
Abstract
Objective. To identify clinical predictors of relapse in childhood autoimmune chronic uveitis after stopping systemic treatment.
Methods. A retrospective, multicenter, cohort study.
Results. Ninety-four children in remission, receiving no treatments and with at least a 6-month followup, were enrolled. A higher probability of maintaining remission after discontinuing treatment was shown in idiopathic compared with juvenile idiopathic arthritis uveitis (Mantel-Cox chi-square = 23.21) if inactivity had been obtained within 6 months from starting systemic treatment (Mantel-Cox chi-square = 24.17) and by antitumor necrosis factor-α treatment (Mantel-Cox chi-square = 6.43).
Conclusion. Type of disease, time, and type of systemic therapy to achieve inactivity predict different duration of uveitis remission after treatment withdrawal.
- CHILDREN
- THERAPY WITHDRAWAL
- AUTOIMMUNE CHRONIC UVEITIS
- RELAPSE
Because it is a serious and potentially disabling disease, a step-by-step immunosuppression therapy is generally used in childhood autoimmune chronic uveitis (cACU)1,2,3. However, once uveitis inactivity is achieved, there is no guideline advice regarding the exact duration of systemic treatment4,5. Evidence suggests that a longer period of inactivity with treatment reduces the chance of relapse after therapy withdrawal6. However, bad disease activity and a worse visual acuity in juvenile idiopathic arthritis (JIA) uveitis are strongly associated with a lower probability of remission7,8. Knowing the natural clinical history of cACU could be helpful in driving therapeutic decisions for each patient. We aimed to identify potential clinical predictors of relapse in patients with cACU who stopped systemic treatment.
MATERIALS AND METHODS
Study design
Ours was a multicenter, retrospective, comparative cohort study from 4 tertiary pediatric rheumatology centers.
Inclusion criteria
At the time of enrollment, patients were required to fulfill the following: (1) disease onset at ≤ 16 years of age; (2) vision-threatening noninfectious, chronic uveitis that previously obtained remission receiving at least 1 disease-modifying antirheumatic drug (DMARD) or/and any biologic modifier treatment as single therapy or as combined therapy for at least 3 months and thereafter discontinued by decision of the involved physician; (3) inactive uveitis (defined as rare cells or < 1 cell per field at standard slit-lamp examination) for at least 3 months after discontinuation of all treatments, including topical treatment, thus achieving remission according to the Standardization of Uveitis Nomenclature (SUN) working group criteria9; (4) outcome measures collected according to the SUN criteria10; and (5) at least a 6-month period of followup without any treatment.
Outcome measures
Main outcome was, once remission was achieved, the time up to the first relapse after discontinuing any treatment. Additionally, we defined inactivity on therapy if inactive uveitis has been maintained for at least 3 consecutive months after discontinuing any steroid treatment, but still receiving systemic therapy. Secondary outcomes were time to achieve uveitis inactivity on therapy, time to steroid discontinuation, and time of inactivity on therapy. Anterior chamber cells and flare were graded according to the SUN grading schemes criteria. Intraocular inflammation was considered “active” or uncontrolled if the inflammatory activity grade was ≥ 1 at any examination9,10.
Study protocol
Chart review has been performed to extract data at the time of the enrollment, and then every 3 months up to the time of the first flare, and in any case when uveitis flared. Data were collected using a customized uveitis database available online (trial.biostatistica.net) for each center with a unique user name and password entering anonymous data, with the coordinating center (Florence) acting as data manager. Because this study is an observational, retrospective chart review, ethical committee approval was not required in accordance with the policy of the involved institutes.
