited prior to elective THA and TKA surgery and prospectively followed. Clinicians evaluated RA clinical characteristics 0–2 weeks before and 6 weeks after surgery. Patients answered questions regarding disease activity including self-reported joint counts and flare status weekly for 6 weeks. Per standard of care, biologics were stopped before surgery, while glucocorticoids and methotrexate (MTX) were typically continued. Multivariable logistic regression was used to identify baseline characteristics associated with postsurgical RA flares.
Results. Of 120 patients, the mean age was 62 years and the median RA duration 14.8 years. Ninety-eight (82%) met 2010/1987 American College of Rheumatology/European League Against Rheumatism criteria, 53 (44%) underwent THA (and the rest TKA), and 61 (51%) were taking biologics. By 6 weeks, 75 (63%) had flared. At baseline, flarers had significantly higher disease activity (as measured by the 28-joint Disease Activity Score), erythrocyte sedimentation rate, C-reactive protein, and pain. Numerically more flarers used biologics, but stopping biologics did not predict flares, and continuing MTX was not protective. A higher baseline disease activity predicted flaring by 6 weeks (OR 2.12, p = 0.02).
Conclusion. Flares are frequent in patients with RA undergoing arthroplasty. Higher baseline disease activity significantly increases the risk. Although more patients stopping biologics flared, this did not independently predict flaring. The effect of early postsurgery flares requires further study.
- RHEUMATOID ARTHRITIS
- TOTAL KNEE ARTHROPLASTY
- TOTAL HIP ARTHROPLASTY
- POSTOPERATIVE FLARE
- RISK FACTORS
The prevalence of disease-modifying antirheumatic drugs (DMARD) and biologics including tumor necrosis factor inhibitors (TNFi) has not meaningfully decreased the use of total hip arthroplasty (THA) and total knee arthroplasty (TKA) for patients with rheumatoid arthritis (RA)1,2. While health-related quality of life and functional status for patients with RA has improved dramatically, rates of THA and TKA have remained stable3,4. THA and TKA are still indicated in RA patients with advanced joint destruction. Contrary to the notion that patients with established RA have “burnt out” inactive disease at the time of arthroplasty, the majority of patients with RA undergoing arthroplasty are taking DMARD and biologics to control joint inflammation5,6. In 1 orthopedic referral hospital, 40% of patients with RA undergoing TKA and 34% of those having THA were treated with biologics, while up to 67% were treated with nonbiologic DMARD5,7. These therapies are often stopped prior to surgery, a practice that may increase the risk of flare in the perioperative period.
Patients with RA are at increased risk of prosthetic joint infection compared to patients with osteoarthritis6, and the use of biologics increases that risk8. The practice has been to discontinue biologics prior to surgery, and the 2017 guidelines of the American College of Rheumatology (ACR) and the American Association of Hip and Knee Surgeons explicitly weigh the risk of flares against the risk of infection9,10. Flares are frequent among patients with RA, and a known precipitant is medication withdrawal11. Increased RA disease activity is characterized by increasing pain and fatigue12, which may lead to difficulty with rehabilitation after arthroplasty, but the risk of flares must be balanced against the increase in the risk of infection if DMARD and biologics are continued through surgery. However, little is known about flares of RA after arthroplasty, and the effect of medication management decisions.
The purpose of our study was to determine the rate, characteristics, and risk factors of patient-reported flares of RA within 6 weeks of THA and TKA.
MATERIALS AND METHODS
Our study is reported per the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cohort studies13. Our study was approved by the Hospital for Special Surgery, New York, ethical review board (#2014-233), and all included patients gave informed consent.
Study design and setting
The RA Perioperative Flare Study is a prospective observational cohort study of patients with RA undergoing THA and TKA at a single, high-volume tertiary care center for musculoskeletal diseases. The records of all patients undergoing THA and TKA were screened to identify patients with RA. All patients with confirmed RA over the age of 18 undergoing THA or TKA were eligible. Patients were recruited consecutively prior to surgery, either on the day of surgery or during the preoperative visit, and underwent a comprehensive evaluation including patient- and physician-reported measures and laboratory evaluations at baseline and at 6 weeks after surgery.
Patients answered a questionnaire each week for 6 consecutive weeks after surgery, addressing RA status and disease flare. Recruitment occurred from November 2013 through September 2016. Patients who flared after surgery were compared to patients who did not flare.
