
The creation of the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for rheumatoid arthritis (RA; Figure 1)1 sought to address some of the criticisms of the previous ACR criteria set published in 1987 (Figure 2)2 — namely that they were insensitive, particularly early in the disease course, and that this led to the exclusion of many patients with early disease from clinical trials and research studies3. As a result, there was an absence of evidence regarding the efficacy of new treatments in this group of patients, who may have had the potential to benefit the most4,5. Thus, 1 aim of the 2010 criteria was to identify those patients with early RA with the key purpose of rapid disease-modifying antirheumatic drug (DMARD) initiation. However, the ability to classify patients as having RA is important at all phases of the disease, early and late. A case definition is required as an entry criterion not only to clinical trials, but also a consensus for inclusion in longterm observational studies and the whole spectrum of research in RA. Numerous studies have tested the validity of the new criteria since their publication against various standards6, but they have generally been applied in patients with relatively short duration of symptoms, ranging from < 3 months to < 2 years. Thus, the question remains, can we extend these classification criteria to patients with established disease?

2010 ACR/EULAR Classification criteria for RA1. ACR: American College of Rheumatology; EULAR: European League Against Rheumatism; RF: rheumatoid factor; ACPA: anticitrullinated protein antibodies; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; RA: rheumatoid arthritis. From Aletaha, et al. Ann Rheum Dis 2010;69:1580–8; with permission.
{kind=link}
{kind=link}
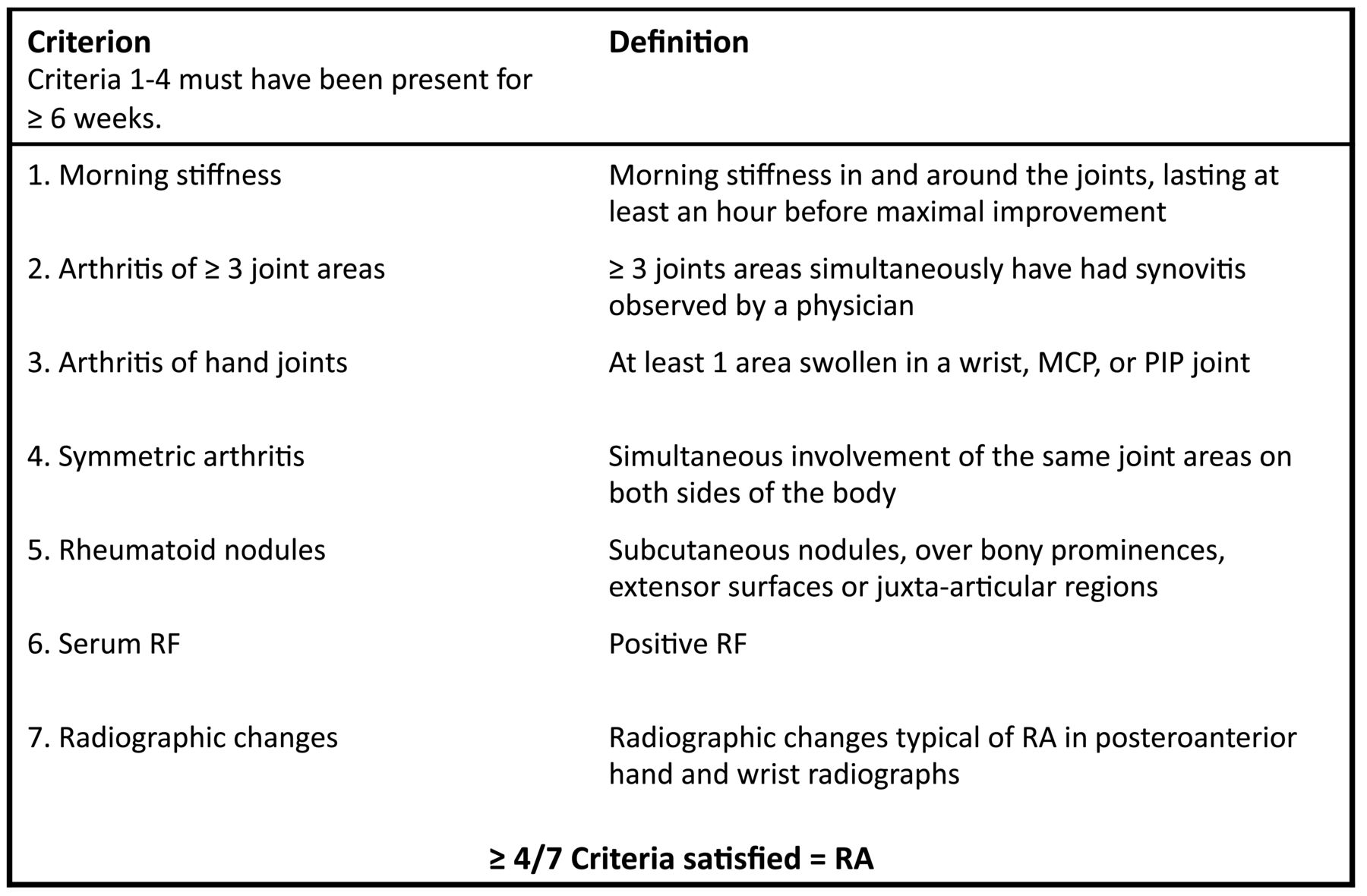
1987 ACR Classification criteria for RA2. ACR: American College of Rheumatology; RF: rheumatoid factor; MCP: metacarpophalangeal; PIP: proximal interphalangeal; RA: rheumatoid arthritis. From Arnett, et al. Arthritis Rheum 1988; 31:315–24; with permission.
