
To the Editor:
Tumor necrosis factor-α (TNF-α) antagonists are effective treatments for inflammatory disorders but are associated with an increased risk of infections including reactivation of latent tuberculosis infection (LTBI). We describe a patient who developed miliary TB as a complication of TNF-α antagonist therapy despite negative pretherapy screening for LTBI.
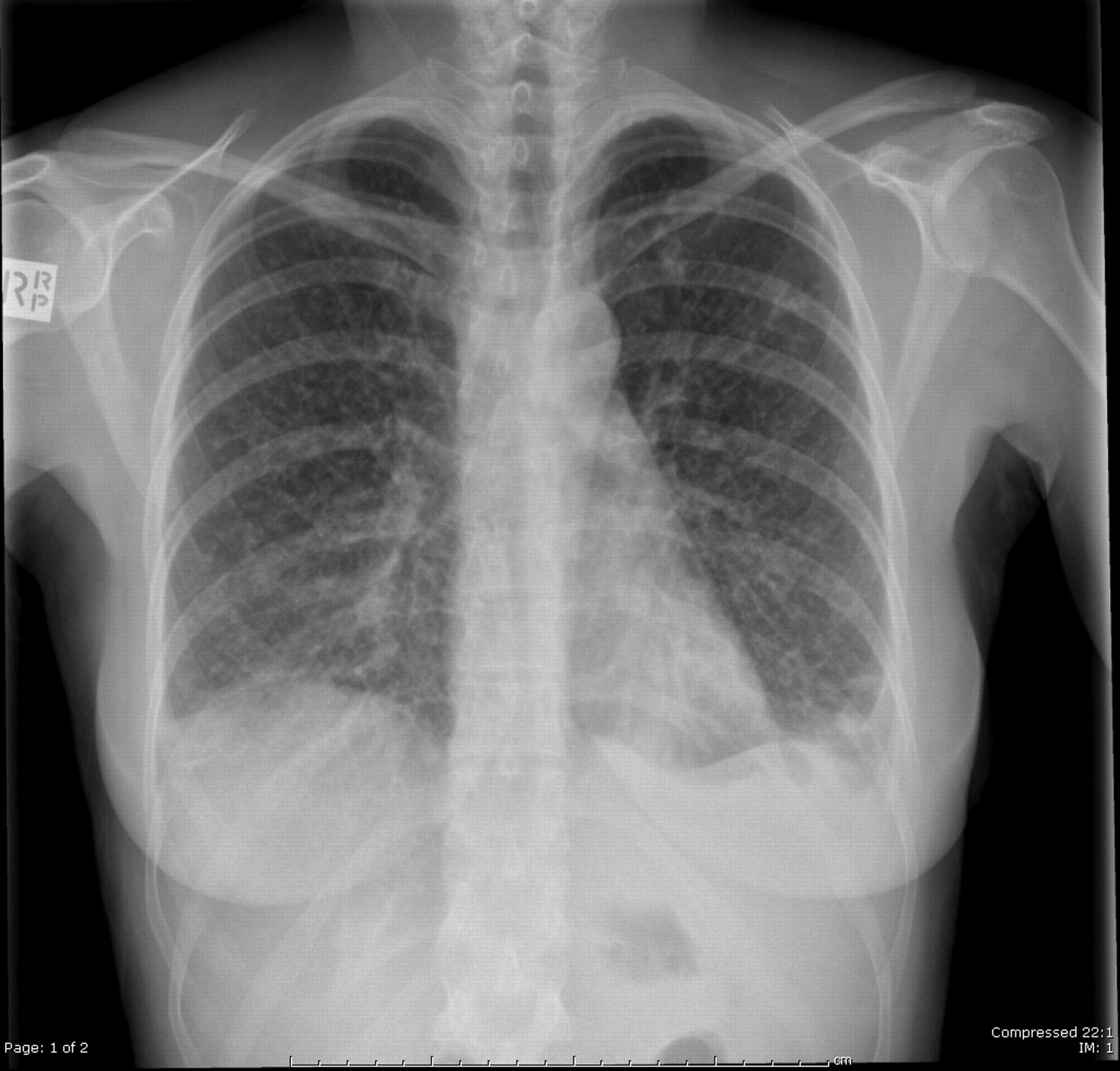
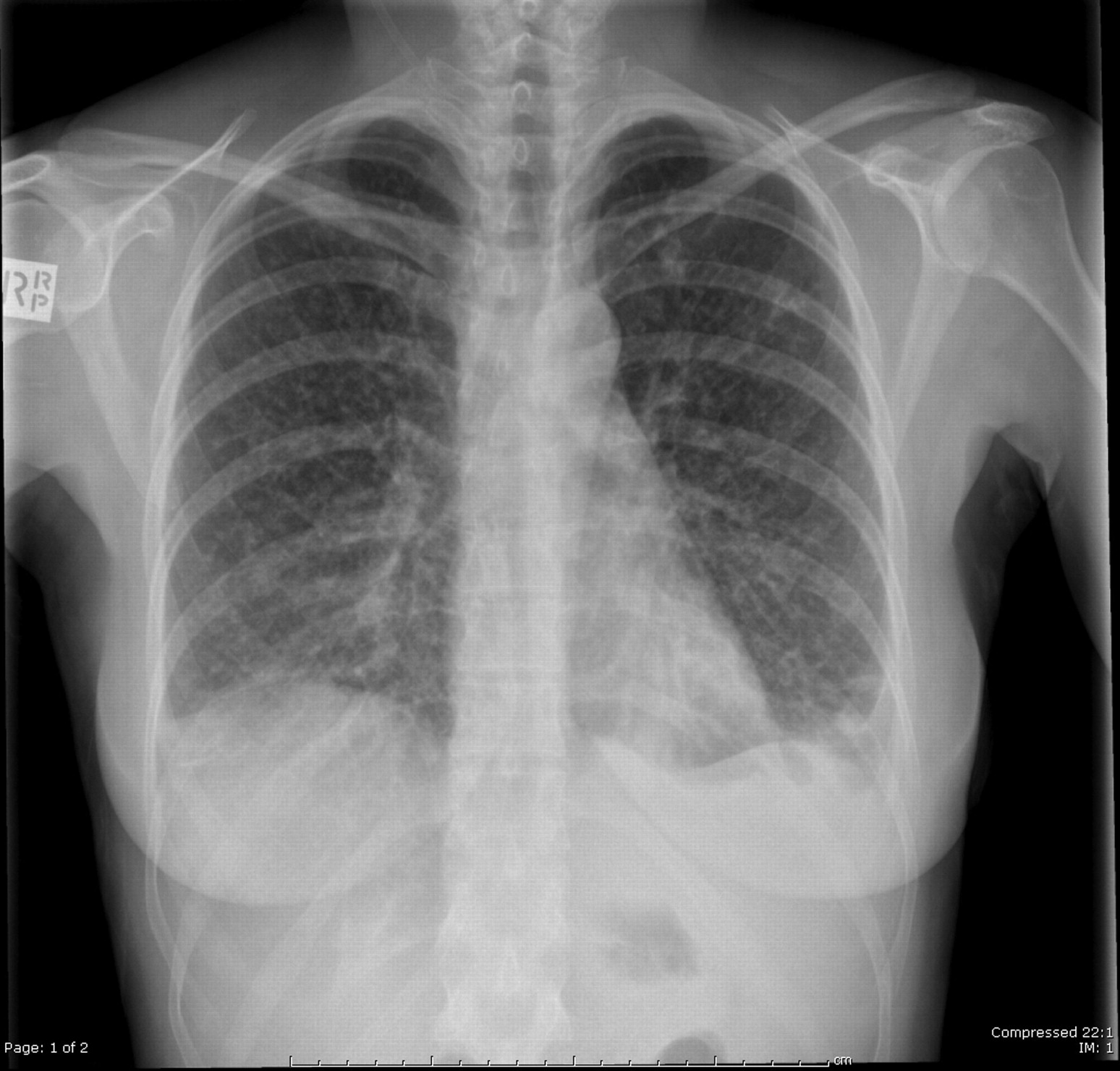
A 42-year-old woman with severe psoriatic arthritis presented with a 3-week history of fevers, night sweats, nonproductive cough, and 4-kg weight loss. She had been receiving treatment with adalimumab for 3 years after failing other disease-modifying antirheumatic drugs. A computerized tomography scan of her chest showed widespread nodules, bilateral lower zone patchy consolidation, and moderate splenomegaly, with small areas of nonenhancement consistent with miliary TB (Figure 1). She underwent bronchoscopy, which was smear- and culture-positive for Mycobacterium tuberculosis. She started isoniazid, rifampicin, pyrazinamide, and ethambutol, with resolution of symptoms over the following 2 weeks.
