
Abstract
Objective. Retinol-binding protein 4 (RBP4), an adipokine related to impaired glucose tolerance, has been associated with insulin resistance (IR) and β-cell function in subjects with obesity or diabetes. In our study we assessed RBP4 levels in patients with rheumatoid arthritis (RA). We also determined whether any correlation exists between RBP4 levels and the presence of IR in these patients.
Methods. Plasma RBP4, insulin, C-peptide concentrations, and homeostasis model assessment (HOMA)-IR were measured in 101 patients with RA and 115 sex-matched and age-matched controls. A multivariable analysis adjusted for IR classic cardiovascular risk factors and body mass index was performed to establish the correlation between RBP4 plasma concentrations and features of IR in RA. Data were adjusted for glucocorticoid intake in patients with RA.
Results. Patients had higher levels of insulin, C-peptide levels, HOMA-percentage of β-cell secretion (%B) index, and HOMA-IR index than controls. RBP4 levels were significantly lower in the whole group of patients than in controls [13.99 (9.78–19.88) vs 21.50 (10.28–32.59) μg/ml, p < 0.01]. However, only those who were glucocorticoid-naive showed significant difference in RBP4 plasma concentration when compared to controls [11.88 (7.93–17.96) vs 21.50 (10.28–32.59) μg/ml, p < 0.01]. The HOMA-%B [log β coefficient 0.00 (0.00–0.01), p < 0.01] showed positive relationships regarding RBP4 in controls. That was not the case in patients with RA [log β coefficient 0.00 (−0.0–0.00), p = 0.93 for HOMA-%B].
Conclusion. RBP4 does not correlate with the presence of IR and β-cell function in patients with RA. The mechanisms leading to IR in RA may be different from those occurring in obesity or diabetes.
- RHEUMATOID ARTHRITIS
- HUMAN RETINOL-BINDING PROTEIN 4
- INSULIN-SECRETING CELLS
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory disorder of unknown etiology that can lead to the destruction and deformity of joints because of the erosion of cartilage and bone. Epidemiologic data suggest that patients with RA have increased prevalence of premature atherosclerosis even after adjusting for traditional cardiovascular (CV) risk factors1,2,3. This accelerated atherosclerosis and increased risk of CV disease in patients with RA may be influenced, at least in part, by the presence of insulin resistance (IR).
Inflammation and disease severity play important roles in the development of IR in RA. In this regard, association of markers of inflammation, such as C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and disease activity scores with IR has been observed in patients with RA4. Similarly, β-cell function has been found to inversely correlate with Disease Activity Score (DAS28) and with swollen and painful joints. Chung, et al5 studied IR in 104 patients with RA and 124 patients with systemic lupus erythematosus (SLE). Patients with RA had a higher IR index than did those with SLE. In RA, IR showed a positive correlation with the levels of proinflammatory cytokines, interleukin 6 (IL-6), and tumor necrosis factor (TNF)-α, CRP, ESR, and carotid atherosclerosis6. Other studies have also shown a high incidence of IR in RA. They emphasized the link between IR and inflammation in RA5,7,8,9. However, other mechanisms may also account for the development of IR in RA10.
Retinol-binding protein 4 (RBP4) is a plasma protein released from adipocytes that has been found to correlate with the degree of IR in patients with obesity, impaired glucose tolerance, or type 2 diabetes, as well as in nonobese subjects with11 or without12 a strong family history of type 2 diabetes. Reduction of RBP4 levels has also been observed in individuals who experience improvement of IR with exercise. Studies in humans disclosed an inverse relationship between glucose transporter 4 (GLUT4) in adipocytes and serum RBP411. In addition, mice lacking adipocyte GLUT4 have increased RBP4 levels, leading to IR in muscle and liver13. Therefore, it is possible that increased serum RBP4 levels may contribute to impaired insulin-stimulated glucose uptake in the muscle and elevated hepatic glucose production, both of which are typical features of obesity and type 2 diabetes. However, the molecular mechanisms leading to IR mediated by RBP4 induction are unknown. Interestingly, RBP4 has been shown to induce the release of proinflammatory cytokines, including IL-6 by endothelial cells, in part through activation of NADPH oxidase and nuclear factor-κB transcription factor14. Therefore, RBP4 may inhibit insulin signaling in adipocytes by inducing proinflammatory cytokines in macrophages15.
