
Abstract
Objective. To clarify whether magnetic resonance imaging (MRI) bone edema predicts the development of rapid radiographic progression (RRP) in the Nagasaki University Early Arthritis Cohort of patients with early-stage rheumatoid arthritis (RA).
Methods. Patients with early-stage RA (n = 76) were enrolled and underwent 1.5-T MRI of both wrists and finger joints. Synovitis, bone edema, and bone erosion were evaluated using the Rheumatoid Arthritis Magnetic Resonance Imaging Scoring (RAMRIS). RRP was defined as an annual increment > 3 at 1 year by the Genant-modified Sharp score of plain radiographs. A multivariate logistic regression analysis was performed to establish the risk factors for RRP.
Results. Median disease duration at enrollment was 3 months. RRP was found in 12 of the 76 patients at 1 year. A univariate analysis revealed that matrix metalloprotease-3, RAMRIS bone edema score, and RAMRIS bone erosion score were associated with RRP. Multivariate logistic regression analyses demonstrated that the RAMRIS bone edema score at enrollment (5-point increase, OR 2.18, 95% CI 1.32–3.59, p = 0.002) was the only independent predictor of the development of RRP at 1 year. A receiver-operating characteristic analysis identified the best cutoff value for RAMRIS bone edema score as 5. RRP was significantly rare among the patients with a RAMRIS bone edema score < 5 at enrollment (2 from 50 patients).
Conclusion. Our findings suggest that MRI bone edema is closely associated with the development of RRP in patients with early-stage RA. Physicians should carefully control the disease activity when MRI bone edema is observed in patients with early RA.
- MAGNETIC RESONANCE IMAGING
- BONE EDEMA
- RAPID RADIOGRAPHIC PROGRESSION
- EARLY-STAGE RHEUMATOID ARTHRITIS
The pattern of bone edema on magnetic resonance imaging (MRI) has a signal quality similar to that of inflamed synovium and has been suggested to reflect true inflammatory infiltrates rather than a pure accumulation of extra-cellular fluid1,2,3,4,5. Bone edema near sites of rheumatoid synovitis-related inflammation are heavily vascularized, contributing to the high water content and enhanced visibility on MRI1,2,3,4,5. Our previous studies of patients with early-stage rheumatoid arthritis (RA) revealed that the presence of bone edema is associated with anticitrullinated protein antibodies (ACPA) and HLA-DRB1*0405 allele carriership6,7, indicating that bone edema is an important feature that reflects the typical RA phenotype.
The development of rapid radiographic progression (RRP) is considered a poor outcome in patients with RA. RRP is identified by measuring a patient’s annual plain radiographic progression. The prevalence as well as the prediction of RRP have been described for patients with RA in Western countries8,9,10,11. The retardation of RRP development was described in Japanese patients with active RA treated with the combination therapy of adalimumab (ADA) with methotrexate (MTX) compared with MTX alone in a clinical trial12. However, to date, the risk model of RRP in Japanese patients with RA has been unclear.
Considering the therapeutic window of opportunity in RA13, the risk estimation of RRP is considered more timely in early RA compared with established RA, and in fact, risk models of RRP in patients with early-stage RA have been developed in Western countries8,9,10. These risk models consist of physical synovitis and serum variables at baseline; MRI findings are not included8,9,10. Our previous study demonstrated that MRI findings including bone edema not only are sensitive but accurately reflect the joint inflammation compared with joint tenderness and swelling in patients with early-stage RA14.
Since synovitis, bone edema, and bone erosion detected by MRI are known as risk factors for further radiographic progression15,16,17,18,19,20, we hypothesized that MRI findings could be informative variables that could be used to establish a risk model of RRP in patients with early-stage RA. In our study, we investigated whether MRI findings, especially bone edema, predicted the development of RRP by using the Nagasaki Early Arthritis Cohort, in which both the wrist and finger joints of the cohort were examined by MRI.
MATERIALS AND METHODS
Study population
The Nagasaki Early Arthritis Cohort opened in 2001 as part of the Unit of Translational Medicine, Department of Immunology and Rheumatology, Nagasaki University Graduate School of Biomedical Sciences21,22. The patients in this cohort were referred from an area in the western part of Japan, Nagasaki Prefecture, which had about 450,000 inhabitants. From our ongoing prospective observational study conducted through this unit, 95 patients with early-stage RA whose disease duration at enrollment was < 12 months and who had taken disease-modifying antirheumatic drugs (DMARD) within 1 month after MRI examinations were consecutively recruited between 2003 and 2011 for our present study; their disease status was formally confirmed by Japan College of Rheumatology–certified rheumatologists.