Participants
Participants were undergoing elective THA or TKA and met classification criteria for RA using ACR/European League Against Rheumatism 2010 or 1987 criteria, or were confirmed as having RA by the principal investigator (PI; SMG). Because the study involved a tertiary surgical referral center, many patients received their rheumatologic care elsewhere, so full evaluations including hand and foot radiographs were not available for all cases. However, when patients did not meet criteria at the time of their surgery, the PI examined the patient and contacted their rheumatologist to obtain additional RA-specific information and confirm the diagnosis. All patients undergoing THA or TKA were offered the opportunity to participate in the study. The majority of the hip replacements were performed using a posterolateral approach and the majority of the knee replacements were performed with a medial parapatellar approach. Synovectomies were performed when there was excessive synovitis. Patients had to be English-speaking and agree to complete a series of validated, patient-reported outcome measures.
Data collection
Baseline data collected included age, sex, comorbidities, duration of disease, medications (along with stop date if stopped), MD Health Assessment Questionnaire (MD-HAQ), Routine Assessment of Patient Index Data (RAPID)-3, and the 28-joint Disease Activity Score (DAS28; ≥ 4.1 signified high disease activity)14. Questionnaires were as described above. Serologic status for rheumatoid factor (RF) and anticitrullinated protein antibody (ACPA) were obtained at baseline. Variables completed at each visit were joint counts (excluding the operated joint), inflammatory markers, DAS28, MD-HAQ, and RAPID-3. Medication use was standard of care; biologic DMARD were stopped prior to surgery and the last date of use was recorded. Glucocorticoids (GC) and methotrexate (MTX) were usually continued without change and recorded. Supraphysiologic GC doses (“stress-dose”) given by the anesthesiologist in the operating room (usually 100 mg of hydrocortisone acetate) were also recorded. If a medication was withheld for surgery, the patient was considered a current user. All other DMARD and perioperative medications were recorded. Withheld medications were typically restarted in weeks 4–6.
Assessment of flare
Flare status was determined by MD review of all aggregate data and was used to define flare within all analyses. While flare status did not require MD-patient concordance, discordance was minimal. Patients completed the Rheumatoid Arthritis Flare Questionnaire (RA-FQ) weekly for 6 weeks after surgery, reporting severity and duration of flares, but it was not otherwise scored. The RA-FQ has been validated in clinical and observational trials, and contains 5 items assessing pain, fatigue, stiffness intensity, and global function impairment that can identify and measure RA flares15. Patient-reported flare was defined as a response of “yes” to the anchor question “Are you in a flare?”11. Participants also answered questions about self-management of their disease, change in activity, and medication use.
Because the RA-FQ has not been used in the postoperative setting, participants completed the RAPID-3, and the tender/painful joint region score modified from the Rheumatoid Arthritis Disease Activity Index (RADAI) questionnaire including a self-report of specific painful and swollen joints on a homunculus depicting 40 joints15,16,17,18. Participants also answered questions pertaining to global assessment of disease activity, and completed the Hip (HOOS) or Knee (KOOS) disability and Osteoarthritis Outcome Scores19,20. The HOOS and KOOS are validated lower extremity instruments that are sensitive to change after THA and TKA20,21. Aggregate data were assessed for each patient by 2 investigators (SMG, VPB) after the 6-week visit to assign an MD assessment of flare status (yes or no) and to record which week the flare occurred.
Missing data
At least 1 full questionnaire after baseline had to be completed to be included in the study for patients reporting flare; those not flaring were included if at least 4 questionnaires were completed through Week 6. Missing questionnaires did not affect the flare status assessment when it was evident from the responses on the adjacent weeks on at least 2 questionnaires, because flare status was defined by a change in response from “no” to “yes” over the 6-week time period. In addition, the MD measures had to be completed at baseline and 6 weeks. Baseline characteristics of patients who did not provide the minimum data to ascertain flare status were compared to remaining participants to evaluate bias.
Data analysis
Baseline patient characteristics for patients assessed as having a flare (“flarers”) and those who did not (“nonflarers”) are summarized as frequencies and percentages for categorical variables. The distribution of continuous baseline patient characteristics was assessed for normality using the Shapiro-Wilk test. Continuous characteristics are summarized by mean ± SD or median [interquartile range (IQR)], as appropriate. Categorical variables were compared using Fisher’s exact tests. Student t tests or the Wilcoxon rank-sum test were used, as appropriate, to compare continuous variables.
