
Abstract
Objective. To retrospectively assess changes in disease activity and skeletal damage in children with chronic nonbacterial osteomyelitis (CNO) after infliximab and methotrexate, with or without zoledronic acid or nonsteroidal antiinflammatory drug (NSAID) monotherapy, using a standardized magnetic resonance imaging (MRI) approach.
Methods. Treatment-related changes in clinical and MRI measures from aggressive therapy and NSAID monotherapy groups (n = 9 per group) were evaluated using nonparametric methods.
Results. Pain, physical function, physician global assessment, inflammatory markers, nonvertebral inflammatory lesion number, and maximum bone edema score all improved significantly with aggressive therapy (p < 0.03), whereas only the maximum soft tissue inflammation severity decreased (p = 0.02) with NSAID monotherapy. Vertebral deformities and physeal damage did not worsen in the aggressive therapy group but 1 in the NSAID group had worsening of growth plate damage.
Conclusion. An aggressive treatment regimen in CNO improved clinical and imaging measures of disease activity without progression of skeletal damage.
- CHRONIC NONBACTERIAL OSTEOMYELITIS
- METHOTREXATE
- NONSTEROIDAL ANTIINFLAMMATORY DRUGS
- ZOLEDRONIC ACID
- MAGNETIC RESONANCE IMAGING
- INFLIXIMAB
Chronic nonbacterial osteomyelitis (CNO) is an inflammatory bone disease that causes skeletal inflammation and pain, and can be complicated by functional impairment, vertebral fractures, and limb length discrepancy. Although treatment with nonsteroidal antiinflammatory drugs (NSAID) relieves pain in some patients1,2,3,4,5, those at risk for skeletal deformities or with persistent pain require additional therapy with tumor necrosis factor−α inhibitors (TNFi)1,3,6,7,8 or bisphosphonates4,9,10,11,12, 13,14,15,16.
CNO treatment studies have focused on clinical, laboratory, and radiographic improvements. Magnetic resonance imaging (MRI) is useful to assess active bone and soft tissue edema, periosteal reaction, and hyperostosis, as well as components of skeletal damage, including physeal bony bar formation and vertebral collapse. Previous MRI-based studies have not examined specific lesion characteristics, mainly reporting the change in the number of lesions and qualitative bone marrow enhancement improvement2,7,8.
In our practice, TNFi therapy is used for patients with active vertebral disease or CNO-related persistent pain despite NSAID or other nonbiologic disease-modifying therapy. Additionally, MRI is performed at diagnosis to identify individuals with vertebral involvement, who are offered a single dose of bisphosphonate therapy with zoledronic acid (ZOL), with maintenance infliximab (IFX) therapy and concomitant methotrexate (MTX). Our retrospective study aimed to evaluate changes in clinical and MRI characteristics of CNO in children treated with an aggressive therapy including IFX and MTX, with or without ZOL, and those treated with NSAID monotherapy. Our hypothesis was that aggressive therapy would improve pain, physical function, and MRI characteristics of disease activity, and prevent progression of skeletal damage.
MATERIALS AND METHODS
Participants
Patients treated for CNO in the Division of Rheumatology at The Children’s Hospital of Philadelphia (USA) from 2006–2013 and 2–18 years of age at diagnosis were identified. Two pediatric rheumatologists (YZ and JMB) confirmed the CNO diagnosis if unifocal or multifocal inflammatory bone lesions were present without evidence of malignancy or infection according to laboratory tests and histologic examination, if performed1. Patients were included if regional or whole body MRI (WBMRI) scans contained multiplanar fluid-sensitive sequences and were conducted at most 2 months prior to and at least 2 months after IFX initiation or NSAID therapy. Exclusion criteria included the coexistence of a condition associated with bone lesions, or motion-degraded MRI studies. The Institutional Review Board approved the study.
Measures
Demographic, clinical, and laboratory data were abstracted from the medical record. Pain, patient and physician’s global assessment (PGA), Childhood Health Assessment Questionnaire (CHAQ) score17, complete blood cell count, erythrocyte sedimentation rate (ESR, mm/h) and C-reactive protein (CRP, mg/dl) levels were assessed at encounters nearest to the relevant MRI evaluations. Paired regional or WBMRI scans were evaluated before and after treatment by a pediatric radiologist (NAC). WBMRI sequences included coronal short-tau inversion recovery (STIR) of the entire body including all extremities, axial T2 fat-saturated images through the chest, abdomen, and pelvis, and sagittal STIR images of the spine. Regional focused MRI scans included multiplanar fluid–sensitive sequences.