Statistical analysis
A priori power analysis, setting effect size (f) at 0.40 and power at 0.95, showed that 86 participants in all groups combined would be required. The Mann-Whitney U test, Kruskal-Wallis test, Wilcoxon signed-rank test for paired samples, chi-square test, and Fisher’s exact test, when appropriate, were used to compare data. The following data were considered as variables for correlations, and as covariates for the survival curves: age at the entry study/age at the initiation of systemic therapy, sex, associated JIA and joint activity status (active vs inactive), disease duration, age at uveitis onset, uveitis duration, active uveitis duration, time interval between the uveitis onset and the initiation of systemic therapy, drug therapy administration (dose and frequency), concomitant medications including methotrexate (MTX) when used in association with antitumor necrosis-α (anti-TNF-α), cumulative corticosteroid dose and its duration, previous treatment type and duration, number of previous flares, best corrected visual acuity at the time of enrollment, eye complications because of chronic uveitis (including glaucoma, synechiae, band keratopathy, cystoid macular edema, vitritis, and cataract), time to obtain remission, time of inactivity while receiving therapy, and followup time. Pearson and Spearman correlation tests were used to determine correlation coefficients for different variables. To identify predictors of outcome, Cox regression model and Kaplan-Meier curves were constructed, each at the mean of the above-reported covariates. Analyses were performed on SPSS package for MAC, version 23.0 (SPSS).
RESULTS
From June 2013 to December 2015, of 335 children followed for cACU, 94 (28%, median age 11.6 yrs, range 3.2–15.4) were eligible for our study because they had discontinued all treatments and showed a persistent remission over at least 6 months. Sixty-seven (49 female, 18 male) were affected by JIA: 35 oligoarticular onset, 18 polyarticular, 10 psoriatic arthritis, and 4 enthesitis-related arthritis. Twenty-seven (11 female, 16 male) were affected by idiopathic chronic