Univariate logistic regression modeling was performed and OR (95% CI) are reported. Multivariable modeling was performed with log-transformed RADAI (40-joint count adjusted for surgical joint), log-transformed C-reactive protein (CRP), DAS28, log-transformed disease duration in years, MTX, biologic, and GC use, and discontinuation of a biologic > 2 dose intervals prior to surgery. Items were included in the multivariable model if they were significant in the univariate model or on the basis of the research interest. Biologic and MTX use, while not significant in the univariate model, were included in the multivariable model.
Analyses were performed using SAS version 9.4. A 2-tailed p value < 0.05 was considered statistically significant.
RESULTS
Of 23,584 patients screened for possible RA and who were undergoing THA and TKA, 23,230 did not meet inclusion/exclusion, leaving 354 possible cases (Figure 1). Of those, 169 subjects declined to participate, leaving 185 consented subjects. After enrollment, 23 patients withdrew or were withdrawn, and 42 did not complete sufficient questionnaires and were dropped from the study. Of the 23 patients identified as having RA who did not participate, 69.6% did not meet diagnostic criteria, and 30.4% were protocol failures. There was no significant difference in the characteristics of patients who withdrew/were withdrawn from the study compared to those who enrolled in age, sex, race, or disease duration (Supplementary Table 1, available with the online version of this article). However, more participants had a positive RF (43% vs 17%, p = 0.007) and a high positive ACPA (> 3× upper limit of normal, 36% vs 13%, p = 0.02), and more participants were taking biologics (51% vs 20%, p = 0.01) and MTX (52% vs 20%, p = 0.008). While RADAI [median (IQR) of nonparticipants: 4.0 (0.0–8.0) vs participants: 8.0 (5.0–15.0), p < 0.001] and DAS28-ESR (mean 2.7 ± 1.8 in nonparticipants vs 3.5 ± 1.5 in participants) were higher in those who participated, levels of RAPID-3, ESR, and CRP were not significantly different.

Recruitment flowchart.
Of the 120 patients included in the final analysis (Table 1), 99 (83%) were female, 95 (81%) were white, and 53 (44%) were undergoing THA. RA classification criteria were met in most participants. There were no significant differences in patient and disease characteristics or flare rates between the patients undergoing TKA versus THA, or those who flared at baseline versus those who flared later (Supplementary Table 2, available with the online version of this article), so they were analyzed together.