In scoring the MRI, bone edema was defined as increased bone marrow signal intensity, soft tissue inflammation as increased signal intensity within perilesional soft tissues adjacent to the bony cortex, periosteal reaction as separation of the periosteum from the cortex, hyperostosis as new bone formation at lesion sites, vertebral compression as decreased height of a vertebral body compared with adjacent vertebral bodies, and growth plate abnormalities as either loss of the normal trilaminar appearance or premature growth arrest with consequent bony bar development in skeletally immature patients. A bony bar was defined as an abnormal osseous connection between the epiphysis and metaphysis seen in skeletally immature patients18. Arthritis was defined as thickening of the synovium with an abnormal joint effusion.
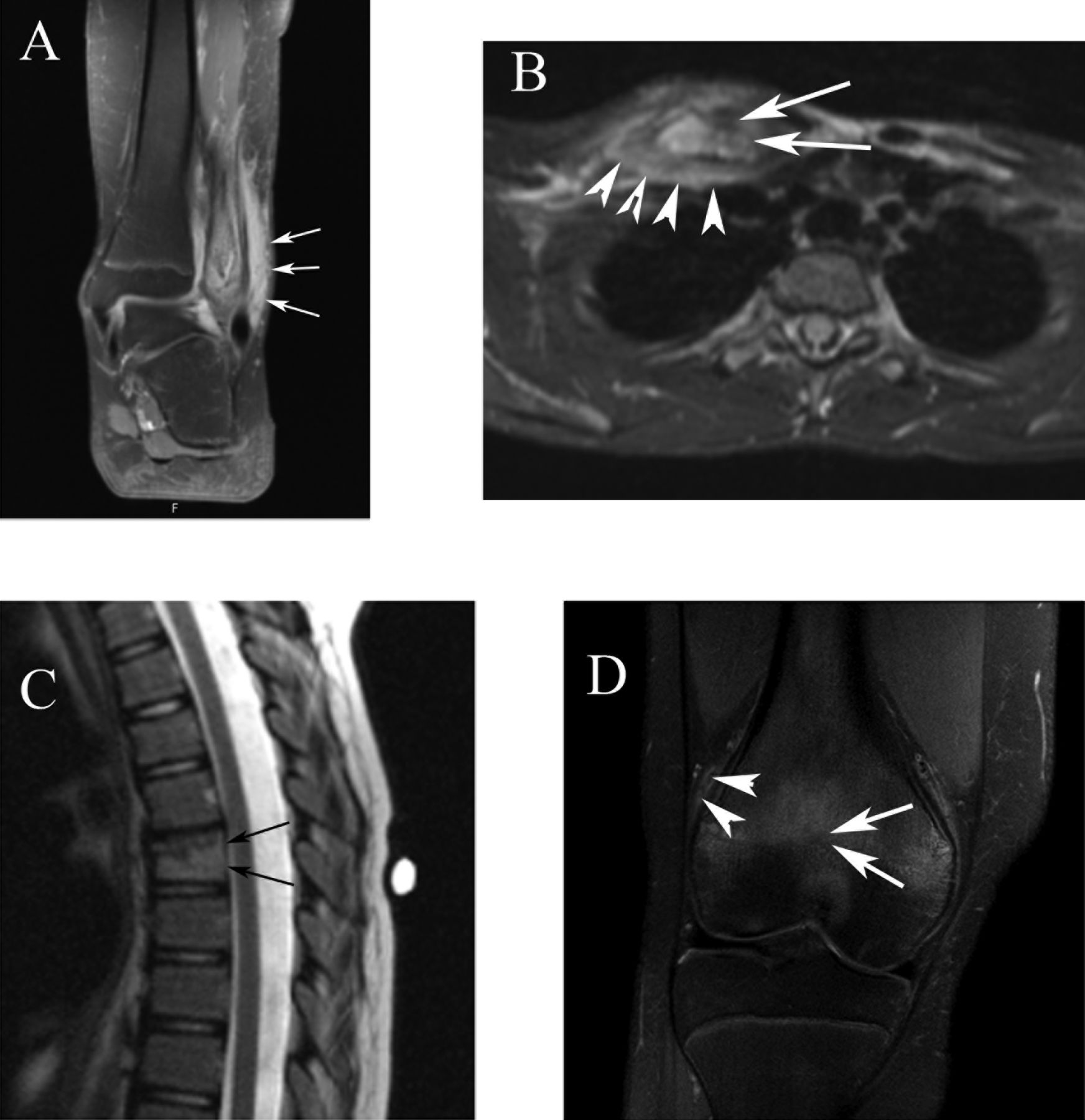
Bone edema and soft tissue inflammation severity were categorized based on the percentage of involved bone or soft tissue volume as none (0), mild (1: < 25%), moderate (2: 25–50%), or severe (3: > 50%). Periosteal reaction, hyperostosis, and arthritis were categorized as absent or present. Long bone growth plates were categorized as normal (0), with physeal irregularity (1), or complete bony bar (2). Vertebral compression was categorized as none (0), partial (1), or complete (2). To systematically assess abnormalities at skeletal sites, anatomic regions were defined (Appendix 1). For the assessment of MRI characteristics, records were kept of the number of unique inflammatory lesions, maximum bone edema severity, total lesion number with periosteal reaction, total lesion number with hyperostosis, maximum bony bar severity, maximum vertebral compression severity, maximum soft tissue inflammation severity, and the number of joints with arthritis. Representative MRI images to illustrate each characteristic are shown in Figure 1.