Because the presence of a chronic inflammatory state is of high importance in the process of accelerated atherogenesis observed in RA2, it is plausible to think that inflammation may also play a key role in the mechanisms leading to IR in RA. This may be of singular importance to differentiate the development of IR in RA from that occurring in other conditions not associated with high chronic inflammation. In our study we aimed to assess whether serum levels of RBP4, a protein strongly associated with obesity and diabetes, correlate with the magnitude of IR observed in patients with RA.
MATERIALS AND METHODS
Study participants
Two hundred sixteen subjects, 101 patients with RA, and 115 age-matched and sex-matched controls were recruited for a cross-sectional study. All patients with RA were 18 years old or older, and fulfilled the 2010 American College of Rheumatology/European League Against Rheumatism diagnostic criteria16. All of them were diagnosed by rheumatologists and were periodically followed at rheumatology outpatient clinics. For the purpose of inclusion in our study, RA disease duration was required to be ≥ 1 year. To minimize the potential effects of TNF-α blockers on IR17, patients with RA undergoing TNF-α antagonist therapy were not included in our study. However, because glucocorticoids are often used in the management of RA, patients taking prednisone or an equivalent dose (12.5 mg/day or less) were not excluded. Nevertheless, to determine the potential effect of glucocorticoid therapy, we established 2 groups within the cohort of patients with RA; those receiving prednisone therapy (including subjects taking prednisone therapy at the time of the assessment or who had been taking glucocorticoids within 3 months prior to onset of the study), and another group of glucocorticoid-naive patients with RA. In patients included within the group of glucocorticoid-treated individuals, the glucocorticoid dose was measured as the equivalent prednisone dose administered during the previous 3 months (mg per day). Patients and controls with diabetes mellitus were not included in the study; therefore, none of the patients or controls were receiving glucose-lowering drugs or insulin therapy. In addition, patients and controls were required to have a glucemia < 7 mmol/l. Patients and controls were excluded if they had a history of myocardial infarction, angina, stroke, a glomerular filtration rate < 60 ml/min/1.73 m2, a history of cancer, any other chronic disease, or evidence of infection. None of the controls were receiving glucocorticoid treatment. Our study protocol was approved by the Institutional Review Committee at Hospital Universitario de Canarias (Spain), and all subjects provided written informed consent.
Data collection
Patient surveys for both the RA and control groups were identical, except for additional questions asked of patients with RA. Subjects completed a CV risk factor and medication use questionnaire and underwent physical examination to determine their anthropometrics and blood pressure. Medical records were reviewed to ascertain the specific diagnosis and medication. Waist circumference and hip circumference were measured and the waist-to-hip ratio was also estimated. In patients with RA, disease activity was measured using the DAS2818, whereas disease disability was determined by using the Health Assessment Questionnaire (HAQ)19. A subject’s metabolic syndrome was defined based on the 2005 National Cholesterol Education Program (Adult Treatment Panel III) criteria20.
