
Abstract
Objective. Successful management of rheumatic conditions involves increasing complexity of care. Delivering this in a holistic way is a growing challenge. The aim of our study was to develop a Patient Concerns Inventory (PCI) and assess it in the rheumatology clinic setting.
Methods. This observational exploratory study occurred with 2 phases. In phase I, the PCI was developed after a systematic literature search, expert opinion, and 3 patient focus group discussions. In phase II, the PCI was piloted in a general rheumatology clinic.
Results. Fifty-four patients were assessed in the pre-PCI group and 51 in the post-PCI group. Median (IQR) duration of consultation was 8 min (5–14) without PCI and 15 min (10–20) with PCI. The pre-PCI group raised 335 concerns from 50 patients, median (IQR) of 5 (3–10) per patient, rising post-PCI to 521 concerns, median (IQR) of 9 (5–16) from 51 patients, p = 0.002. Additional concerns predominantly arose from “physical and functional well-being” and “social care and well-being” domains. Most patients rated their experience with their doctor in the consultation as excellent or outstanding across all 11 questions in the questionnaire, both before and after the introduction of the PCI to the clinic setting.
Conclusion. The PCI is a useful holistic needs assessment tool for rheumatology clinics. Although its use may initially prolong the consultation slightly, patients can raise a significantly higher number of concerns, which does not occur at the expense of patient satisfaction. This may help in identifying areas of unmet needs that previously went unnoticed.
- PATIENT CONCERNS INVENTORY
- PATIENT SATISFACTION
- HOLISTIC NEEDS ASSESSMENT
- UNMET NEEDS
Rheumatology services deal with a wide range of conditions that includes inflammatory arthritis, osteoarthritis, and connective tissue disorders, all of which may have profound detrimental effects on the quality of life. The care of rheumatology diseases has improved considerably over the last few decades, with the advent of biological agents1,2,3,4,5,6,7, establishment of registries8, and development of protocolized, target-driven disease management pathways. The net effect is to encourage early identification and manage disease as dynamically and actively as possible9,10. As a result of this shift and increasing financial pressures worldwide, patient encounters have become more pressured, with less time for interaction.
Because rheumatic conditions tend to run a longterm course, the need for a holistic approach is essential if the many different problems that patients may encounter are to be adequately addressed11,12, including pain, reduced function, loss of independence, infertility, and appearance and psychological issues. Some problems are potentially difficult or embarrassing to talk about and therefore may be underreported and underrecognized13,14. This problem can be compounded in a busy clinic, where the clinician, who may be a doctor, nurse, physiotherapist or occupational therapist, might not have the time to take an exhaustive history. It would therefore be advantageous to have a system in place that allows the patient and clinician to focus specifically on issues that are most relevant to the patient at that particular time.
Such a problem is not unique to rheumatology. Rogers, et al developed a Patient Concerns Inventory (PCI) for use in patients with head and neck cancer15. The purpose of the PCI is to provide patients with a list of potential concerns, which they highlight shortly before their consultation, thereby helping the clinician to focus on and address those problems that were most relevant to the individual patient. The ultimate aim is to improve efficiency of the consultation and patient satisfaction. Experience from the head and neck cancer PCI indicates that this is a feasible and effective tool for use in the outpatient setting16,17,18,19,20,21,22,23,24,25. A PCI was also piloted for the neurooncology setting26. The outcomes from that study showed that patient satisfaction was high and that the PCI was able to address many issues that were not covered by other general cancer needs assessment tools. A similar study of 21 patients was carried out in breast oncology27, where the PCI was able to identify 121 items of unmet need in patients with breast cancer.
There are many self-report questionnaires already in use in rheumatology28,29,30. However, most are disease-specific and used to monitor disease activity or therapeutic response. Other scores are problem-specific, such as Health Assessment Questionnaire (HAQ; physical activity) and visual analog scale (pain). While there has been considerable effort to develop and measure patient-reported outcomes (PRO) for rheumatic diseases, these have not been linked directly with patient concerns, which have been implied and not prospectively identified. We therefore set out to develop a tool that could allow a holistic needs assessment to be undertaken efficiently and effectively in rheumatology and could subsequently inform the future design and interpretation of PRO.
MATERIALS AND METHODS
Our study was approved by the National Research Ethics Service Northwest ethics board (REC reference 12/NW/0312).
In phase I, a rheumatology-specific PCI was developed, using literature, expert opinion from healthcare professionals, and patient focus groups. In phase II, it was piloted in a general rheumatology outpatient clinic, analyzing patient satisfaction and length of consultation.
