
Abstract
Objective. Rapidly progressive interstitial lung disease (RP-ILD) is an intractable and fatal complication of juvenile dermatomyositis (JDM). This study evaluated serum levels of B cell activating factor (BAFF) and a proliferation-inducing ligand (APRIL) in JDM patients with complicating ILD, and their association with ILD phenotypes, clinical variables, and anti-melanoma differentiation-associated gene 5 (MDA5).
Methods. We measured the levels of BAFF, APRIL, and anti-MDA5 in the sera of 23 JDM patients with ILD [8 in the RP-ILD group and 15 in the chronic ILD (C-ILD) group], 17 JDM patients without ILD (non-ILD group), and 10 age-matched controls, using the ELISA method. ILD was identified by high-resolution computed tomography.
Results. Serum BAFF titers were significantly higher in the JDM patients with RP-ILD versus those with C-ILD (p = 0.011) and in healthy controls (p = 0.0004). The C-ILD group had significantly higher levels of BAFF versus controls (p ≤ 0.0001). Serum APRIL was markedly elevated in the RP-ILD group as compared with the C-ILD group (p = 0.003) and controls (p = 0.006). In patients with ILD, both BAFF and APRIL levels were correlated with serum Krebs von den Lungen-6 and interleukin 18. Subjects with high titer anti-MDA5 (> 200 U) had higher levels of BAFF and APRIL than those with low titer anti-MDA5 (< 100 U; p = 0.019 and p = 0.0029, respectively), which may have been due to a relationship between RP-ILD and high anti-MDA5 titer.
Conclusion. Our findings of markedly elevated levels of BAFF and APRIL in patients with RP-ILD JDM suggest the potential importance of these cytokines in the diagnosis and treatment of RP-ILD accompanying JDM.
- B CELL ACTIVATING FACTOR
- PROLIFERATION-INDUCING LIGAND
- ANTI-MDA5
- JUVENILE DERMATOMYOSITIS
- INTERSTITIAL LUNG DISEASE
Juvenile dermatomyositis (JDM) is a childhood-onset autoimmune inflammatory myopathy characterized by skin rashes and muscle weakness. JDM prognosis was poor before the introduction of corticosteroid therapy, with death occurring in one-third of patients1. Although the mortality rate has since decreased to 0.7–3.1% with combination therapy of corticosteroids and immunosuppressants2,3,4, our recent nationwide survey revealed that mortality in JDM remained higher than in other juvenile rheumatic diseases in Japan and that the major cause of death was rapidly progressive interstitial lung disease (RP-ILD)5.
It was reported that differences in clinical DM phenotypes among several myositis-specific autoantibodies (MSA) indicated a role of autoantibodies in DM pathogenesis6. Autoantibodies to melanoma differentiation-associated gene 5 (MDA5), which is found in 10–20% of Asian patients with adult-onset DM, have been correlated with both clinically amyopathic disease and a high incidence of ILD, particularly RP-ILD7,8,9,10,11. Similarly to adult cases, we have uncovered a relationship between anti-MDA5 titer and ILD severity in patients with JDM5,12, suggesting a critical role of anti-MDA5 in the development of JDM-associated ILD.
B cell activating factor (BAFF) and a proliferation-inducing ligand (APRIL) are important physiological mediators of B cell homeostasis and play important roles in the production of antibodies. Both cytokines are expressed by myeloid lineage cells such as macrophages, monocytes, and dendritic cells, and at lower levels by T cells13. Serum levels of BAFF and APRIL are reportedly increased in several autoimmune diseases such as systemic lupus erythematosus (SLE), Sjögren syndrome (SS), multiple sclerosis, and systemic sclerosis (SSc), and elevated BAFF alone was reported in ANCA-associated renal vasculitis, Grave disease, autoimmune pancreatitis, and myasthenia gravis14. In particular, elevated BAFF is associated with the presence of disease-specific autoantibodies such as anti-SSA in SS, anti-dsDNA in SLE, and anti-histone in SSc15,16,17,18. Moreover, a prominent role of BAFF in the development of autoimmune diseases has been supported by the therapeutic effects invoked by BAFF antibodies in SLE and RA19,20.
Elevated levels of BAFF in the serum and in muscle tissue have also been reported in patients with idiopathic inflammatory myopathy (IIM)6,21,22, and BAFF titer was associated with the presence of autoantibodies and disease activity scores of myositis6,21. However, because the roles of BAFF and APRIL in patients with ILD accompanied by JDM remain unclear, our present study measured the serum levels of these mediators in patients with JDM-associated ILD and examined for associations with clinical course, disease variables, anti-MDA5 titer, and treatment.