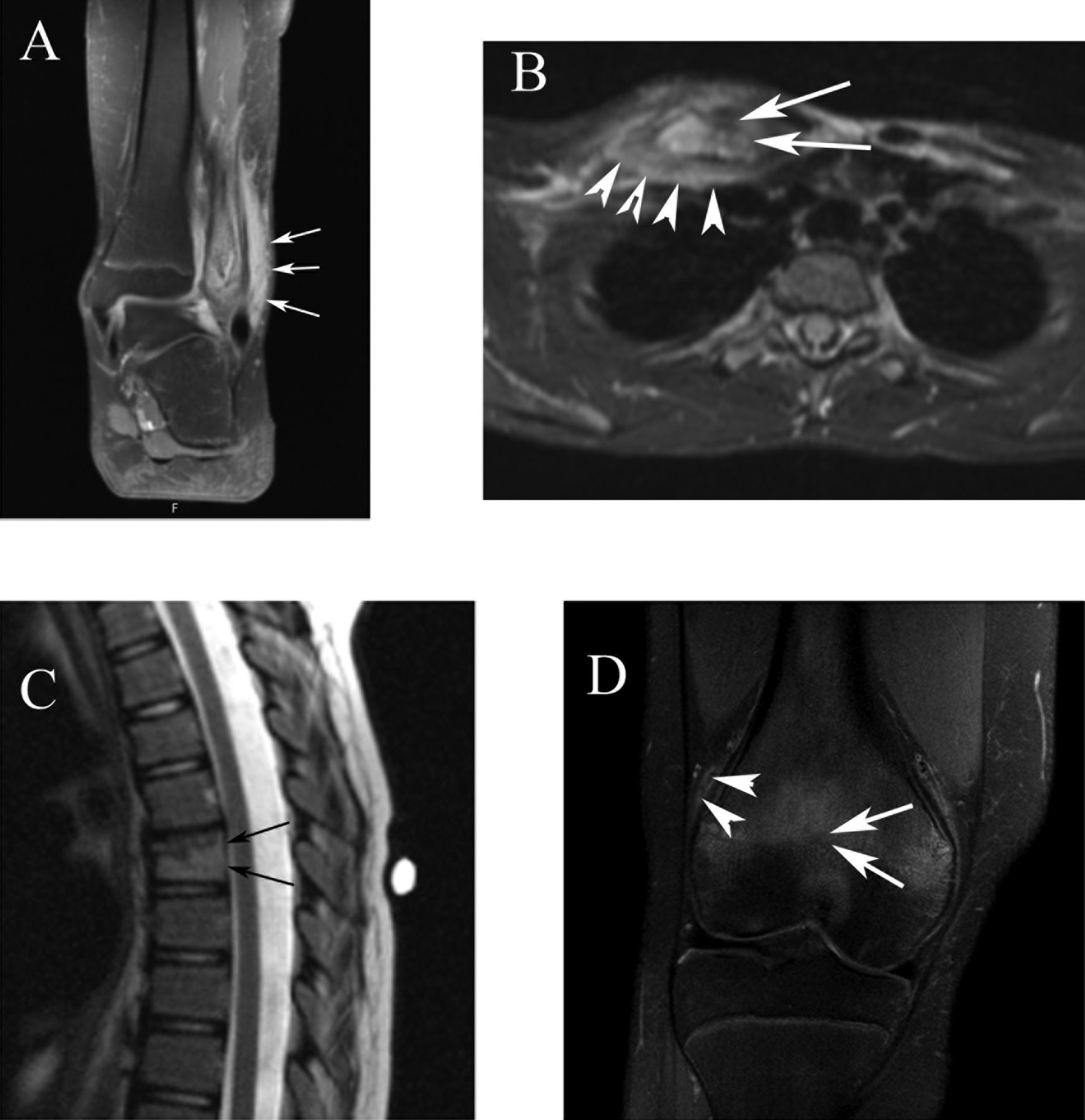
Representative images and grading of bone edema, soft tissue inflammation, hyperostosis, vertebral compression, and growth plate bony bar. A. Severe bone marrow edema (affecting > 50% of bone volume) of the distal fibula with severe adjacent soft tissue inflammation (arrows; affecting > 50% of adjacent soft tissue volume). B. Severe bone marrow edema and hyperostosis (arrows; new bone formation at lesion site) of the right clavicle with adjacent soft tissue edema (arrowheads). C. Severe bone marrow edema of a thoracic vertebral body with partial compression as demonstrated by loss of vertebral body height (arrows) compared with adjacent vertebral bodies. D. Complete bony bar (arrows; obliteration of the distal femoral physis and continuous marrow signal seen between the metaphysis and physis) with mild bone marrow edema and mild soft tissue inflammation (arrowheads; affecting < 25% of soft tissue volume). A normal physis is seen within the proximal tibia.
The statistical analysis was performed using Stata 11.0 (StataCorp.). Patient demographic and disease characteristics were summarized using standard descriptive statistics. The changes in clinical, laboratory, and MRI outcome measures were analyzed using nonparametric Wilcoxon matched pairs signed-rank test.
RESULTS
Demographic and clinical characteristics of the aggressive therapy and NSAID groups are summarized in Table 1. Eighteen patients with CNO met inclusion criteria, of whom 9 received aggressive therapy and 9 received NSAID monotherapy. In the aggressive treatment group, all received IFX and concomitant MTX, and 6 additionally received ZOL. Seven previously received a combination of antibiotics, NSAID, prednisone, bisphosphonate, and MTX prior to the IFX initiation. Aggressive therapy was instituted for persistent disease (n = 5) or