uveitis (IdCU): 9 intermediate and the remaining by panuveitis. Demographic information and other variables reported into the statistical analysis section did not differ between JIA and IdCU. Fifty-three children previously received MTX at 15 mg/mq2/week, 36 adalimumab (ADA) at 24 mg/mq2/2 weeks, and 5 infliximab (IFX) at 8 mg/kg, every 6 weeks in combination with MTX 7.5 mg/week. Twenty-eight children also received MTX in combination with anti-TNF-α: 23 with ADA, 5 with IFX (Table 1).
Comparison of variables for correlations, and as covariates for the survival curves, in 67 children with JIA-associated uveitis and in 27 with IdCU. Continuous variables are expressed as median (range) values.
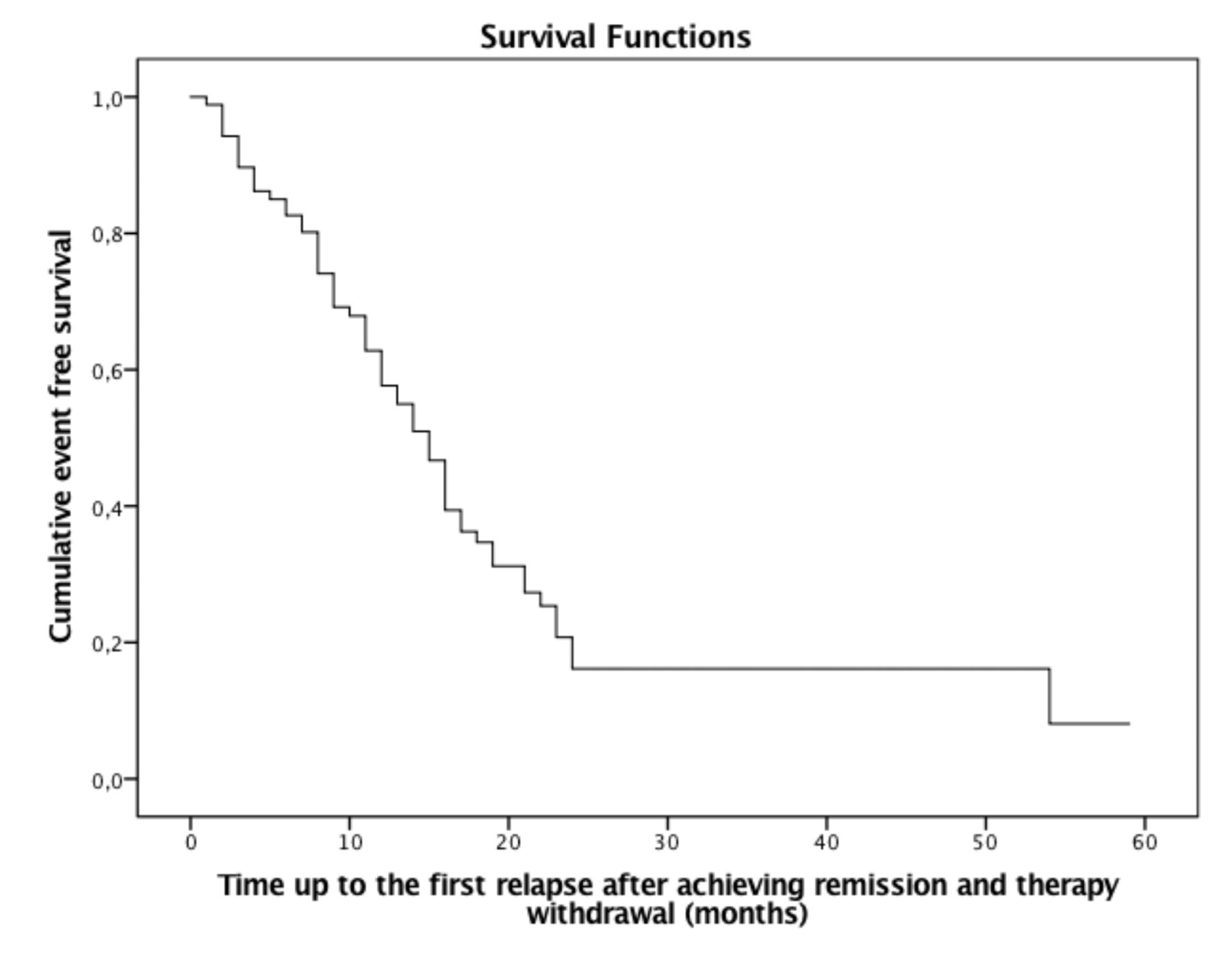
The total median time in remission was 12 months (range 6–59; Figure 1). At last available followup after treatment discontinuation (median 49 mos, range 15–68), 26 out of 87 children (29.9%) maintained a complete remission over a median period of 28 months. Seven children (4 JIA, 3 IdCU) were lost at followup: 3 previously received MTX, 3 IFX, and 1 ADA. At 49 months of followup, which was the longest period common to the 2 groups, 15/24 children with IdCU (62.5%) compared with 11/63 children with JIA (17.4%) were still in remission, while 52/63 JIA-cACU (82.5%) compared with 9/24 IdCU (37.5%) already relapsed at least once during the followup time (Pearson chi-square test-continuity correction = 14.74, p < 0.0001). A higher probability of maintaining uveitis remission after discontinuing treatment was shown in IdCU compared with JIA (Mantel-Cox chi-square = 23.21, p < 0.0001; Figure 2). Antinuclear antibody positivity was associated with a higher probability of uveitis flare in overall population (Mantel-Cox chi-square = 6.12, p < 0.01), but not in subanalysis limited to JIA (Mantel-Cox chi-square = 0.78, p = 0.37) and IdCU (Mantel-Cox chi-square = 2.55, p = 0.11).

Survival curve of the time up to the first uveitis relapse after achieving remission and any therapy withdrawal (time on remission, off therapy) of the 94 children with autoimmune chronic uveitis enrolled.