Phase I: development of a rheumatology-specific PCI
A literature review was conducted to identify issues relevant to patients with musculoskeletal diseases (supplementary data available from the authors on request). A further search looked for papers that used any health-related quality of life (HRQOL) measured within the rheumatology setting. Papers were selected on their titles and compatibility with inclusion and exclusion criteria. Search terms were charted to subject headings. Abstracts of relevant papers were read, and when appropriate, full papers accessed. Any relevant concerns within accessed HRQOL tools were extrapolated.
Second, 19 clinical specialists (rheumatology consultants/postgraduate trainees/specialist nurses, physiotherapist, occupational therapist, pharmacist, general medical trainees, and an orthopedic surgeon) were consulted about issues they considered most important to their patients and given the task of further refining the list of PCI items from the literature review.
Third, 3 focus groups, drawn from patients attending rheumatology outpatient clinics between February and April 2013, provided feedback regarding the PCI. All patients visiting the clinic during the recruitment period were invited to attend, with no exclusions. Seventeen patients expressed an interest in being involved in the focus groups; 16 (n = 4, 5, and 7) patients attended the focus groups. The age range was 46–70 years (7 male, 9 female). To encourage candor, 2 nonclinical researchers (M.O. and J.K.), not associated with the rheumatology clinic, facilitated the focus groups.
Participants had previously been given information sheets. The PCI categories were provided at the start of the focus group. Participants were invited to consider 4 questions when discussing each item: (1) Is this something that might concern you or be important to you, either now or in the past or the future? (2) Is this something that you might want to talk to your doctor or other healthcare professional about? (3) Do you think that this item should be on the PCI? and (4) What do you think about the wording of this item?
Patients were also asked whether any important items were missing from the PCI and to comment on its structure. Discussions were digitally recorded and researchers took notes throughout, encouraging participants to clarify any ambiguous comments and guiding them through the items of the PCI.
Focus group data were analyzed using an adapted framework analysis approach31,32, which allowed researchers to systematically work through the data collected. This first involved researchers (M.O. and J.K.) immersing themselves in the data to understand the main discussion points around each PCI item. They listened to focus group recordings and read and re-read verbatim transcriptions and the notes made at each focus group. Researchers used the draft PCI as a basis of the framework and tabulated overall responses to each point on the PCI for each focus group. The data were synthesized by checking the framework chart against the original data sources and summarized to give a clear overall opinion of each focus group and to incorporate any suggested comments.
Fourth, the same panel of clinical specialists was asked to split the PCI into 4 domains by consensus: physical and functional well-being; treatment-related concerns; social care and well-being; and psychological, emotional, and spiritual well-being.
Phase II: pilot study of the rheumatology PCI
The PCI from phase I was piloted in a consultant-led general rheumatology clinic between July and December 2013. All clinic patients were eligible. The study design involved comparison of 2 different cohorts: 1 attending the clinic prior to the introduction of the PCI (pre-PCI) and the other attending after the introduction of the PCI (post-PCI).
Pre-PCI patients attended for their clinic appointment as usual and were not asked to fill in the PCI. An observer sat in on the clinical consultation and ticked items on the PCI that were discussed. The length of consultation was recorded. After the consultation, patients were asked to fill in a validated satisfaction questionnaire about the consultation33. Data regarding number and nature of referrals made and HAQ scores were also collected. Post-PCI, patients were asked to complete the PCI in the waiting room before their clinic appointment. Their responses were passed to the consultant before their consultation began. All items selected by these patients were then addressed.
The Mann-Whitney U test was used to compare pre- and post-PCI groups in the number of PCI concerns, the Likert-type questions on patient satisfaction, and for age, duration of illness, HAQ score, consultation length, and sex. The mean score of all patient-satisfaction questions was also compared. Fisher’s exact test was used to compare pre- and post-PCI groups in regard to sex, referral, and specific concerns. Spearman’s correlation coefficient (rs) was used to quantify the correlation between age, duration of illness, HAQ score, duration of consultation, number of PCI items, and patient satisfaction.
RESULTS
Phase I: development of a rheumatology-specific PCI
The first search (Supplementary data available from the authors on request) produced only 8 relevant papers11,34,35,36,37,38,39,40. The second produced many papers on HRQOL measures within rheumatology: most with only 1 HRQOL questionnaire, and then used only as a secondary outcome measure (supplementary data available from the authors on request). One review41 discussed the use of HRQOL tools in 109 rheumatology papers. We attempted to access all the HRQOL tools highlighted within this review.