vertebral lesions (n = 4). The median duration between diagnosis and IFX initiation was 3.4 months (range: 0.5–19.3) overall and 6.7 months for the persistent-disease subset. In the aggressive therapy group, the baseline and followup MRI scans were obtained at 0.9 months (range: 0.3–2.2) prior to and 5.9 months (range: 2.6–13.4) after IFX initiation, respectively. Paired-site specific MRI were obtained in 6 and paired WBMRI in 3 individuals.
Baseline demographic, clinical, and laboratory characteristics in CNO at initiation of infliximab or NSAID. Continuous variables expressed as median (range).
The mean IFX dose was 8.1 ± 1.9 mg/kg, given at baseline, 2 weeks, and every 4 weeks thereafter in 8 patients and every 8 weeks in one. The median weekly MTX dose was 22.5 mg (range 5–25) or 0.4 mg/kg (range 0.1–1). The median ZOL dose was 1.5 mg (range: 0.63–3) or 0.037 mg/kg (range 0.025–0.05) for a single dose within 2 months of initiation of IFX. One received a dose 9 months prior to IFX. The numbers of patients with lesions at specific sites were spine (4), pelvis (6), clavicle (2), long bones (4), and mandible (1). Significant decreases of the following outcomes occurred after IFX and MTX initiation: pain score (p = 0.008), patient global assessment (p = 0.007), PGA (p = 0.008), CHAQ score (p = 0.02), ESR (p = 0.01), and CRP (p = 0.03; Table 2). Median reductions in the nonvertebral lesion number (p = 0.03) and the maximum bone edema score (p = 0.02) were significant. The maximum soft tissue inflammation score and inflamed joint count decreased non-significantly. Periosteal reaction and hyperostosis resolved in 2 and 1 affected patients, respectively. Growth plate irregularities resolved in 2 of 3 patients. Bony bar formation and vertebral compression did not worsen in any patient. Representative MRI images before and after treatment are shown (Figure 2).