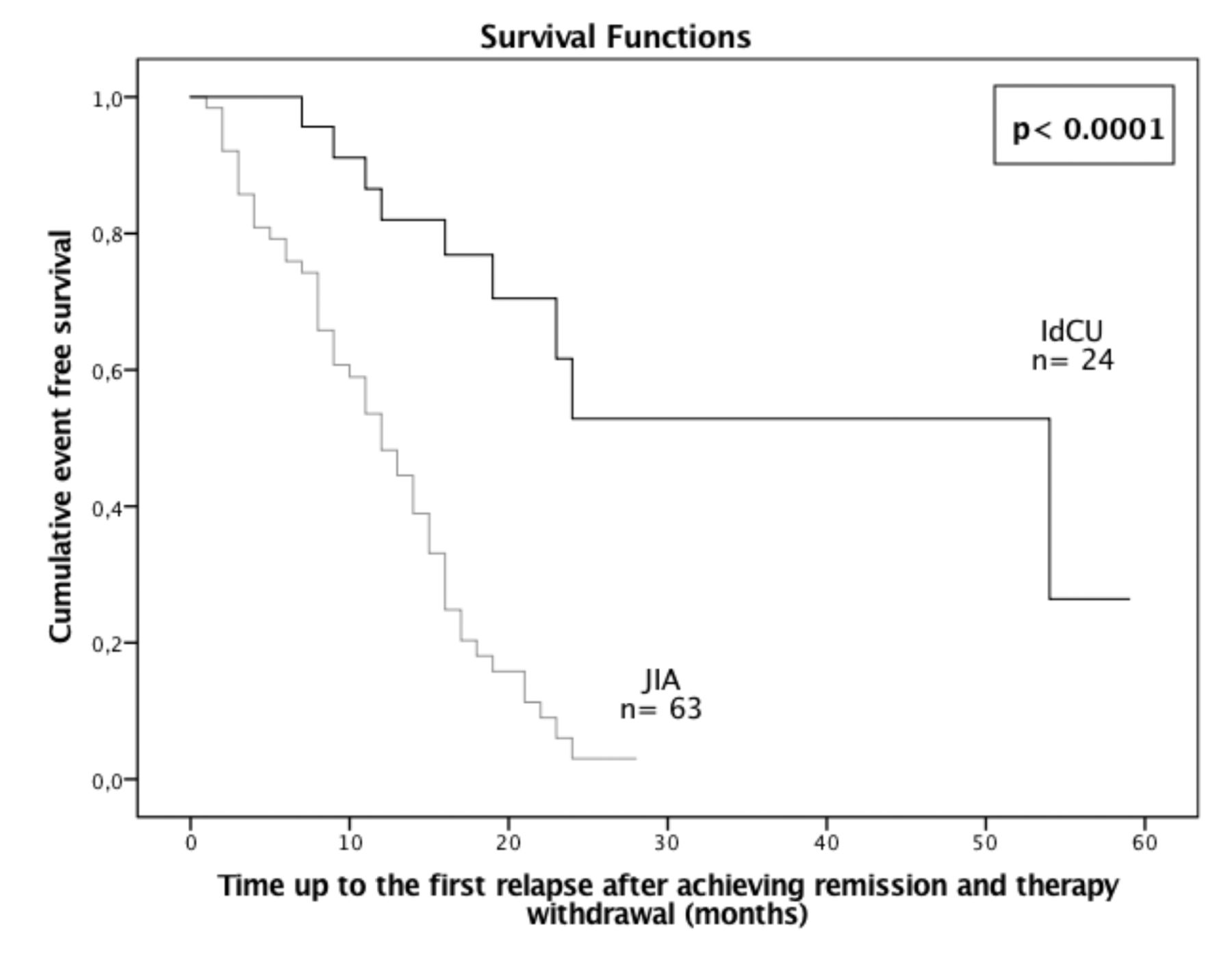
Survival curve of the time up to the first uveitis relapse after achieving remission and any therapy withdrawal (time in remission, off therapy) in IdCU and in JIA-associated uveitis (Log-rank, Mantel-Cox chi-square = 23.21, p < 0.0001). IdCU: idiopathic chronic uveitis; JIA: juvenile idiopathic arthritis.