MATERIALS AND METHODS
Patients and controls
Our present study was approved by the ethics committee of Shinshu University, according to the Declaration of Helsinki. We enrolled 24 JDM patients with ILD (ILD group), including 9 patients with RP-ILD (RP-ILD group) and 15 patients with chronic ILD (C-ILD group), 17 JDM patients without ILD (non-ILD group), and 10 age-matched healthy controls. The clinical records, routine laboratory data, and serum samples of the ILD group were collected from 12 centers across Japan, while those of the non-ILD group were obtained at Shinshu University Hospital and Aichi Children’s Health and Medical Center. One patient in the RP-ILD group was excluded because he was found to have Pneumocystis pneumonia. That left 8 patients in RP-ILD group. All patients were diagnosed as having JDM prior to 16 years of age. JDM diagnosis was made according to the criteria of Bohan and Peter23,24 for dermatomyositis or that of Gerami, et al for clinically amyopathic dermatomyositis25 with some modification, whereby a disease duration for 6 months or longer was excluded because most of the subjects with ILD required prompt systemic corticosteroid and immunosuppressive drug treatment within 6 months of disease onset. ILD was diagnosed using high-resolution computed tomography (HRCT) of the lungs. RP-ILD was defined as ILD rapidly worsening within 3 months of symptom onset or at the time of ILD diagnosis. C-ILD patients included those with apparent ILD without any respiratory symptoms who responded to immunosuppressive therapy or those with slowly progressive ILD over a 3-month period.
The clinical characteristics of patients at the time of ILD diagnosis or at JDM diagnosis for patients without ILD are shown in Table 1. A total of 5 patients succumbed to ILD-related respiratory distress.
Clinical and laboratory data of patients with and without ILD. Values represent the median (interquartile range) or number (percentage) unless otherwise indicated.
Evaluation of clinical laboratory variables and serum BAFF, APRIL, and anti-MDA5 levels
Serum samples were obtained at the time of ILD diagnosis or at JDM diagnosis for the non-ILD group, divided into aliquots, and stored between −20°C and −40°C until analysis. Routine laboratory tests included measurement of serum levels of creatine phosphokinase (CK), aspartate transaminase (AST), alanine transaminase, aldolase, ferritin, Krebs von den Lungen–6 (KL-6), antinuclear antibodies, and anti-Jo1. Two of 8 patients in the RP-ILD group and 5 of 15 patients in the C-ILD group had already been treated for JDM with methylprednisolone pulse therapy (25–30 mg/kg/day for 3 days) followed by high-dose corticosteroids (maximum dose: 1–2 mg/kg/day) at the time of ILD diagnosis. The sera of 8 patients (5 with RP-ILD and 3 with C-ILD) were also available after completion of treatment (Supplementary Table, available at jrheum.org). Serum levels of BAFF (R&D Systems), APRIL (eBioscience), and IL-18 (MBL) were measured by ELISA according to the manufacturers’ protocols. Anti-MDA5 was also measured using ELISA as described10,26, whereby the number of antibody units was calculated from optical density results at the 450 nm (normal range: < 8 U) using a recombinant MDA5 antigen.
Statistical analysis
We performed all statistical analyses using JMP 9 software (SAS Institute). Unpaired data were analyzed with the nonparametric Wilcoxon test. Paired data were examined by the Wilcoxon signed-rank test. Correlations were assessed using Spearman’s rank-order test (rs). A p value < 0.05 indicated statistical significance.