Assessments
Serum RBP4 was measured using an ELISA (ALPCO Diagnostics). ELISA samples were run in duplicate; the coefficient of variation for interassay replicate samples was < 7%. The homeostatic model assessment (HOMA) method was performed to determine IR; specifically, in this study, we used HOMA2: the updated-computer HOMA model21. In brief, this method consists of a structural computer model of the glucose-insulin feedback system in a homeostatic (overnight-fasted) state. It comprises a number of nonlinear empirical equations (and precludes an exact algebraic solution), which describes the functions of organs and tissues involved in glucose regulation. This model can be used to determine insulin sensitivity (%S) and percentage of β-cell secretion (%B) from paired fasting plasma glucose and specific insulin levels, or from C-peptide concentrations across a range of 1 to 2200 pmol/l for insulin and 1 to 25 mmol/l for glucose. In our study, we used C-peptide to calculate β-cell function, because the former is a marker of secretion. In addition, we used insulin data to calculate %S (since HOMA-%S is derived from glucose disposal as a function of insulin concentration). This computer model provides an insulin-sensitivity value expressed as HOMA2-%S (where 100% is normal). HOMA2-IR (IR index) is simply the reciprocal of %S. Insulin (Architect Abbott, 2000I) and C-peptide (Immulite 2000; Siemens), coefficient of variation < 6% in both, were determined using chemiluminescent immunometric assays. Standard techniques were used to measure plasma glucose, CRP, the Westergren ESR, and serum lipids.
Statistical analysis
The number of patients recruited for this research was based on the results of a preliminary study in which we assessed RBP4 in 15 patients with RA and 15 controls. RBP4 in the control group was 21.0 (18.0–24.3) μg/ml, while in patients with RA it was 17.4 (14.3–23.5) μg/ml. Based on this information, using a 1:1 relation, and using Student t test with an α level of 0.05 and a β level of 0.10, we estimated that we would have to enroll 170 subjects: 85 patients and 85 controls. A comparison of the demographic and clinical characteristics of patients with RA and controls, using a Pearson chi-square test for categorical variables or a Student t test for continuous variables (data described as mean ± SD) is shown in Table 1. For noncontinuous variables, either a Mann-Whitney U test or a logarithmic transformation was carried out, and data were expressed as a median [interquartile range (IQR)]. Non-normally distributed variables were log-transformed when used in linear regression analysis. Multivariate analysis, adjusting for factors known to be associated with IR [sex, waist circumference, body mass index (BMI), and prednisone use], was performed to respectively assess the association of anthropometric measures with IR and IR with RBP4 in both controls and patients. All analyses used a 5% 2-sided significance level and were conducted using SPSS software, version 22 (IBM). A p value < 0.05 was considered statistically significant.
Demographic data, metabolic risk factors, and disease-related characteristics of patients and controls.
RESULTS
Clinical characteristics of patients and controls, and the relationship with IR and β-cell function
Table 1 summarizes the population data of our study. Age (55 ± 10 vs 56 ± 11 yrs, p = 0.49) and sex (85% and 90% of women, p = 0.33) in patients and controls, respectively, did not differ significantly. The frequency of hypertension, metabolic syndrome, waist and hip circumferences, waist-to-hip ratio split by sex, levels of total cholesterol, triglycerides, or low-density lipoprotein cholesterol did not differ significantly between patients and controls. Only high-density lipoprotein cholesterol levels showed significant differences (55 ± 13 mg/dl in controls vs 59 ± 15 mg/dl in patients, p = 0.04). As expected, ESR and CRP values showed statistically significant differences between patients and controls. Patients taking glucocorticoids did not differ from those not taking glucocorticoids in demographic data, BMI, waist and hip circumferences, and waist-to-hip ratio. That was also the case for waist and hip circumferences and waist-to-hip ratio differences when patients taking glucocorticoids or those not were stratified according to sex. Apart from a higher frequency of rheumatoid factor positivity in the subgroup of patients with RA taking glucocorticoids (78% vs 38%, p = 0.01), laboratory data (lipids and acute-phase reactants) did not differ between glucocorticoid-naive patients and patients taking glucocorticoids.