Our present study was a prospective and observational cohort study conducted to investigate the variables predicting the development of RRP at 1 year after study enrollment in patients with early-stage RA. We examined the MRI of both the wrists and finger joints of the study subjects, all of whom expressed manifestations of rheumatic disease of the wrist and finger joints at enrollment. The clinical diagnosis of RA (reference standard RA) of the 95 subjects was made according to the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) definition: fulfilling both the 1987 criteria of the ACR for RA and the administration of DMARD within the first year23. Full datasets were available for 76 of the 95 patients. The DMARD administered within the first year among these 76 patients were MTX, 33 patients; sulfasalazine (SSZ), 4; bucillamine (BUC), 3; tacrolimus (TAC) 3; leflunomide, 5; MTX plus SSZ, 2; MTX plus SSZ and BUC, 1; MTX plus SSZ and mizoribine (MZR), 1; MTX plus infliximab, 8; MTX plus tocilizumab (TCZ), 2; MTX plus etanercept (ETN), 2; SSZ plus ETN, 1; TAC plus ETN, 1; TCZ, 1; ADA, 1; switched SSZ to MTX, 2; switched SSZ to BUC, 1; switched SSZ to TAC, 1; switched BUC to MTX, 1; switched TAC to MTX, 2; and switched MZR to TAC, 1.
The baseline clinical manifestations and variables included sex, age, disease duration from onset to entry, morning stiffness, DMARD, glucocorticoid, 28-joint Disease Activity Score with C-reactive protein (DAS28-CRP), CRP (measured by latex turbidimetric immunosorbent assay; Daiichi Pure Chemicals), matrix metalloprotease-3 (MMP-3; measured by ELISA; the cutoff value was 59.7 ng/ml for women and 121.0 ng/ml for men; Daiichi Pure Chemicals), ACPA (measured by ELISA with a cutoff value of 4.5 U/ml; DIASTAT Anti-CCP, Axis-Shield), rheumatoid factor (RF; measured by latex-enhanced immunonephelometric assay with a cutoff value of 14 IU/ml; Dade Behring), MRI-proven symmetrical synovitis, MRI-proven bone edema, MRI-proven bone erosion, and plain radiographs of both the hands and feet. All variables were examined on the same day, as described7,14,21,22.
Each patient provided a signed consent form to participate in the study, which was approved by the Institutional Review Board of Nagasaki University. Ours was a prospective, observational cohort study, but we advised all of the participating rheumatologists to treat the patients based on the patients’ DAS28-CRP values. We did not refer to the choice of DMARD. All of the patients were examined every 3 months, including all the above variables except for MRI and plain radiographs, which were examined at enrollment and at 1 year. We estimated the therapeutic effect at 3 months using the DAS28-EULAR response criteria.
MRI of wrists and finger joints
MRI of both wrists and all finger joints were acquired using a 1.5-T system (Sigma, GE Medical Systems) with an extremity coil. Coronal T1-weighted spin echo (TR 450, TE 13) and short-tau inversion recovery (TR 3000, TE 12, T1 160) images were acquired. The images were evaluated for synovitis, bone edema, and bone erosion with an injection of 0.1 mmol/kg of gadolinium-diethylenetriaminepentacetate (Magnevist, Schering). The MRI were semiquantitatively evaluated by experienced radiologists (MU and ST) according to the Rheumatoid Arthritis Magnetic Resonance Imaging Scoring (RAMRIS) as described24,25. RAMRIS scores of synovitis, bone edema, and bone erosion were examined by consensus opinion through 2 experienced radiologists. Inter- and intraobserver reliability of RAMRIS synovitis, bone edema, and bone erosion scores were 0.80, 0.85, 0.81, and 0.88, 0.92, 0.86, respectively, which were considered high enough to study accurately.