The clinical specialist assessment of potential patient concerns from the literature search led to the generation of a list of 38 potential concerns. After discussions in the patient focus groups, a refined PCI was produced, comprising 39 items in 4 cognate domains (corresponding to other PCI).
Phase II: pilot study of the rheumatology PCI
Demographics and diagnoses for patients in pre- and post-PCI groups are shown in Table 1. Nineteen percent (10/54) of the pre-PCI and 24% (12/51) of the post-PCI group had newly diagnosed disease. Twenty-four percent (13/54) of the PCI group were diagnosed more than 10 years previously compared to 53% (27/51) of the post-PCI group. Pre-PCI patients had lower HAQ scores than those in the post-PCI group (Table 1). Median (IQR) duration of consultation without PCI was 8 min (5–14) and with PCI, 15 min (10–20). Two patients (4%) in the pre-PCI group required referrals to other specialties, whereas no post-PCI patient was referred (p = 0.50). Both groups lived with a variety of rheumatic conditions (Table 1).
Age, sex, duration of illness, diagnosis, duration of consultation, HAQ scores, and onward referral for the 2 groups of patients before and after the introduction of the Patient Concerns Inventory (PCI).
In the pre-PCI group, 335 concerns were raised from 50 patients [median (IQR) 5 (3–10) per patient], rising to 521 [9 (5–16)] from 51 in the post-PCI group (p = 0.002). This rise was predominantly from the physical and functional well-being and social care and well-being domains (Table 2). In the physical and functional well-being domain, the pre-PCI median (IQR) of 2 (0–4) and total of 140 concerns rose to a post-PCI median (IQR) of 5 (2–8) and total of 247 concerns (p < 0.001). Particular concerns after the PCI was introduced related to poor mobility, hand function, sleep, lack of energy, and range of joint movement. For the social care and well-being domain, the pre-PCI median (IQR) of 0 (0–1) and total of 16 concerns rose to a post-PCI median (IQR) of 1 (0–2) and a total of 71 concerns (p < 0.001). Particular concerns more often discussed with the PCI included difficulty in exercising, things to avoid, aids and adaptation/occupational therapy, and difficulty with/needing assistance with activities of daily living. For treatment-related concerns, there was little difference between pre- and post-PCI groups overall [both with median (IQR) of 2 (1–4) concerns] or