Table 2 summarizes the correlations between the demographic and laboratory data and between RA-related features and IR indexes in both controls and patients. In both controls and patients there were significant correlations between BMI, waist circumference, hypertension, and metabolic syndrome with HOMA-IR. Although waist circumference was correlated with HOMA-%B in controls, this was not the case for patients. Additionally, BMI and waist circumference were not associated with HOMA-%B in patients, and waist-hip ratio was inversely related to the HOMA-IR and HOMA-%B only in patients with RA. Nevertheless, ESR and CRP in patients with RA and controls did not show any correlation with IR indexes. Similarly, DAS28 and HAQ scores, as well as positivity for rheumatoid factor or prednisone use, were not significantly associated with IR indexes in our series.
Metabolic risk factors, systemic inflammation, and disease characteristics associated with insulin resistance (IR) indexes and retinol-binding protein 4.
Differences between patients and controls regarding IR and β-cell function and RBP4 plasma concentration
Univariate analyses demonstrated significantly higher levels in RA patients than in controls of insulin [81.26 (47.23–111.12) vs 59.03 (40.28–78.48) pmol/l, p < 0.01], C-peptide [0.72 (0.63–0.89) vs 0.58 (0.54–0.68) nmol/l, p < 0.01], HOMA-%B [101% (67% to 133%) vs 81% (56% to 114%), p < 0.01], and HOMA-IR [1.66 (0.86–2.26) vs 1.09 (0.73–1.52), p < 0.01; Table 3]. When patients were split into those taking glucocorticoids and those not, the former maintained this trend (i.e., exhibited higher levels) compared to controls. However, in HOMA-IR between controls and glucocorticoid-naive patients, no statistically significant difference was found [1.09 (0.73–1.52) in controls vs 1.30 (0.84–1.82) in patients with RA, p = 0.21].
Insulin resistance (IR)-related measures in patients and controls (univariate model).
RBP4 levels were significantly lower in the whole group of patients with RA group than in controls [13.99 (9.78–19.88) vs 21.50 (10.28–32.59) μg/ml, p < 0.01]. Nevertheless, when patients were stratified according to glucocorticoid intake, only those not taking these drugs (glucocorticoid-naive patients) showed significant differences in RBP4 plasma concentration when compared with controls [11.88 (7.93–17.96) vs 21.50 (10.28–32.59) μg/ml, p < 0.01]. In the subgroup of patients with RA taking glucocorticoid therapy, RBP4 levels were also lower than in controls [17.34 (11.97–22.94) μg/ml vs 21.50 (10.28–32.59)] but the difference was not statistically significant (p = 0.35; Figure 1).