Plain radiographs
Plain radiographs of both hands were examined and assessed using the Genant-modified Sharp score (GSS) as described26. RRP in the modified total Sharp score (mTSS; 448 points in total) is usually identified as the Δ (annual) increment of mTSS > 3 or 58,9,27. Because the total possible GSS score is 290 points, RRP in our present study was defined as an annual increment of > 3 points. In fact, a Δ increment of GSS > 1.5 is used as the definition of radiographic progression in the ACT-RAY (a double-blind, TCZ versus placebo-controlled clinical trial evaluating X-ray in RA) clinical trial, in which patients with RA were treated with TCZ in the presence or absence of MTX28. We thus consider the Δ increment of GSS > 3 appropriate as the definition of RRP in our present study.
Statistical analysis
We used Fisher’s exact probability test and the Mann-Whitney U test to assess statistical differences. All statistical analyses were performed using SAS 9.4 software (SAS Institute). The variables with a p value < 0.05 were considered significant. We first performed a univariate analysis to select the variables associated with RRP, then included all variables at p < 0.2 in a multiple logistic regression model. Positive predictive values (PPV) and negative predictive values (NPV) were calculated, and the area under the curve of the receiver-operating characteristic curve was identified to analyze the discriminative value of the matrix in predicting RRP.
RESULTS
Baseline characteristics of the 76 patients with early RA
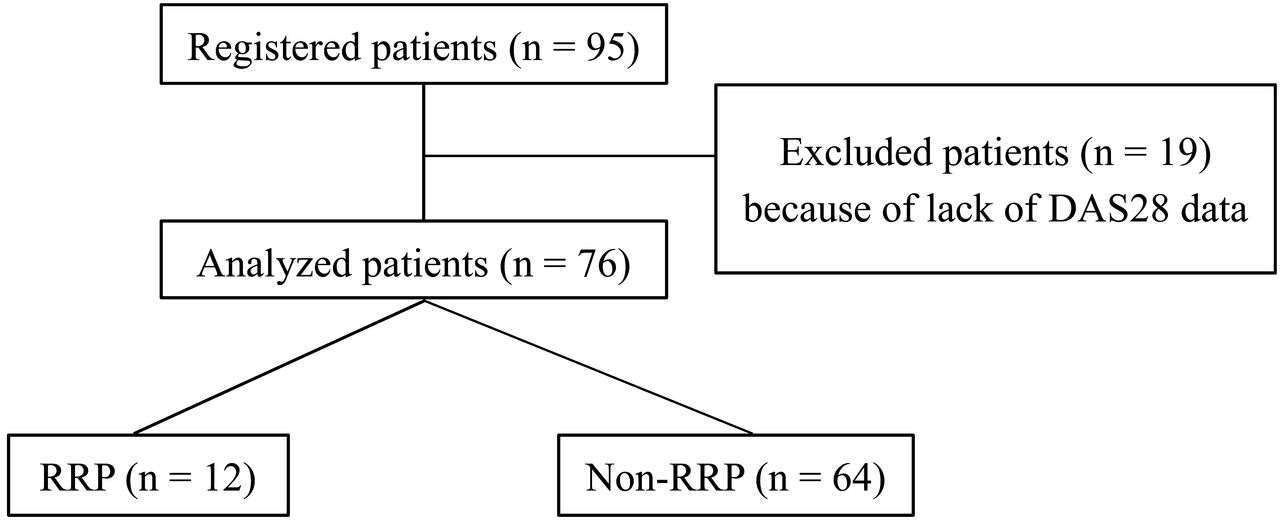
Among the 95 patients at enrollment, the full clinical dataset was available for 76 patients at 1 year of followup (Figure 1). The characteristics of these 76 patients at enrollment are shown in Table 1. The median disease duration was 3 months, and that of 65 of the 76 patients (86%) was less than 6 months. In total, 79.0% and 82.9% of the patients were positive for RF and ACPA, respectively. The median DAS28-CRP value at enrollment was 4.31. These data indicate that most of the subjects in our present study were seropositive early RA with high activity. The median RAMRIS synovitis score, RAMRIS bone edema score, RAMRIS bone erosion score, and GSS score at enrollment were 9, 1, 0, and 0, respectively.

Flow chart of patients with RA enrolled in this study. DAS28: 28-joint Disease Activity Score; RRP: rapid radiographic progression; RA: rheumatoid arthritis.
Association between baseline characteristics and RRP (univariate analyses). Values are median (interquartile range) unless otherwise specified.