Approach to Date
The committee who developed the 2010 criteria emphasized that they should encompass all patients who conform to the construct of “rheumatoid arthritis”1. To this end, they recommended 2 approaches for patients with late disease. First, they stated that the criteria could be applied retrospectively to those patients with the relevant available data1. There is inherent selection bias in this approach, which relies on adequate previous documentation unlikely to be available for all patients. In fact, there may be less documentation in those for whom the diagnosis was overt at initial presentation than in patients who required investigation over time to make a diagnosis. Second, they recommended that patients with radiographic evidence of erosions typical of RA should be considered as having prima facie evidence of RA, and automatically be classified that way1. Van der Heijde, et al established a definition of erosive disease as “evidence of at least 3 eroded joints on X-rays of hands and feet which are available at the time of classification”7,8. However, these studies used baseline radiographs in 2 cohorts of patients with early inflammatory arthritis (symptom duration < 2 yrs), the Leiden Early Arthritis Clinic and French ESPOIR cohort.
Challenges
The approaches so far give us no clues whether the 2010 criteria are useful and valid for patients with established disease. Indeed, there are considerable challenges to overcome if we wish to validate the 2010 criteria in these patients. For example, application of the erosion criteria could potentially classify some patients with psoriatic arthritis (PsA), gout, or erosive osteoarthritis as having RA, reducing the specificity of the criteria. These patients may fall under the exclusion criteria as having their synovitis better explained by another disease1. However, because 1 purpose of classification criteria is to provide a homogeneous group of patients for clinical trials, it has been suggested that any reduction in specificity seen with the 2010 criteria compared to the 1987 criteria is detrimental8.
An additional challenge is raised by the fact that the 2010 criteria are based on active joint involvement and raised inflammatory markers (Figure 1). There is, thus, potential for false negatives. Indeed, the 2010 criteria require a priori that a patient should have at least 1 joint with clinical synovitis at the time of applying the criteria, thus excluding any patient whose disease was in remission as a result of appropriate treatment. Given the current emphasis on aggressive management and aiming for remission, a proportion of patients with established disease may fail to satisfy the 2010 criteria if applied in a cross-sectional manner, or if the relevant information [e.g., anticyclic citrullinated peptide antibodies (anti-CCP) status] was not collected before they started treatment.
It may be necessary to adapt or change the 2010 criteria for use in established disease. This leads to the question of how to define “early” and “established” disease. Further, at what point does the transition from one to the other occur? Is transition only based on symptom duration, or also on clinical and radiographic features, or even a change in patient-reported outcomes?
Potential Solutions
How could we address these challenges? Some potential approaches are the modification of the 2010 criteria, the use of 1987 criteria in established RA, or the use of alternative criteria.
Modification of the 2010 Criteria
Could we adapt the 2010 criteria for use in established disease? Adaptations of the 1987 ACR criteria have previously been evaluated as well, for example, to include radiographs of the feet9, or allowing the replacement of active joint inflammation with deformed joints if radiographs were not available10.
Potential adaptations to the 2010 criteria might be the inclusion of some other typical RA features, for example, rheumatoid nodules, radiographic erosions, symmetrical joint involvement, classic deformities, or extraarticular manifestations. Intensive modern treatment strategies, however, decrease the prevalence of these “typical” RA features, which are frequently the consequence of long periods of uncontrolled disease activity that we aim to avoid in the modern era5,11.