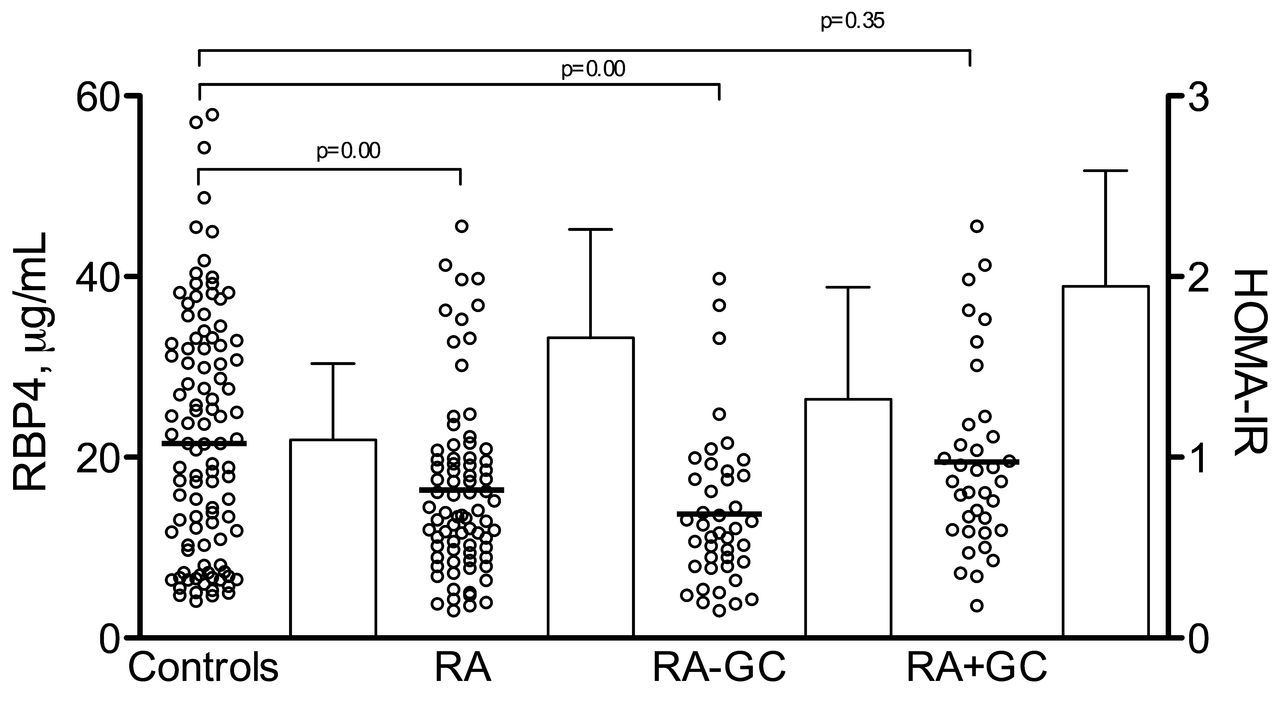
Retinol-binding protein 4 (RBP4; left axis) is expressed as dots (median) in controls, total number of patients with rheumatoid arthritis (RA), patients with RA not taking glucocorticoids (RA-GC), and patients with RA taking glucocorticoids (RA+GC). Homeostasis model assessment (HOMA)-insulin resistance (IR; right axis) is expressed as columns for the same groups (median ± interquartile range). RBP4 levels were significantly lower in the whole group of patients with RA than in controls (p < 0.01). However, when patients were stratified according to glucocorticoid intake, only those who were not taking these drugs showed significant difference in RBP4 plasma concentration when compared with controls.
Relationship of RBP4 with demographic data, RA features, and IR and β function
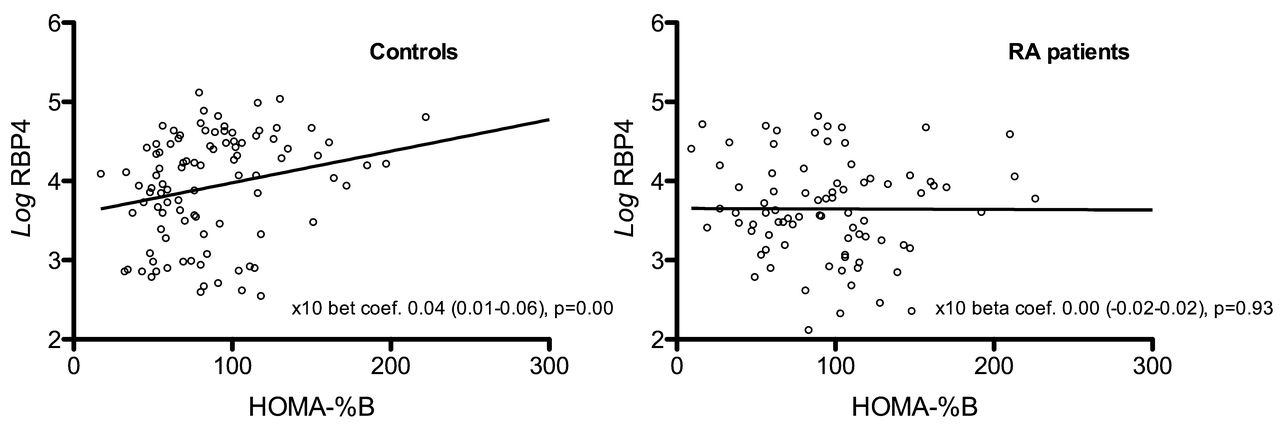
Table 4 depicts the relationship between RBP4 plasma concentration and IR in patients and controls. C-peptide levels, but not insulin concentrations, correlated with RBP4 plasma concentrations both in controls and patients with RA [log β coefficient 1.01 (0.10–1.91), p = 0.03 in controls and 0.88 (0.16–1.60), p = 0.02 in patients with RA, respectively]. ESR, CRP, and disease activity scores did not correlate with RPB4 levels. Only prednisone intake, when analyzed in a binary fashion, was associated with higher RBP4 levels [log β coefficient 0.39 (0.12–0.65), p = 0.01]. On the other hand, in controls, HOMA-%B [log β coefficient 0.00 (0.00–0.01), p = 0.00] showed a positive correlation with RBP4; this was not the case for patients with RA [log β coefficient 0.06 (−0.04–0.15), p = 0.24 for HOMA-IR and 0.00 (−0.0–0.00), p = 0.93 for HOMA-%B; Figure 2]. When this relationship was adjusted for sex, BMI, and waist circumference in controls; and then for sex, BMI, waist circumference, and prednisone intake in patients with RA, the relationship maintained the same trend. The interactions between prednisone intake and HOMA-IR and HOMA-%B, when a lineal regression was performed with RBP4, were all nonsignificant.
{kind=link}
{kind=link}
Retinol-binding protein 4 (RBP4) and homeostasis model assessment (HOMA)-%B univariate analysis for controls and patients with RA. Results were expressed as × 10 β coefficient (95% CI). RA: rheumatoid arthritis.