in total number (123 and 128, p = 0.80). There was also no significant difference in the psychological, emotional and spiritual well-being domain, with a median (IQR) of 1 (0–2) concern and total number 56 pre-PCI and 75 post-PCI (p = 0.48). While after the introduction of the PCI there was more discussion regarding sexual relationships, difficulties with activities of interest, and enjoyment of life/loss of social activities, these were counterbalanced by less discussion about understanding of the patient’s illness.
Concerns discussed by patients, before and after the introduction of the Patient Concerns Inventory (PCI) to the clinic setting.
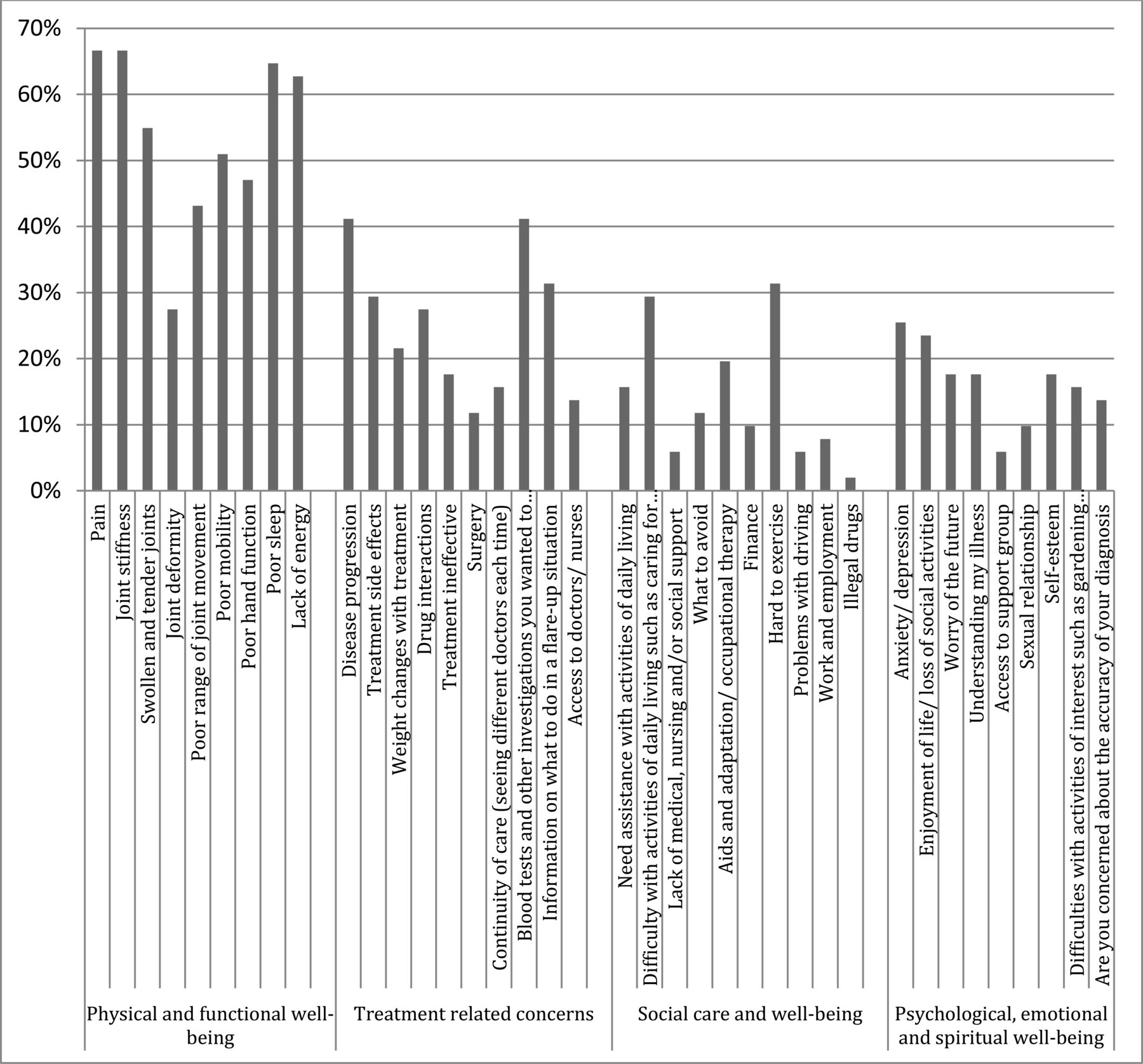
In the pre-PCI group, only pain was discussed with more than half of patients (Table 2, Figure 1). Infrequently discussed concerns (under 5%) were surgery; needing assistance with activities of daily living; lack of medical, nursing, and/or social support; things to avoid; aids and adaptation/occupational therapy; finance; difficulty in exercising; problems with driving; illegal drugs; enjoyment of life/loss of social activities; access to a support group; sexual relationship; and difficulties with activities of interest such as gardening and other activities. However, in the post-PCI group (Table 2, Figure 1), pain, joint stiffness, swollen and tender joints, poor mobility, poor sleep, and lack of energy were discussed with more than 50%, while only illegal drug concern was discussed with fewer than 5% of patients. The proportion of patients reporting each concern in the post-PCI group is detailed in Figure 1.
{kind=link}
Percentage of participants discussing each concern item in the post–Patient Concerns Inventory group.
The vast majority of patients rated their experience with their doctor in the consultation as being excellent or outstanding across all 11 questions both before and after the introduction of the PCI (Table 3). There were 9 consultations pre-PCI for which 1 or more of the responses to the 11 questions was less than very good compared to 7 post-PCI. Mean scores were slightly higher in the post-PCI group, though for none of the questions was there a statistically significant difference between the 2 sets of responses. The overall mean score across all 11 questions was also slightly higher [median (IQR) of 6.18 (5.45–7.00) pre-PCI and 6.41 (5.68–7.00) post-PCI (p = 0.65)].
Patient satisfaction.
