
The sternoclavicular joint is a diarthrodial joint that can be involved in rheumatoid arthritis (RA), and is detectable by ultrasound (US) examination in 15% of patients with RA1. Methotrexate-related lymphoproliferative disorder (MTX-LPD) occurs in extranodal sites in about 40%–50% of the affected patients2; however, intraarticular MTX-LPD is a very rare manifestation with only 1 case report occurring in the knee joint3.
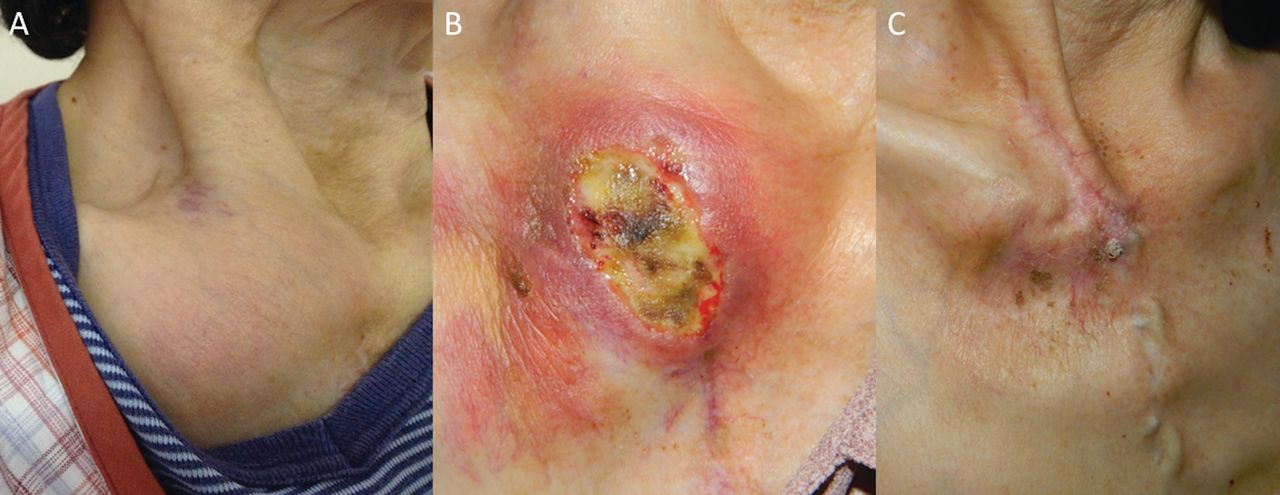
A 67-year-old Japanese woman with a 40-year history of RA, treated with MTX (6 mg/week) for 15 years, presented to our hospital complaining of right sternoclavicular joint swelling (Figure 1A). The serum levels of C-reactive protein (5.68 mg/dl, normal < 0.3), lactate dehydrogenase (325 IU/l, normal 125–237), and soluble interleukin 2 receptor (1340 U/ml, normal 145–519) were elevated. US examination of the swelling joint showed low echoic lesion accompanied with positive power Doppler. Sternoclavicular joint synovitis was suspected, and MTX was increased to 8 mg/week, resulting in the worsening of this joint lesion (Figure 1B). Skin biopsy of the ulcerated lesion revealed CD20+ atypical lymphocytes with Epstein-Barr virus (EBV) latent membrane protein 1 and EBV-encoded RNA-1 (Figure 2). The diagnosis of MTX-LPD associated with EBV was made. The sternoclavicular joint swelling disappeared 6 months after MTX discontinuation (Figure 1C).
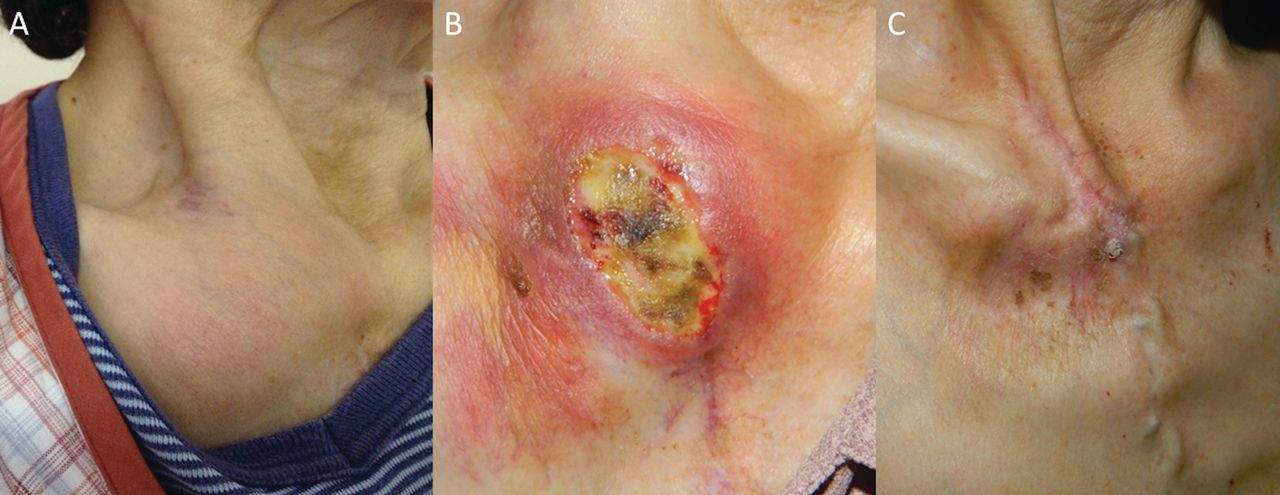
A. Right sternoclavicular joint swelling appeared during the course of RA treated with MTX. B. Increasing the dose of MTX caused ulceration of the sternoclavicular joint swelling. C. Discontinuation of MTX led to improvement of the lesion. RA: rheumatoid arthritis; MTX: methotrexate.

{kind=link}
{kind=link}
Skin biopsy of the sternoclavicular joint ulcer showed CD20+ atypical lymphocytes with LMP-1 and EBER-1. LMP-1: Epstein-Barr virus latent membrane protein 1; EBER-1: Epstein-Barr virus-encoded RNA-1.
This sternoclavicular joint swelling is suggested to be caused by MTX-LPD in the skin overlapping a joint. Mucocutaneous ulcer associated with EBV-positive LPD can develop during immunosuppressive therapy, including MTX4. MTX-LPD should be considered as the differential diagnosis of atypical joint swelling during the course of RA, and histopathologic examination should be carried out.
REFERENCES
- 1.
- 2.
- 3.
- 4.