Metabolic risk factors, systemic inflammation, and disease characteristics association with RBP4.
DISCUSSION
RBP4, an adipokine, was reportedly associated with obesity and its comorbidities, especially IR, type 2 diabetes, and certain components of the metabolic syndrome22. Circulating RBP4 levels have also been positively correlated with intima media thickness, an established measure of atherosclerosis23 that predicts the risk of CV events in patients with RA24. To the best of our knowledge, RBP4 influence has not been explored in RA. Therefore our study constitutes the first attempt to determine the implication of this molecule in a disease where IR is closely linked to the presence of inflammation.
In our study we found that patients with RA, in particular those who are glucocorticoid-naive, have lower RBP4 levels than controls. Also, HOMA indexes correlate with RBP4 in controls but not in patients with RA, and RBP4 levels do not correlate with disease activity in patients with RA. Based on these findings, we hypothesize that IR, when present in patients with RA, is RBP4-independent and that low levels of RBP4 in these patients may be the result of a negative influence mediated by another factor associated with the disease (namely, the presence of a chronic inflammatory state).
Our data are in keeping with other reports that disclosed the presence of IR in patients with RA7,9,10,25,26. However, in contrast to other studies4,27, we did not find that the levels of ESR, CRP, or the disease activity scores assessed at the time of the study had a correlation with the presence of IR in our series. It is possible that the presence of lower levels of inflammation in our study, when compared with other studies, may explain these results. Therefore, low levels of inflammation, as shown in our study, may minimize the well-established effects that a proinflammatory state has on the development of IR in RA. In the study performed by Dessein, et al4, the median CRP level was 19.2 mg/l in a series of 81 patients with RA in whom high-grade inflammation showed a correlation with IR, while in our cohort of 101 patients the median CRP at the time of the study was only 3.8 mg/l. Therefore, as pointed out by the same authors, apart from inflammation, other mechanisms may be implicated in the increased risk of IR observed in patients with RA28.