RESULTS
Serum levels of BAFF and APRIL at the time of diagnosis of ILD
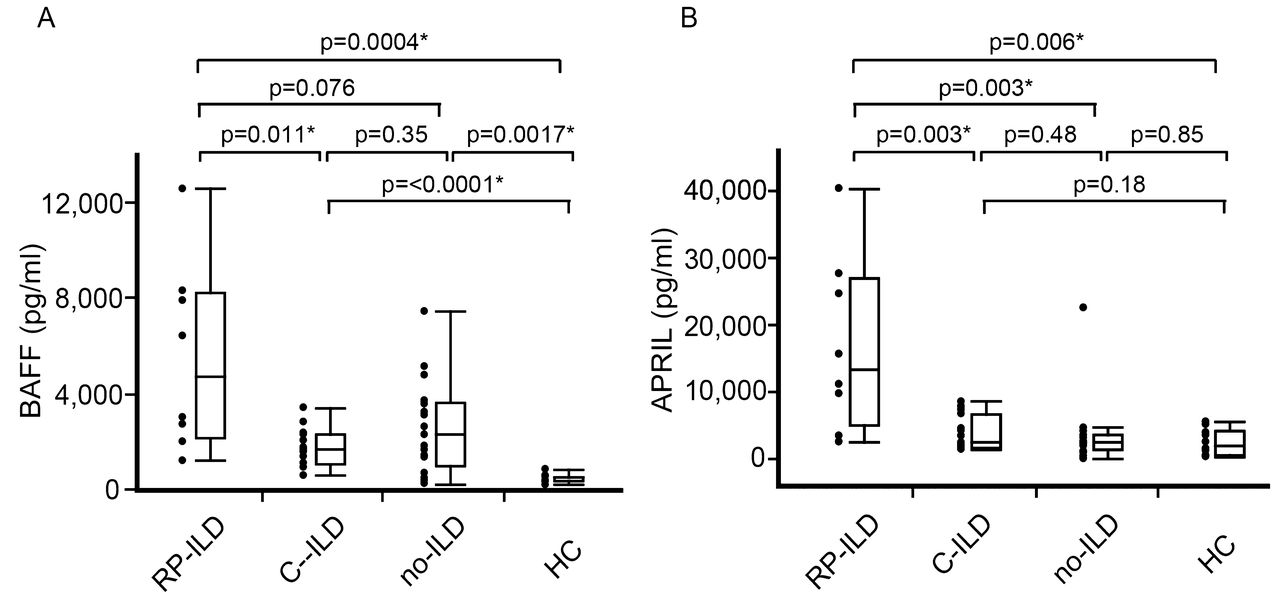
Figure 1 presents the BAFF levels in the 2 ILD subgroups (RP-ILD and C-ILD) and the non-ILD group. Both the RP-ILD [median 4734 pg/ml, interquartile range (IQR) 2198–9219 pg/ml] and C-ILD (median 1721 pg/ml, IQR 1122–2315 pg/ml; p = 0.011) groups had higher levels of BAFF in comparison with the control group (median 534 pg/ml, IQR 361–582 pg/ml; p = 0.0004 and p ≤ 0.0001, respectively). BAFF levels also tended to be higher in the non-ILD group (median 2310 pg/ml, IQR 1036–3662 pg/ml) than in healthy controls (p = 0.0017). Although patients with RP-ILD had significantly higher circulating BAFF levels than did C-ILD patients (p = 0.011), there were no remarkable differences between the RP-ILD group and the non-ILD group (p = 0.076) or the C-ILD group and the non-ILD group (p = 0.35).

Serum BAFF and APRIL levels in patients with juvenile dermatomyositis (JDM) with interstitial lung disease (ILD). Those with ILD are divided into rapidly progressive ILD (RP-ILD) and chronic ILD (C-ILD). Other categories are patients without ILD (no-ILD), and healthy controls (HC). The horizontal line within boxes represents the median, the upper and lower boundaries of the boxes represent the 75th and 25th percentiles, respectively, and the top and bottom whiskers represent the 95th and 5th percentiles, respectively. Dots represent individual patient cytokine values. Significant differences are indicated by asterisks. BAFF: B cell activating factor; APRIL: a proliferation-inducing ligand.
Serum levels of APRIL were significantly elevated in the RP-ILD group (median 13,350 pg/ml, IQR 4975–26,850 pg/ml) as compared with the C-ILD group (median 2400 pg/ml, IQR 1600–6700 pg/ml; p = 0.003), non-ILD group (median: 2500 pg/ml, IQR 1300–3475 pg/ml; p = 0.003), and healthy controls (median: 2000 pg/ml, IQR 475–4200 pg/ml; p = 0.006). There were no marked differences among the remaining groups.
Correlation of serum BAFF and APRIL levels with laboratory variables
Next, we determined the correlation coefficients of BAFF and APRIL with laboratory variables in the ILD group (Table 2). Serum BAFF and APRIL were positively correlated with AST and aldolase (p < 0.05), but not with CK (p = 0.51 and p = 0.88, respectively). Serum BAFF and APRIL were significantly associated with KL-6 (rs = 0.60, p = 0.003 and rs = 0.62, p = 0.0019, respectively) and IL-18 (rs = 0.46, p = 0.0026 and rs = 0.57, p = 0.0045, respectively). Ferritin had a positive correlation with APRIL (rs = 0.49, p = 0.026), but not with BAFF (p = 0.23).
Correlations of serum BAFF and APRIL levels with clinical and laboratory variables in ILD patients with JDM.