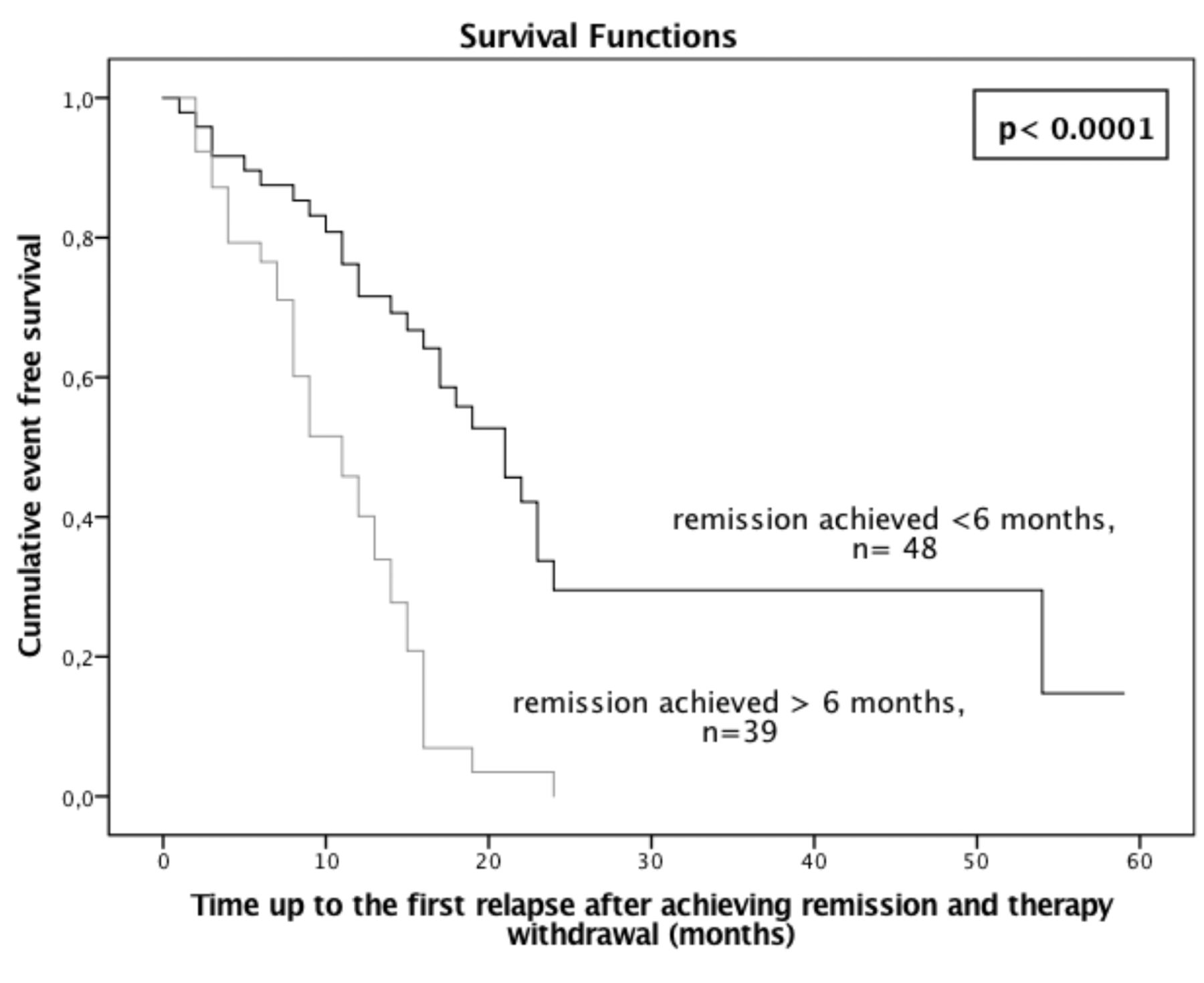
No variable resulted in significant predictors of long-lasting remission without therapy, including sex (Mantel-Cox chi-square = 2.17, p = 0.21), visual acuity (Mantel-Cox chi-square = 1.03, p = 0.21), type of treatment, DMARD vs anti-TNF-α (Mantel-Cox chi-square = 0.23, p = 0.62), concomitant versus nonconcomitant medication (Mantel-Cox chi-square = 0.13, p = 0.83), time of inactivity over 1 year of treatment (Mantel-Cox chi-square = 2.63, p = 0.12), as well as over 2 years of treatment (Mantel-Cox chi-square = 0.05, p = 0.94). However, stratifying the overall cohort by the time to achieve inactivity on treatment, the Cox regression analysis (at mean of the above-reported covariates) showed a higher probability of maintaining remission after treatment discontinuation if remission had been obtained within 6 months from starting systemic treatment (Mantel-Cox chi-square = 24.17, p < 0.0001; Figure 3). At 49 months of followup, 21/48 children who obtained inactivity on therapy within 6 months (43.8%) compared with 5/39 who obtained inactivity on therapy after 6 months (12.8%) were still in remission (Pearson chi-square test-continuity correction = 17.35, p < 0.0001).