{kind=link}
{kind=link}
Representative MRI images from a 10-year-old girl with CNO and left jaw pain. Axial (A) and coronal (B) fluid-sensitive images through the mandible demonstrate severe bone marrow edema (affecting > 50% of bone volume) within the ramus of the left mandible (*) with periosteal reaction (thin arrows; separation of the periosteum from the cortex) and severe adjacent soft tissue edema (arrowheads; affecting > 50% of soft tissue volume). The remainder of the mandible is normal. Axial (C) and coronal (D) fluid-sensitive images 1 year later, after aggressive treatment with methotrexate and infliximab, demonstrate resolved periosteal reaction and soft tissue edema. There is remodeling of the left mandibular ramus with mild expansion and residual bone marrow edema (arrows; affecting < 25% of bone volume).
Changes in clinical outcomes, inflammation markers, and MRI characteristics after infliximab and methotrexate treatment or NSAID monotherapy. Variables are expressed as median (range) unless otherwise noted.
In the NSAID monotherapy group, naproxen, diclofenac, meloxicam, and indomethacin were prescribed in 4, 4, 3, and 8 patients, respectively. The baseline MRI was obtained a median of 0.5 months (range 0–1.3) prior to NSAID initiation and the followup MRI was obtained a median of 7.3 months (range 2.8–31.8) after NSAID initiation. Paired-site specific MRI scans were obtained in 7 and paired WBMRI in 2 individuals. The numbers of patients with lesions at specific sites were spine (3), pelvis (6), and long bone (8). No patient had mandible or clavicle involvement. The majority of these patients was treated prior to our adopting an aggressive regimen or deferred additional therapies by family. At the visit closest to the followup MRI, these measures did not decrease among patients with complete data: median pain (n = 4), patient global assessment (n = 3), PGA (n = 5), CHAQ scores (n = 4), ESR (n = 9), and CRP (n = 8). No improvement was observed in the number of unique lesions, nonvertebral lesions, or vertebral lesions, or in the maximum edema score. However, the median decrease in the maximum soft tissue inflammation severity was significant (p = 0.03). Periosteal reaction resolved in all 3 patients (p = 0.08). Among 3 patients with growth plate abnormalities, 1 progressed from physeal irregularity to a complete bony bar. One patient with minimal vertebral compression showed improvement in the appearance of the involved vertebra at followup.
DISCUSSION
CNO can be a painful, disabling condition but unfortunately, no guidelines exist to assist clinicians when choosing a treatment plan according to disease severity and the risk of skeletal damage. Because of the lack of randomized control trials, treatment is empirical. A stepwise strategy was proposed, suggesting NSAID initially, with more intensive treatment reserved for severe cases, including those with structural damage19. TNFi1,3,4,6, MTX1,7, and bisphosphonate therapy4,9,10,11,12,13,14,15,16 result in symptom relief in selected patients, and our approach is to use IFX for persistent disease or vertebral involvement, with MTX used mainly to prevent human antichimeric antibody formation. Although etanercept may be effective in CNO, we have had etanercept failures, and so we instead used IFX in our study. It is possible that adalimumab would have been as effective as IFX20. Additionally, a single dose of ZOL was given to diminish bone resorption and possibly further diminish inflammation in patients considered at risk for vertebral compression fractures or persistent pain despite at least 2 IFX infusions. ZOL is a nitrogenous bisphosphonate that has been used in osteogenesis imperfecta21,22, and is about 100 times more potent than pamidronate. While not designed to demonstrate the effectiveness of a single agent, this treatment regimen resulted in clinical and MRI-defined improvement in a severely affected subset of patients without progression of skeletal damage.