Correlation of serum BAFF and APRIL levels with anti-MDA5
Among MSA, anti-aminoacyl-tRNA synthetases (anti-ARS; anti-Jo1) and anti-MDA5 have been associated with ILD in patients with dermatomyositis27. We previously reported that serum anti-MDA5 was frequently observed in patients with ILD and that extremely high serum levels of anti-MDA5 (> 200 U) were found in all patients with RP-ILD as compared with C-ILD patients, whose anti-MDA5 was comparably lower (< 100 U)5. Here, all RP-ILD subjects had high titers of anti-MDA5, while 10 of 15 C-ILD subjects had lower values (Table 1). To evaluate the relative influence of BAFF and APRIL on anti-MDA5, the C-ILD group was subdivided into patients with and without anti-MDA5. The RP-ILD group having high anti-MDA5 exhibited significantly increased levels of BAFF and APRIL than did the C-ILD group with low anti-MDA5 (p = 0.019 and p = 0.0029, respectively; Supplementary Figure, available at jrheum.org).
Associations of BAFF and APRIL with clinical course in JDM patients with ILD
To determine the effect of immunosuppressive therapy on serum levels of BAFF and APRIL in JDM patients with ILD, we analyzed these cytokines in 8 JDM-associated ILD patients before and after treatment. Three patients with RP-ILD did not respond to therapy and succumbed to respiratory distress. Additionally, nonresponders exhibited pulmonary involvement as detected by HRCT (data not shown) and persistently high levels of serum KL-6 (nonresponders: mean 2375 U/ml, range 1767–6190 U/ml vs responders: mean 208 U/ml, range 242–750 U/ml), suggesting that disease activity was present after completion of treatment. In contrast, ILD symptoms and chest CT findings of the other 2 patients with RP-ILD and the 3 with C-ILD were both improved.
BAFF levels were significantly decreased after treatment compared with those at the diagnosis of ILD (p = 0.0078; Figure 2). Interestingly, the posttreatment BAFF levels in the patients who subsequently died remained higher than those of healthy controls. APRIL levels were reduced by treatment in 6 of 7 patients (Figure 2). However, 1 patient who succumbed to RP-ILD had markedly high values of APRIL in comparison with healthy controls, and the APRIL levels of the remaining 2 dead and 1 recovered patient with RP-ILD did not return to the levels of healthy controls.

{kind=link}
{kind=link}
Serum BAFF (left panel) and APRIL (right panel) levels in dead patients with JDM and rapidly progressive-ILD (RP-ILD; open triangles), recovered patients with RP-ILD (closed circles), and patients with C-ILD (open circles) at the diagnosis of ILD (pretreatment) and after completion of the treatment protocol shown in Table 2. Eight data points are shown for BAFF and 7 are displayed for APRIL. One C-ILD patient could not be examined for APRIL because of insufficient serum volume. The therapies used until the second sampling point are described in the supplementary table and are summarized as follows: all 5 patients with RP-ILD and 2 of 3 patients with C-ILD received methylprednisolone pulse therapy (25–30 mg/kg/day for 3 days) followed by high-dose corticosteroids (1–2 mg/kg/day) and cyclosporine. One patient with C-ILD was treated with corticosteroids and tacrolimus. Cyclophosphamide (500 mg/m2/day for 2–4 weeks) was added to the regimens of 3 patients with RP-ILD. Intravenous immunoglobulins were administered to 1 patient who died, 1 RP-ILD patient who recovered, and 1 patient with C-ILD. Significant difference is indicated by an asterisk. BAFF: B cell activating factor; APRIL: a proliferation-inducing ligand; JDM: juvenile dermatomyositis; C-ILD: chronic interstitial lung disease.
DISCUSSION
In our present study, we saw that serum values of BAFF and APRIL were significantly higher in the RP-ILD group than in the C-ILD group, which suggested that these cytokines may be markers of the rapidly progressive form of ILD in JDM. BAFF and APRIL were also positively correlated with KL-6 and IL-18 in the JDM patients with ILD. KL-6 is produced by type II alveolar epithelial cells and is known as a useful circulating biomarker for the clinical diagnosis of ILD and evaluation of disease severity28,29,30,31. Meanwhile, high levels of IL-18 have been observed in RP-ILD patients with adult-onset DM and JDM5,32. Gono, et al also suspected that macrophage activation in the lung tissue based on high levels of IL-18 could be a prognostic marker of RP-ILD32. In addition, we found that patients with high anti-MDA5 had higher BAFF and APRIL titers than those with lower values of anti-MDA5. In a previous study, we reported that a high titer of anti-MDA5 (> 200 U) was a possible disease marker of RP-ILD in patients with JDM5. The current results therefore support that BAFF and APRIL titers are correlated to ILD disease severity in JDM.