Patient baseline characteristics. Values are n (%) unless otherwise specified.
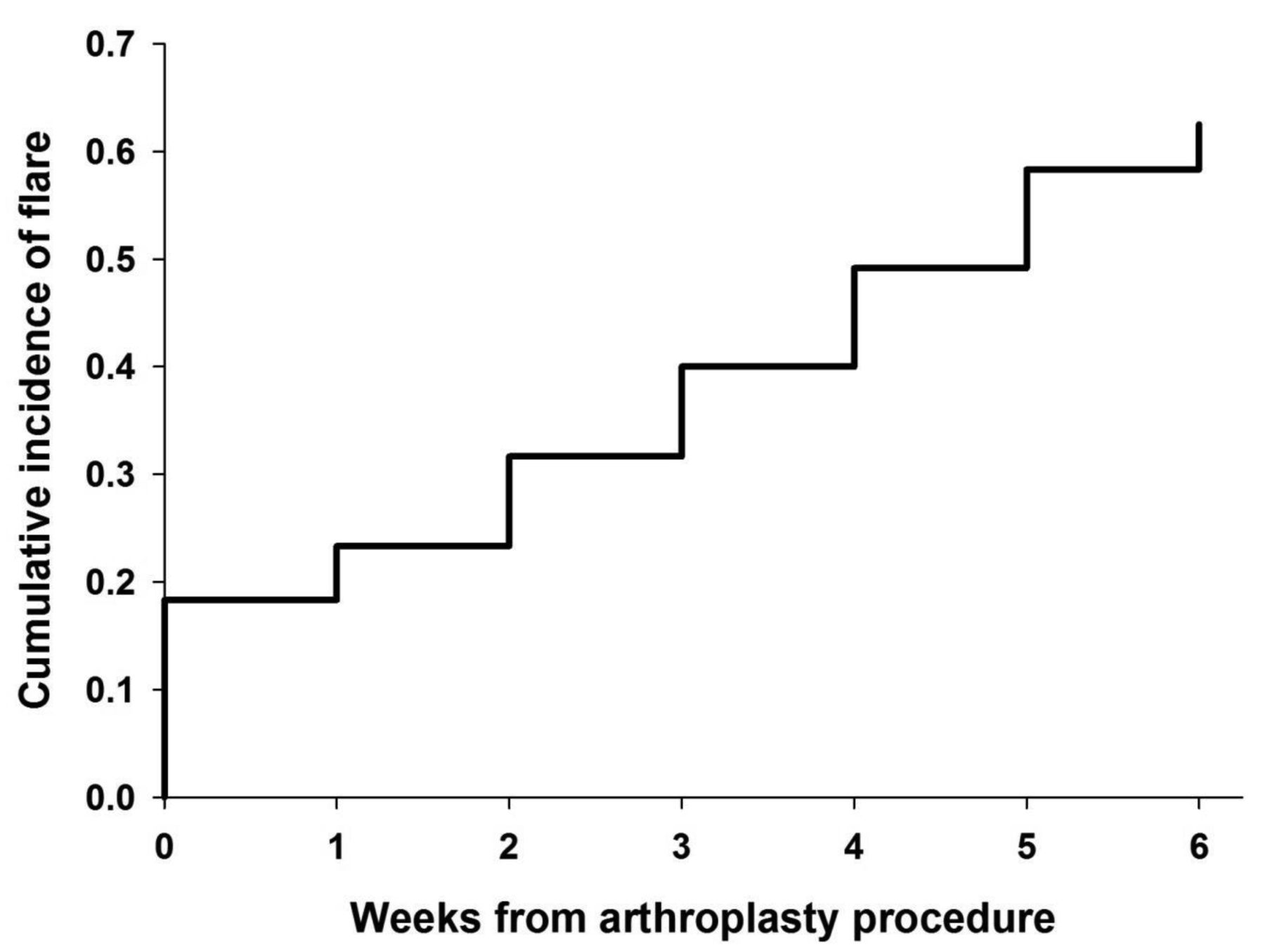
Flares of disease were common and were reported by 63% of patients undergoing THA and TKA (Figure 2). There was little discordance between patients and MD; 7 patients were MD/patient discordant (5.83%). Five patients (4.17%) were “MD Yes” and “Patient No,” and 2 (1.67%) were “MD No” and “Patient Yes.”

{kind=link}
{kind=link}
Proportion of patients with flare versus weeks from arthroplasty procedure.
Among flarers, the median time to flare after surgery was 2 weeks, with a median severity of 7 (1–10 scale), and a median duration of 4–7 days. Although 22 patients reported flaring on the day of surgery at baseline, there was no difference between those with baseline versus postbaseline flare. There was no significant difference in patients who flared in disease characteristics such as disease duration or baseline medication use (Table 2). Numerically more flarers were treated with biologics (57% vs 42%, p = 0.14). There was no difference in MTX use (flarers 51% vs nonflarers 53%) or GC use on the day of surgery (flarers 88% vs nonflarers 86%) between groups. Disease activity was higher at baseline for flarers, with higher DAS28-CRP and ESR, Clinical Disease Activity Index (median 20.0 vs 15.0, p = 0.002), and RAPID-3 (mean 17.0 vs 13.1, p < 0.001). Inflammatory markers such as CRP and ESR were higher at baseline in flarers, and the number of tender joints (median 2.0 vs 1.0, p = 0.013), RADAI Joint Score (median 10 vs 5.0, p < 0.001), and the number of swollen joints were significantly higher (median 4.0 vs 3.0, p = 0.04). A higher proportion of flarers met both the 1987 and 2010 RA criteria compared to patients without flare (49% vs 24%). Patients classified as flarers had significantly worse MD-HAQ function at baseline (mean 4.1 vs 3.4, p = 0.009) and at 6 weeks (median 3.7 vs 2.7, p = 0.002), but the change from baseline to 6 weeks was similar between groups (mean −0.5 vs −0.5, p = 0.97). There was no significant difference in baseline HOOS activity scores (mean 37.3 vs 48.8, p = 0.053), although baseline KOOS was lower (worse) in flarers (38.3 vs 51.5, p = 0.012).