{kind=link}
Chest radiograph of the patient shows disseminated nodules throughout both lung fields.
This patient was born in Ireland and migrated to Australia when 3 months old. At age 12 years, her step-brother was diagnosed with pulmonary TB, her only known TB exposure. As part of family contact screening, she underwent tuberculin skin testing (TST), which was nonreactive, and subsequently received a Bacillus Calmette-Guerin vaccine. Prior to commencement of adalimumab, she was reinvestigated for latent TB infection with a chest radiograph, which was normal, and interferon-γ release assay (IGRA; QuantiFERON®-TB Gold In-Tube, Cellestis, Chadstone, Australia), which was negative. She had limited local travel, no international travel, and no other history to suggest new exposure to TB following the 2 screening tests. Although possible, this history makes new local acquisition of TB after screening unlikely. Following her symptomatic TB disease, a repeat IGRA was positive.
With increasing use of TNF-α antagonists, it has become apparent that this treatment is associated with an increased risk of serious infections. These are particularly due to intracellular pathogens, most notably a 5-fold increase in the risk of reactivation of M. tuberculosis infection1,2. TNF-α antagonists carry differential risks, with infliximab and adalimumab having higher rates of TB reactivation than etanercept3. As highlighted by our case, adalimumab is associated with the longest median time to reactivation, and TB is more likely to be disseminated with this than with the other TNF-α antagonists3.
Screening for and treatment of LTBI prior to initiation of TNF-α antagonists has been shown to be effective in markedly reducing the rates of TB reactivation4. The Australian Rheumatology Association has published guidelines on screening for LTBI prior to use of TNF-α antagonists, which recommend case history risk factor assessment, chest radiograph, and an IGRA or 2-step TST. In these guidelines, patients with “high” risk factors should be referred for consideration of LTBI treatment, which generally consists of 9 months of isoniazid therapy5. Other guidelines have instead suggested that only patients with prior personal history of TB, changes on chest radiograph, or positive IGRA should be referred for further assessment and treatment6.
As illustrated by our case, prior negative testing for LTBI does not eliminate the risk of TB following commencement of TNF-α antagonist therapy. The patient had a history of a nonhousehold TB contact but TB screening tests had been negative on 2 occasions; first, immediately following TB contact in childhood, and second, prior to TNF-α antagonist therapy. Accordingly, she was not given treatment for LTBI.
The case illustrates some of the difficulties in TB risk factor assessment and the pitfalls of relying on screening tests that carry a risk of false-negative results, especially in the setting of immunosuppression7. Alternative approaches, such as serial LTBI testing after initiation of TNF-α antagonists, have been proposed, as rates of conversion from negative to positive as high as 30% have been reported8. However, the clinical implications of such strategies are unclear.
This case highlights the need for careful specialist assessment of TB risks for all patients receiving TNF-α antagonist therapy. In addition to encouraging routine pre-TNF-α antagonist therapy screening, we would remind clinicians that high-risk patients, as defined by a personal history of TB (incompletely treated or not documented), unexplained abnormalities on chest radiograph in the appropriate epidemiological setting, or known contact with infectious pulmonary TB, should be considered for LTBI treatment regardless of the results of screening tests unless there is an unacceptably high risk of hepatotoxicity with isoniazid. A summary of practice points derived from this experience is given in Table 1. For patients born in high TB-incidence countries but without a defined history of TB exposure, we suggest that regular clinical monitoring for TB while on TNF-α antagonist therapy is appropriate, while alternative strategies such as serial IGRA or TST warrant further study. These cases illustrate that current screening strategies will not prevent all cases of TB reactivation and that clinicians need to maintain heightened vigilance for TB in patients receiving TNF-α antagonists, regardless of results of LTBI screening.
Summary of practice points from the case.
Acknowledgment
The authors thank Associate Professor Damon Eisen for his contribution and review of this report.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.