Bone edema at enrollment is the only predictor of RRP development at 1 year
We performed a univariate analysis to select the variables associated with RRP. At 1 year after enrollment, the 76 patients’ median Δ increase in the GSS score was 0, with a mean ± SD of 3.35 ± 16.0. RRP was observed in 12 patients (16%). The univariate analysis showed that the MMP-3 concentration, RAMRIS bone edema score, and RAMRIS bone erosion score were significantly higher in the RRP group compared with the non-RRP group (n = 64; Table 1). The seropositivity of ACPA, CRP concentrations, RAMRIS synovitis score, and GSS score were marginally higher in the RRP group (p values between 0.05 and 0.20). Tender joint count and swollen joint count (SJC) at enrollment (data not shown) were not significantly different between the RRP and non-RRP groups.
The treatment regimen may affect the development of RRP. Because about 70% of the present study’s patients were classified as moderate or good responders based on the DAS28-EULAR response criteria at 3 months, the choices of DMARD were considered to be appropriate. The rate of moderate or good responders at 3 months and the use of MTX as the first-line conventional synthetic DMARD (csDMARD) and biological DMARD (bDMARD) use within 6 months of enrollment were comparable between the 2 groups (Table 1), indicating that the treatment regimen may not be significantly associated with the development of RRP in the present patient series.
In the multivariate analysis (Table 2), the MRI bone edema score at enrollment was revealed as the only independent predictor of the development of RRP at 1 year (OR 2.176, 95% CI 1.319–3.590, p = 0.0023). There was no statistical significance with analysis for multiple interactions, e.g., synovitis and edema, edema and erosion (Mann-Whitney U test). An MRI bone edema score ≥ 5 at enrollment was associated with the risk of development of RRP, with 83.3% sensitivity, 75% specificity, 38.5% PPV, 96% NPV, and 76% accuracy (Figure 2).

ROC curve for RAMRIS bone marrow edema score for RRP. The area under the ROC curve was 0.86, with cutoff point of RAMRIS bone marrow edema score ≥ 5. ROC: receiver-operating characteristic; RAMRIS: Rheumatoid Arthritis Magnetic Resonance Imaging Scoring; RRP: rapid radiographic progression.
Multivariate logistic regression analysis for RRP.
We next divided the patients by the RAMRIS bone edema cutoff score of 5 at enrollment and compared the cumulative probability plots of Δ increment of GSS score at 1 year (Figure 3): 26 patients (34.2%) had an MRI bone edema score ≥ 5, and 50 patients (65.8%) had an MRI bone edema score < 5. As expected, RRP at 1 year was significantly rare among the patients with a RAMRIS bone edema score < 5 at enrollment (2 of the 50 patients, 4%, p = 0.0002 vs MRI bone edema score ≥ 5 at enrollment, 38.5%). Inversely, the rate of no radiographic progression at 1 year (Δ increment of GSS score at 1 yr ≤ 0) was significantly low in the group with an MRI bone edema score ≥ 5 at enrollment compared with the MRI bone edema score < 5 at enrollment group (30.8% vs 84.0%, p < 0.0001).

{kind=link}
{kind=link}
{kind=link}
Cumulative probability plots for GSS at 1 year. Triangles: total (n = 76). Open circles: RAMRIS bone marrow edema score < 5 (n = 50). Dark circles: RAMRIS bone marrow edema score ≥ 5 (n = 26). GSS: Genant-modified Sharp score; RAMRIS: Rheumatoid Arthritis Magnetic Resonance Imaging Scoring.
DISCUSSION
As stated in the international treat-to-target (T2T) recommendations29, the EULAR 2013 update30, and the ACR 2012 update31, the main objective for the treatment of RA is to improve or maintain the patient’s quality of life (QOL). It is well known that the impairment of the QOL of patients with RA largely depends on joint damage32, and thus radiographic damage in patients with RA is one of the most important outcome measures in both clinical practice and clinical trials8,9,10,11,12. Because joint damage has been demonstrated to develop significantly in the early phase of RA33, the management of the radiographic outcome of patients with early-stage RA is particularly indispensable to improve these patients’ prognosis.
In the EULAR recommendations for the use of imaging of the joints in the clinical management of RA, recommendation #5 states that MRI bone edema is a strong independent predictor of subsequent radiographic progression in early RA and should be considered for use as a prognostic indicator20. This statement is drawn from several prospective investigations15,16,17,18,19. Subsequent to these investigations, our present study revealed new information about MRI bone edema as a predictor of radiographic progression.