Baseline characteristics of flarers versus nonflarers. Values are n (%) unless otherwise specified.
The majority (52%) of reported flares occurred by Week 2, and rated as severe (> 7/10) in 36% of flarers. Similar numbers of patients managed flares by decreasing their activities; 23% responded “I reduced the amount of activities I did and/or rested more,” 19% responded “I avoided doing activities I had planned to do,” 17% increased their analgesics or antiinflammatories, and 5% increased their GC to manage flare. Only 4% sought help from their rheumatologist. Sixty percent of flares lasted 1–7 days. For half of flarers (51%), the patient global, “considering how active your RA has been, how much difficulty have you had during the last week taking part in activities typical for you?” was > 6/10.
Univariate logistic regression models were analyzed, and results are displayed in Supplementary Table 3 (available with the online version of this article). Relative to patients who met neither the 2010 nor the 1987 RA classification criteria, patients who met both the 2010 and 1987 criteria had a > 5-fold increase in risk of flare (OR 5.89, p = 0.002). Risk of flare appeared higher in those with higher disease activity at baseline. Patients with high disease activity by DAS28-ESR (values > 5.1) were over 25-times more likely to report a flare over the subsequent 6 weeks compared to patients with low disease activity/remission (DAS28-ESR ≤ 2.6; OR 25.59, p = 0.003)14. Elevated RAPID-3 was associated with an increased risk of flare (OR 1.18, p < 0.001). A decreased risk of flare was seen with CRP ≤ 1.5 mg/dl and ≤ 2.0 mg/dl (OR 0.29, p = 0.006, and OR 0.17, p = 0.002, respectively). Patients with normal ESR values (defined by age and sex) also had a lower risk of flare (OR 0.30, p = 0.03).
Multivariable modeling (Table 3) demonstrated that baseline DAS28 (OR 2.11, p = 0.015) and log-transformed RADAI joint score (OR 2.97, p = 0.023) were independent predictors of MD-validated patient report of flare. Increasing levels of CRP increased the risk of flares (OR 4.24, p = 0.035). However, neither disease duration nor medication use, including biologics, increased the risk of flares; discontinuation of a biologic > 2 dose intervals prior to surgery did not increase the risk of flares. Use of MTX at the time of surgery did not independently protect against the risk of flares.
Multivariable logistic regression to predict flare.
DISCUSSION
This is the first study, to our knowledge, to prospectively assess postoperative patient-reported flares of RA in patients undergoing THA and TKA using the RA-FQ, a validated patient-reported outcome instrument for identifying RA flares, in addition to other patient-reported measures11. We found that postoperative flares are frequently reported by patients with RA, who rate them as severe. Patients at highest risk of flaring within 6 weeks of arthroplasty are those who had higher disease activity at baseline. Medication withdrawal does not independently predict flares; while numerically more patients who discontinued biologics flared, it is not an independent risk factor for flares, and continuing MTX at the time of surgery does not independently decrease the risk of flares. Moreover, GC use at the time of surgery was not different between groups. Previous studies of RA flares have not systematically assessed changes in disease activity within 6 weeks of surgery or assessed the potential effect of biologic withdrawal in this setting22. While decreases in overall RA disease activity have been reported ≥ 1 year after arthroplasty, we focused on the immediate postoperative period, when an inflammatory response to the stress of surgery has been reported23,24,25,26,27.
Expectedly, we observed significantly higher baseline joint counts in patients reporting flares after THA and TKA compared to those for whom RA remained stable. Some subjects were already flaring at baseline, because therapies were often stopped 2–12 weeks earlier. However, there was no difference in medication use between those who flared at baseline compared to those who flared later. In addition, multiple outcomes important to patients are significantly worse in patients who report flare after THA and TKA, including self-reported pain, fatigue, stiffness intensity, and global function impairment. At baseline, patients meeting both 2010 and 1987 RA criteria were more likely to flare; this probably reflects the increased disease activity and severity, with elevated joint counts and elevated inflammatory markers required to meet both classification criteria. Similarly, higher disease activity has been associated with flares in nonsurgical RA patients, with flare rates from 4–11% when assessed every 3 months to almost 70% when assessed retrospectively over a 6-month period28,29. Neither of these other studies assessed for flares using a validated instrument. Thus, the higher rates of flare identified in our study may reflect the prospective study design and our systematic frequent assessment of flare in a population who may be at higher risk of flare; the stress of surgery and medication withdrawal can trigger an inflammatory response that may lead to increased inflammation and flares.