Other analyses were performed to investigate the level of association between the baseline variables of age, sex, HAQ score, and duration of illness and length of consultation, patient satisfaction, and the number of PCI items. Both pre- and post-PCI groups were combined for these analyses. No statistical association was seen at p < 0.01 between any of these baseline variables and duration of consultation, nor between age or duration of illness with either the number of PCI items or with patient satisfaction. There was, however, significant correlation between HAQ score and number of PCI items, with higher HAQ scores tending to go with a greater number of PCI concerns in the physical and functional well-being (rs = 0.34, p = 0.004) and treatment-related concerns domains (rs = 0.27, p = 0.02) and total number (rs = 0.34, p = 0.003), but not with the other 2 domains (rs = 0.03 and rs = 0.00, respectively). There were also negative correlations of borderline significance with the patient satisfaction questions, ranging from rs = –0.28 to rs = –0.14, median rs = –0.25, and with the overall mean patient satisfaction score rs = –0.25, p = 0.05, indicating the tendency for higher HAQ scores to go with lower (worse) satisfaction scores. These correlations involving HAQ scores were generally weak, but because HAQ score seems to be a potential confounder to the comparisons made between pre- and post-PCI groups, the results were stratified (Table 4). The tendency remains toward having more PCI concerns post-PCI for HAQ scores between 0.50 and 0.99, for scores of 1.00 and above, and for when scores were not known, and there were too few scores below 0.50 in the post-PCI group to pass comment. There was also a consistent trend toward greater satisfaction post-PCI for HAQ scores 0.50–0.99 and of 1.00 and above.
PCI concerns and patient satisfaction before and after the introduction of the PCI, stratifying for HAQ score. Table shows mean (n) values.
Duration of consultation was also associated with a number of PCI items in 3 of the 4 domains and overall (rs = 0.36 overall, p < 0.001). There was a median of 5 concerns for consultations under 10 min, 7 when 11–19 min, and 10 when longer than 20 min. Among the baseline variables, sex was associated with HAQ scores (p = 0.001) and with females having lower HAQ scores (median 0.38 vs 0.88). Duration of illness was also associated with HAQ score, rs = 0.32, p = 0.006. Median HAQ score was 0.44 for duration 0–1 years, 0.75 for 2–9 years, and 0.88 for 10 or more years. Duration of illness was also associated with age, rs = 0.44, p < 0.001.
DISCUSSION
We have developed a novel instrument with potential utility across a wide range of rheumatological conditions. It is able to facilitate the identification of concerns that patients may have but perhaps are not able to raise with their clinician. Our data demonstrated that, despite the overall longer duration of illness and higher mean HAQ scores, patient satisfaction in the post-PCI group remained high. This may occur, in part at least, because patients in the post-PCI group asked significantly more questions and discussed a greater number of concerns compared to the pre-PCI group (Table 2). It has previously been demonstrated that patient satisfaction increases significantly when interventions are designed to encourage patients to ask questions42. The fact that the baseline patient satisfaction in this clinic was so high meant that it was not practical to detect significant changes in satisfaction after implementation of the PCI. It is now under evaluation across other clinics.
Although the mean duration of consultation increased slightly post-PCI, it is important to remember that the PCI identified a significantly higher number of items of unmet need, mainly from the physical and functional well-being and the social care and well-being domains (Table 2). This was because PCI provided patients the opportunity to discuss potential problems such as sexual relationships, difficulties with activities of interest, and enjoyment of life and loss of social activities, among others — important concerns that patients had previously been unable to discuss. Part of the problem might lie in the patients’ perceived acceptability of asking certain questions. It appears to become easier for patients when potential specific concerns are presented on a checklist, reassuring patients that it is appropriate to ask such questions.
There are a number of potential limitations to our study. While we took great pains to devise a list of concerns from a literature search, expert opinion, and focus groups, it is possible that important potential concerns were missed. This can be addressed as the tool is used more widely. We also evaluated the instrument in only 1 clinic. However, the number of patients studied was sufficient to detect the initial changes that we set out to evaluate and to determine whether it was an appropriate tool to roll out further. There were also advantages of consistency if initial studies used only 1 clinician. Finally, the difference in disease duration between the 2 groups might have potentially led to a difference in needs. Indeed, understanding possible changes of needs with time is a focus for future work with this tool.
The PCI provides an opportunity to improve doctor-patient communication, serving as a visual aid for both doctors and patients and providing a novel and powerful tool for holistic needs assessment in the rheumatology clinic, where it can highlight important areas of unmet need. Our study demonstrates that, with the use of the PCI, patients are able to discuss significantly more important concerns that would otherwise go unrecognized when the traditional consultation style is used. While rheumatologists may not be able to deal with all the concerns during the same appointment, this should prompt appropriate referrals with suitable followup to ensure that the concerns are adequately addressed.
Footnotes
Supported by the Aintree Arthritis Trust.
- Accepted for publication December 23, 2015.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.