Indeed, the outcome set in our present study was not the radiographic damage, but the RRP. Effective therapies can reduce the odds of radiographic progression by as much as 78%34, and both early and intensive treatment can alter the course of the disease by slowing the rate of radiographic progression even in the mid- to longterm observational periods35,36,37. However, RRP occurs in a subset of treated patients with RA, and thus the identification of individual patients with RA at high risk of developing RRP is critical to making appropriate treatment choices, especially in the early stage of RA. Our present findings showed that MRI bone edema is the most significant predictor toward the subsequent development of RRP at 1 year.
Several risk models for the prediction of RRP in early-stage RA have been developed based on clinical trials including the Active-Controlled Study of Patients Receiving Infliximab for the Treatment of Rheumatoid Arthritis of Early Onset8 and the BeSt (Behandel Strategieën, i.e., Treatment Strategies Study)9 trials and an observational cohort10. These risk models indicated that the baseline variables such as elevated SJC, CRP, ESR, RF, ACPA, and plain radiographic erosion are risk factors for RRP. Our present investigation also includes the above variables, but even in the univariate analysis, the MRI findings appeared to be significantly associated with RRP compared with SJC, CRP, RF, ACPA, and plain radiographic injuries. These data reinforce the involvement of MRI, which can directly visualize and objectively quantify the synovial inflammatory process in patients with RA, especially those at a very early stage20.
Among MRI findings, MRI bone edema is the best variable to predict the development of RRP. This is consistent with our previous report that MRI bone edema is the most specific variable for classifying patients with early arthritis into an RA group compared with MRI synovitis or bone erosion21. In that previous report, the OR of ACPA to classify patients with early arthritis into the RA group was higher than that of MRI bone edema21; however, ACPA was not extracted as a predictor of RRP in our present study. These data suggest that the predictive variables for the early classification/diagnosis of RA are somewhat different from those that could be used for the early prognostic evaluation of radiographic damage.
Because the maturation of osteoclasts, in which the cells preferentially form bone erosion, is detected at the site of MRI bone edema in patients with RA1,2,3, MRI bone edema is likely to be strongly associated with RRP compared with ACPA. Receptor activator of nuclear factor-κB ligand, an essential cytokine for osteoclast development and activation, does not directly correlate with the clinical disease activity of RA38, and thus no associations of SJC and CRP with RRP were identified in our present study, unlike MRI bone edema. Plain radiographic injuries, and even MRI bone erosion, do not predict the development of RRP compared with MRI bone edema, reflecting the previous finding that bone edema forms earlier than bone erosion1. The past report39 that MRI bone edema does correspond with regions where there is a cellular infiltrate replacing marrow fat in subchondral trabecular bone may support our study. The effect of bone edema toward RRP was also identified in another aspect of RA in our present study, in that the achievement of structural remission at 1 year as shown by GSS score was preferentially induced in the patients whose RAMRIS bone edema score was low at enrollment.
Our present study includes the following limitations. We extracted the index to predict RRP using multiple variables; however, the number of patients was small, with only 12 developing RRP. Although this was a prospective cohort and we recommended that the participating rheumatologists treat the patients with falling DAS28-CRP values every 3 months, the treatment choice depended on the decision of each rheumatologist. The rate of MTX as the first-line csDMARD or bDMARD use within 6 months and the DAS28-CRP value at 3 months were not predictive of RRP; however, the treatment regimens might have resulted in bias. A randomized placebo-controlled trial of golimumab has clearly shown that a high RAMRIS bone edema score at enrollment is an independent predictor of radiographic progression at 1 year40. Such distinctive protocol-driven investigations are necessary to test our present findings.
Bone edema in patients with RA at enrollment is the most significant predictor of RRP at 1 year. Our present data indicate that a RAMRIS bone edema score ≥ 5.0 predicts the development of RRP with 83.3% sensitivity and 75.0% specificity. Importantly, our cohort of patients with early-stage RA included 34.2% with a RAMRIS bone edema score at enrollment ≥ 5.0, indicating that a substantial population among patients with early-stage RA are at risk of developing RRP. Our findings might be useful for deciding which patients must receive early aggressive therapy with biologic DMARD in daily clinical practice. MRI bone edema may also be considered as an imaging biomarker that allows triage of patients with RA strictly by T2T therapeutic strategy.
- Accepted for publication March 31, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.