Currently, standard perioperative care is to discontinue biologics at the time of arthroplasty to mitigate infection risk9. The incidence of prosthetic joint infections has remained high for patients with RA30,31 and readmission within 90 days of arthroplasty, most commonly for infection, has continued to rise31. Additionally, increased odds of infection (OR 2.47, 95% CI 1.66–3.68) were demonstrated in a metaanalysis comparing patients exposed to TNFi at the time of surgery to those without a recent exposure8. Despite improvement in the status of patients with RA32, poorer outcomes are still reported after arthroplasty, raising concern that postoperative flares linked to withholding medication might affect rehabilitation efforts and outcomes33,34. While our study cannot address flare effect on longterm outcomes, the evidence presented here suggests that medication management decisions are not independent risk factors for postoperative flares.
This information should be regarded in the face of certain limitations. With any cohort study, there is the possibility for unmeasured confounding. Patients with chronic diseases and worse status are known to decline questionnaires more often35,36. Although it is possible that those RA patients with the worst flares dropped out, in our study comparisons of baseline data between those who completed the study and those who did not suggest that the more severe cases tended to participate37. Although we screened all consecutive patients for recruitment to minimize selection and channeling bias, there is the possibility of bias if physicians preferentially encouraged patients with more severe RA to enroll. Our study may not be generalizable because it was performed in a tertiary care hospital with high RA-specific arthroplasty volume, so more severe cases might have been referred for surgery. We used patient-reported flare rather than physician examination with joint counts in the weekly surveys, because it would not be possible to examine patients weekly. However, all measures were carefully assessed to exclude reports of flare that may have been due to pain or surgical symptoms. Nonetheless, postoperative complaints unrelated to disease activity might have been confounding. However, only 6 patients (5%) reported flares at Week 1, when the symptoms attributable to surgery would be maximal. In addition, patient-reported RADAI scores were adjusted to exclude the operative joint. An additional limitation is the lack of a control group, because flares may have been unrelated to surgery. However, we were able to assess the characteristics and risk factors for flares after arthroplasty using the patients with RA who did not flare as a comparator group. A lack of accuracy in reporting medication regimens could also introduce bias, even though this information was carefully collected prospectively. We were unable to assess infection or other complications between groups, which would have added depth to the study. Not all patients with RA undergoing this surgery could be included, owing to failure to meet the inclusion criteria.
Strengths of the study include the prospective design with weekly evaluation of patients’ symptoms and effects plus additional patient-reported measures intended to increase the certainty of validating a patient’s report of flare. All patients with RA undergoing THA or TKA were identified through careful screening to permit recruitment of all consecutive cases. Recall bias was avoided by describing flares and disease status in real time. Serial weekly use of the RA-FQ, RADAI joint symptom questionnaire, and self-reported specific joint counts, plus concordance of 2 investigators after review of all available data including the pattern of active joints and supportive history, further increase the reliability. While the single-center design avoids center differences, a single high-volume tertiary care center with high RA-specific experience may affect generalizability. Importantly, we showed that completion of a detailed questionnaire weekly after surgery was feasible (with 83% completion rates), and this enabled us to confidently describe the rates and characteristics of postoperative RA flares.
Our study demonstrates that RA flares are frequent and severe after arthroplasty. While patients with higher disease activity report more flares, preoperative antirheumatic medication withdrawal is not an independent risk factor for flares. Determining the rate and characteristics of flares in the perioperative setting will enable further research to determine whether these differences in disease activity and worsening symptoms within the first 6 weeks after THA and TKA place these patients at risk for worse longterm outcomes or an increase in adverse events. Given the high rate of disease flares after THA and TKA, the notion that patients with established RA undergoing THA and TKA have “burnt out” disease lends further credence to the spreading idea that RA is an ongoing disease over a lifetime, at best controlled by medication. Additional studies are needed of postoperative flares in patients with established RA and the relationship to longterm outcomes.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
Supported by grant # 1UH2AR067691 from the US National Institutes of Health Accelerating Medicine Partnership program, the Weill Cornell Clinical Translational Science Center (UL1-TR000457-06), and the Block Family Foundation.
- Accepted for publication November 29, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.