Our results are consistent with previous reports1,3,6,7,8 that TNF inhibition resulted in clinical symptom relief and imaging improvement, and our study is the largest to date. The mechanism remains unclear. Findings of impaired interleukin 10 expression but unchanged TNF-α and interleukin 6 expression from monocytes in patients with CNO23 suggest a possible restored balance between proinflammatory and antiinflammatory cytokines in patients with CNO treated with TNFi. It is possible that the concomitant use of MTX and ZOL may have contributed to the favorable response. In a large US cohort study (n = 70), MTX, TNFi, and corticosteroid were shown superior to NSAID1. Pamidronate is commonly used to treat CNO4,9,10,11,12,13,14,15,16 and has shown efficacy when given 3 days every 3 months or once a month. In a comprehensive assessment using WBMRI, the majority of CNO lesions improved after 1 year of pamidronate; however, 2 new lesions developed during the treatment15. ZOL has never been used in CNO but demonstrates similar bone density improvements to pamidronate in osteogenesis imperfecta22. Our study is the first, to our knowledge, to use ZOL in CNO, and its primary role in our study was as adjunctive therapy. After a median of 6 months, there was no worsening of vertebral shape. Our observation is consistent with a report that pamidronate reduced pain in children with vertebral disease, but vertebral shape was unlikely to improve over about 13 months12. Our observation duration is probably too short to determine the longterm effect of ZOL on preventing vertebral compression fractures. A comparative study between bisphosphonate and TNFi is necessary to determine the relative effectiveness from each agent and is beyond the scope of our study.
In contrast, we found mixed imaging results with NSAID monotherapy. The NSAID group had baseline MRI characteristics and inflammatory markers similar to those of the aggressive treatment group (data not shown). Clinical and functional scores suggested a suboptimal clinical response in the NSAID group, which was reflected in the lack of improvement in lesion number and maximum edema score. These patients from the NSAID group were treated largely before our aggressive regimen protocol was developed; 3 patients with spinal lesion were not treated with TNFi or ZOL. Although soft tissue inflammation decreased and periosteal reaction resolved, the maximum bone edema score and the total number of inflammatory lesion sites did not change. Additionally, 1 patient with growth plate irregularity progressed to a complete bony bar. The decreased soft tissue inflammation and periosteal reaction are consistent with a therapeutic effect, but not enough to result in overall clinical improvement.
It is not known which MRI characteristics are reliably assessed and most sensitive to change, and how each relates to other clinical assessment tools in CNO. No imaging method to assess disease activity and damage in CNO has currently been validated. One study proposed a CNO score including the MRI-based lesion number, ESR, physician and patient/parent global assessment, and CHAQ score2. It is possible that our method complements that of Girschick, et al5 by defining degrees of bone edema according to skeletal site, periosteal reaction, hyperostosis, soft tissue inflammation, and damage metrics such as vertebral deformities and physeal irregularities. That bone edema, pain, and functional limitation improved in those patients in the aggressive therapy group suggests that the severity of bone edema should be monitored and used as part of an assessment tool. Bone edema is most likely reversible and responsive to the antiinflammatory treatment based on our study. Additionally, a standardized skeletal damage assessment should be part of any longitudinal study in CNO as an outcome measurement. Future studies should define how to incorporate MRI characteristics into a scoring system to evaluate disease activity and damage progression in clinical trials.
There are limitations in our study to be considered. First, the retrospective nature of the study makes it prone to selection bias, particularly for the NSAID-only group, in which patients were included if additional imaging was required. However, selection bias in the NSAID group does not alter our findings in the patients receiving aggressive therapy. Second, the observation period is relatively short for determining the longterm effect of treatment on skeletal damage. Third, only a few patients had whole body MRI, so the occurrence of new asymptomatic lesions cannot be determined. However, if a patient has vertebral lesions, our practice is to perform followup MRI scans of the entire spine. Additionally, the clinical relevance of asymptomatic lesions in the appendicular skeleton is unknown. Fourth, our MRI scoring tool will need further validation in a prospective study.
An aggressive treatment regimen of IFX and MTX with or without ZOL in CNO improved clinical and imaging measures of disease activity without progression of skeletal damage. Future studies are needed to further develop appropriate outcome measures and identify therapies that protect skeletal development and optimize pain control.
Acknowledgment
We thank Jenna Tress for her assistance throughout this project.
Appendix
APPENDIX 1. Anatomic sites used in the MRI assessment of CNO disease activity and damage.
- Accepted for publication March 17, 2015.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.