As mentioned, serum RBP4 levels not only exist at higher levels in subjects with impaired glucose tolerance or type 2 diabetes, but also inversely correlate with insulin sensitivity in nondiabetic subjects11,12,29. In this regard, our finding that shows a correlation of RBP4 with IR indexes in controls is in agreement with these studies. Although we did not find a correlation between RPB4 and insulin levels, we were able to find a relationship with C-peptide levels in both patients and controls, effectively showing that this molecule is related to IR indexes. Interestingly, although C-peptide also correlated with RBP4 in patients with RA, HOMA indexes did not correlate, suggesting that HOMA indexes in RA may not be dependent on RBP4. In the same way, serum RBP4 levels have been found to be elevated and correlated positively with BMI in obese subjects with and without diabetes11,13. Consistent with this finding, we found a correlation, albeit only in patients with RA, between RBP4 and BMI and abdominal obesity. When we analyzed the relationship of RBP4 with disease features, we found no association with disease duration or activity scores. Further, we did not observe any correlation between CRP or ESR with RBP4 levels, although in another study, higher RBP4 levels were associated with markers of systemic inflammation30.
To our knowledge, the influence of glucocorticoids on RBP4 levels has not been studied in RA. In our study, patients with RA not exposed to glucocorticoids were the subgroup of patients with lower levels of RBP4. Patients with RA taking glucocorticoids and controls did not show statistically significant differences in RBP4 levels. The reason that glucocorticoids induce IR is not completely understood, but it seems to occur as a result of peripheral metabolic effects on skeletal muscle, liver, and adipose tissue, thus leading to hepatic gluconeogenesis, inhibition of glucose uptake in adipose tissue, and alterations in receptor and postreceptor functionality31. As RBP4 levels have been found to decrease with weight loss and exercise, it is reasonable to think that patients not exposed to glucocorticoids may have lower levels of RBP4 than those who were following such a regimen. Interestingly, in our series, patients who had not used glucocorticoids also exhibited lower levels of RBP4 than did controls. This means that these patients, in contrast to healthy controls, may have an inhibitory mechanism against this molecule stemming from the IR related to the disease itself. Our findings that showed that glucocorticoids induce higher levels of RBP4 could link them with a specific mechanism that is related to an alteration of the glucose metabolism.
To better understand the relationship between IR and RBP4 in patients with RA taking glucocorticoids, we constructed a multivariate analysis of the relationship of IR indexes, with RBP4 adjusted for glucocorticoid intake. We expected to find a significant relationship after the adjustment. However, this was not the case, because the relationship of IR indexes with RBP4, after adjusting for adiposity and glucocorticoids, was not significant. Therefore, an effect of interaction between glucocorticoids and IR indexes associated with RBP4 was not confirmed in our study. A plausible explanation for that may be related to the presence of a chronic inflammatory burden in our series of patients. In this regard, because inflammation plays a pivotal role in the mechanisms associated with IR and accelerated atherogenesis in RA, it is possible that our results indicate that the effect mediated by chronic inflammation prevails over those of glucocorticoids, adiposity, or RBP-4 levels in the development of IR in RA.
We found that IR in patients with RA was not associated with RBP4, a molecule that has been found to correlate with IR in other situations, such as obesity or diabetes. We believe that chronic inflammation or other unknown mechanisms implicated in the pathogenesis of RA may account for the development of IR in patients with RA. Although our study involved a relatively large number of subjects, the actual effect of RBP4 in the IR of patients with chronic inflammatory diseases warrants further investigation.
Footnotes
-
Supported by a grant to I.F-A. from the Fundación Española de Reumatología and by a grant to F.D-G. from the Spanish Ministry of Health (Fondo de Investigaciones Sanitarias; FIS 09/02209). The work performed by M.A.G-G. was supported by grants from “Fondo de Investigaciones Sanitarias” PI06/0024, PS09/00748, and PI12/00060 and by the RETICS Program, RD08/0075, and RD12/0009/0013 (RIER) from “Instituto de Salud Carlos III” (ISCIII), Spain.
- Accepted for publication November 19, 2013.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.