{kind=link}
{kind=link}
{kind=link}
Survival curve of the time up to the first uveitis relapse after achieving remission and any therapy withdrawal (time in remission, off therapy) in childhood autoimmune chronic uveitis who obtained inactivity on therapy within 6 months (≤ 6 mos) and after 6 months (> 6 mos) from starting systemic therapy (Log-rank, Mantel-Cox chi-square = 24.17, p = 0.0001).
In children who obtained inactivity on therapy within 6 months, the probability of maintaining remission after treatment discontinuation were significantly higher if they received anti-TNF-α treatment compared with children who received MTX (Mantel-Cox chi-square = 6.43, p = 0.011).
DISCUSSION
Even with a retrospective study, our results suggest that JIA and time to achieve inactivity, rather than the length of treatment, can predict different duration of uveitis remission after therapy withdrawal. Achieving inactivity and remission by anti-TNF-α results in a predictor of low chance of relapse once systemic therapy is stopped. If duplicated in a prospective study, these data might be helpful in building up a tailored therapy for a better standard of care.
As previously reported11,12,13,14, we confirm that JIA uveitis shows a persistent chronic course with a risk of relapse after treatment withdrawal that is significantly higher than that of IdCU over time. In agreement with Kalinina Ayuso, et al6 regarding MTX withdrawal, our data in a larger cohort confirm the majority of cACU relapse over 1 year after stopping treatment. Unfortunately, we were not able to replicate that a longer period of remission on treatment reduces the chance of relapse after stopping therapy. Conversely, our present study points out that a shorter time to achieve persistent inactivity on treatment represents a significant predictor to keep inactivity once systemic treatment is stopped. In addition, to the best of our knowledge, our cohort represents the longest and largest cohort of cACU reporting natural history after anti-TNF-α and MTX treatment withdrawal. To date, several multicenter studies have attempted to identify predictors of remission in chronic uveitis in adults as well as in children15,16,17,18,19, but data are lacking regarding the optimal duration for systemic treatment and the risk of relapse after therapy withdrawal.
Before drawing firm conclusions, some limitations must be discussed. First, the inherent selection bias of 4 tertiary referral centers must be considered; in addition, children enrolled represent a heterogeneous population with possible variable responses to treatment. However, outcome results were weighted and corrected to include significant clinical variables, such as concomitant medication and visual acuity.
Heterogeneity due to the underlying disease might also affect these results, even if we also reported a subcohort analysis limited to JIA. Further, since different cACU are not included in our cohort, our present data might not represent the effect size of the overall cACU population. However, eligible children derived from the 335 children with cACU, encompassing different types of uveitis (Behçet, early onset sarcoidosis, tubulointerstitial nephritis, and uveitis syndrome) and doubtless JIA and IdCU, represent the most diffuse uveitis types in the pediatric population.
Notably, another shortcoming is the type of assigned treatment used; it was not randomly assigned, but chosen based on physician decision, current knowledge of systemic treatment in cACU, and drug availability.
However, ours might be a pilot study for a multicenter prospective study aimed to identify, according to JIA or not JIA uveitis, time and type of systemic therapy to achieve inactivity, the more suitable approach to obtain the longest possible remission after therapy withdrawal.
- Accepted for publication February 21, 2017.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.