It could be possible to further clarify “synovitis not better explained by another disease”, by constructing a list of differential diagnoses that need to be ruled out before the classification criteria can be applied. This list may be easier to develop than in early arthritis because disease-specific features, such as the characteristic structural damage of PsA, have had time to develop.
Another solution might be to apply different weighting to the 4 variables of the criteria in established disease. For example, reweighting might increase the value given to anticitrullinated protein antibodies (ACPA) positivity, because this is recognized to be more specific for RA than for rheumatoid factor (RF)12. Alternatively, a different cutoff could be used. Because the 2010 criteria were developed to identify patients with early disease requiring DMARD, a lower cutoff might be applied to patients already taking DMARD, in whom disease activity will be lower than those with newly diagnosed RA.
Importantly, any approach to modify the criteria would necessitate a data-driven validation, raising the question of how to best define an “RA” gold standard in such an analysis. Further, any modification may likely change the sensitivity and specificity.
Continued Use of the 1987 Criteria
An alternative to modifying the 2010 criteria would be to continue to use the 1987 criteria in these patients. The 1987 criteria have been shown to have better sensitivity and specificity in patients with longstanding disease compared to early disease13. However, there are a number of problems with this approach. First, it would be cumbersome to maintain 2 criteria sets. Second, it would introduce ambiguity to the research using both. Finally, it would essentially create 2 parallel disease definitions that may not, in fact, be describing exactly the same disease. However, a study from the Norfolk Arthritis Register demonstrated that there is reasonably good overlap between the 2 criteria sets if the 2010 criteria are applied soon after disease onset and the 1987 criteria are applied cumulatively over 5 years of followup14.
Alternative Criteria: Treatment
A further response could be to consider a rheumatologist diagnosis of RA alongside evidence of response to DMARD as equivalent to RA classification in established disease. This is a pragmatic solution, but could lead to significant heterogeneity as the majority of DMARD are also used to treat other inflammatory arthritides, and diagnosis is dependent on the opinion of the individual clinician. When physician diagnosis was used as the gold standard in validation studies of the 2010 criteria in early arthritis, results varied extremely widely between cohorts, with sensitivities ranging from 58–87%15,16. This viewpoint, however, is not meant to address diagnostic criteria, but to discuss the use of the 2010 classification criteria in established RA.
Alternative Criteria: Autoantibodies
Within the 2010 criteria, there is strong weighting given to the autoantibodies RF and ACPA. Synovitis of just 1 small joint for more than 6 weeks, with high levels of RF or ACPA, is sufficient to classify a patient as having RA. However, in studies that have made direct comparisons, most patients who satisfy the 1987 criteria but not the 2010 criteria are seronegative17,18,19. As stated above, ACPA is more specific than RF. Thus, in the context of established disease, it may be necessary to distinguish between RF-positive and ACPA-positive patients.
Could we therefore define all RA using autoantibodies? It could be postulated that patients with so-called “seronegative disease”, eventually differentiate into non-RA phenotypes. Other autoantibodies (such as antimutated citrullinated vimentin antibodies, an ACPA that is not detected by second-generation anti-CCP2, the most widely used test; and anticarbamylated protein antibodies) have been identified in anti-CCP–negative patients and associated with poor prognosis20,21. It is possible, therefore, that inclusion of other antibodies in the criteria could account for all those patients with poor outcomes. However, the supportive evidence around these antibodies as prognostic markers, other than RF and ACPA, is currently insufficient. Further, it would be important to confirm the stability over time of any such antibodies to use them to classify patients with established disease.
Conclusion
The 2010 ACR/EULAR classification criteria for RA represent a major step forward in rheumatology for patients in the early stages of RA and have already begun to inform the research agenda and our clinical practices8,22. Notably, they are different from the previous definition of the disease, characterized by damage. By allowing us to identify early those with poor prognostic markers requiring rapid intervention, this new definition perhaps better identifies the current construct of RA. However, it is important to remember that patients with longstanding disease numerically outnumber those with early disease, and we also require a robust method for their classification. We have summarized some of the many challenges in using the 2010 criteria in patients who are further into the natural history of the disease, and presented some of the potential options for dealing with them. Notably, all of the proposed solutions come with their own advantages and disadvantages. With our viewpoint article, we wish to stimulate the discussion of how to classify patients with established RA.
Acknowledgment
We thank Dr. Annette van der Helm-van Mil for her contribution.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.