Krystufkova, et al described a relationship between BAFF and anti-Jo1 in IIM and implicated BAFF with anti-Jo1 production in IIM positive for anti-Jo16. There is increasing evidence supporting a critical association between unique MSA profiles and distinct clinical phenotypes not only in adult-onset DM, but also in JDM27,33. We observed positive results for anti-MDA5 in 78% of patients with ILD and only a low frequency of anti-Jo1, suggesting that anti-MDA5 was the MSA related most to Japanese ILD patients having JDM. Additionally, several roles of BAFF and APRIL in the production of autoantibodies have been reported6,15,16,17,18,34,35. The elevated levels of BAFF and APRIL in the RP-ILD group possessing high anti-MDA5 further indicated a role of B cells and these cytokines in the production of autoantibodies and disease phenotypes in this subset of JDM.
Our study revealed that the RP-ILD group alone had significantly high serum levels of APRIL, while both RP-ILD and non-ILD groups exhibited elevated BAFF. In previous reports, serum APRIL and APRIL mRNA in peripheral blood mononuclear cells were not raised in IIM6,21, but those studies did not include patients with RP-ILD. On the other hand, increased level of APRIL has been described in patients with other autoimmune diseases accompanying ILD36,37. We speculate that APRIL is more important in the pathogenesis of RP-ILD than in that of C-ILD. APRIL may be more directly involved than BAFF in the disease mechanisms of RP-ILD and more useful as a detection marker for JDM with RP-ILD.
BAFF levels were also significantly higher in the non-ILD group than in healthy controls. Gunawardena, et al reported that anti-transcriptional intermediary factor 1-γ protein, antinuclear matrix protein, and anti-Mi2 were the most common MSA in JDM (23–29%, 13–23%, and 2–13%, respectively) and described a low frequency of ILD among patients with those antibodies27. Accordingly, we cannot exclude the possibility that the high titers of BAFF in the non-ILD group may have been associated with other clinical phenotypes dependent on separate MSA.
Krystufkova, et al reported an association between BAFF and CK in IIM and speculated that BAFF levels are in close relation to local muscle involvement6. However, we found no relationship between circulating BAFF and CK levels in ILD accompanying JDM. Most of our patients with ILD had positive titers of anti-MDA5. Similarly to adult-onset DM, anti-MDA5–positive JDM appears to be a milder myositis phenotype and has normal levels of CK38. Our data also revealed that CK in the ILD group was within normal levels and lower in comparison with the non-ILD group. One possible explanation for this discrepancy is a difference in the analyzed subsets of clinical phenotypes. Another possibility is that CK is a low sensitivity indicator of muscle damage in JDM39. We observed an association of BAFF/APRIL with aldolase and AST in the ILD group. Aldolase and AST leak into the systemic circulation from damaged muscle and have been reported to more closely monitor disease activity than CK39. Several core sets have been proposed to assess myositis disease activity40, which will be important in the future evaluation of associations between BAFF/APRIL and myositis. We were unable to compare BAFF/APRIL levels with activity scores in the present study owing to a lack of standardized measurements of disease activity among the collaborating institutes.
The serum levels of BAFF and APRIL in most of our JDM patients with ILD were markedly decreased by immunosuppressive therapy, suggesting that BAFF/APRIL production was sensitive to this form of treatment. Further, posttreatment levels of the 2 cytokines in treatment responders returned to almost normal levels. In contrast, nonresponders persistently had increased BAFF/APRIL values, even after more intensive therapy, in comparison with responders. In spite of the limited cohort size, our results indicate that sustained abnormal levels of BAFF and APRIL may contribute to a poor response to treatment and that analysis of these cytokine levels after treatment may be useful for evaluating treatment progress in patients with ILD-JDM.
Our findings on BAFF and APRIL levels in ILD-JDM support the notion that these cytokines may be disease markers of RP-ILD that can be used to assess treatment response in ILD associated with JDM. The efficacy of B cell depletion therapy using rituximab has been reported in patients with refractory anti-ARS–positive DM complicated with chronic ILD as well as on the mucocutaneous lesions of patients with anti-MDA5-positive DM41,42,43,44. Anti-BAFF antibodies have shown favorable results in SLE patients with joint and skin disease8,19,20. Our data also indicate that BAFF and APRIL might constitute potential therapeutic targets for RP-ILD accompanying JDM.
Acknowledgment
We thank all patients and pediatricians for their contributions to serum samples and data analysis. We also thank Miyako Nakagawa and Etsuko Iwata for their excellent technical assistance.
Footnotes
Supported by a Health Labor Sciences Research Grant from The Ministry of Health, Labor, and Welfare of Japan.
- Accepted for publication July 23, 2015.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
ONLINE SUPPLEMENT
Supplementary data for this article are available online at jrheum.org.