
Abstract
Objective. In patients with systemic sclerosis (SSc), to determine concentrations of antibodies against survivin and their clinical association with SSc, and to evaluate serum survivin concentrations.
Methods. Anti-survivin antibody was examined by ELISA and immunoblotting using human recombinant survivin. Serum survivin levels were assessed by ELISA.
Results. IgG but not IgM anti-survivin antibody levels in patients with SSc were significantly higher than those in healthy controls and patients with systemic lupus erythematosus (SLE). When cutoff values were set as mean + 2 SD of control, IgG anti-survivin antibodies were positive in 41% (25/61) of patients with SSc, while they were detected in only 1 healthy individual (3%, 1/29) and 1 patient with SLE (5%, 1/20). Regarding the clinical correlation, patients with SSc who were positive for IgG anti-survivin antibody exhibited significantly longer disease duration than those who were negative. Immunoblotting analysis confirmed the presence of anti-survivin antibody in sera from patients with SSc. Serum survivin levels in patients with SSc were also significantly higher than in controls and patients with SLE.
Conclusion. Our results suggest that autoantibody against survivin is generated in patients with SSc, especially those with long disease duration.
- SYSTEMIC SCLEROSIS
- AUTOANTIBODY
- SURVIVIN
Systemic sclerosis (SSc) is a multisystem disorder of connective tissue characterized by excessive fibrosis in the skin and various internal organs, such as lungs, kidneys, esophagus, and heart. Although the pathogenesis of SSc remains unknown, systemic autoimmunity is one of the central features, since antinuclear antibodies are detected in more than 90% of patients with SSc1. Patients with SSc have autoantibodies that react to various intracellular components, such as DNA topoisomerase I, centromere, RNA polymerases, U1RNP, U3RNP, Th/To, and histones1. Although it remains controversial whether these SSc-specific autoantibodies directly contribute to the clinical manifestations of SSc, autoantibodies against several intracellular and extracellular enzymes, including one of the antioxidant enzymes peroxiredoxin and matrix metalloproteinases, may play a pathogenetic role2,3,4.
Ischemic/reperfusion injury following Raynaud’s phenomenon, the most frequent first clinical manifestation in SSc, can generate reactive oxygen species that may result in vascular endothelial damage by inducing apoptosis5, suggesting that endothelial cell apoptosis is one of the preceding events in the development of SSc6. Apoptosis is a tightly regulated process of elimination of aged cells without disrupting cellular integrity7,8. Apoptosis may be initiated by extracellular stimuli through activation of death receptors on the cell surface, and intracellularly by the release of mitochondrial cytochrome c into the cytoplasm. Both pathways induce expression of apoptosis genes and activation of the caspase cascade, resulting in DNA fragmentation. The apoptosis signals are abrogated by the family of inhibitors of apoptosis proteins (IAP).
Survivin is a 142-amino acid-long protein described originally as a member of the IAP family containing a baculovirus repeat9. Survivin can downregulate, directly or indirectly, both death receptor-mediated and mitochondria-mediated pathways of apoptosis9. This direct, antiapoptotic effect of survivin is mediated by binding to caspases, especially caspase-3, or to a second mitochondrial activator of caspases10. However, reports give conflicting results on whether survivin can inactivate caspase-3 activity11,12. Survivin has also been suggested to regulate cell division during mitosis. Indeed, survivin is the only one of the IAP that is tightly connected to the cell cycle, being upregulated in the G2/M phase. Inside the dividing cell, survivin is found incorporated in centrosomes and mitotic spindles, and relocates to midbodies in the late telophase, and it is also present in nuclear centromeres13. Disruption of survivin function by negative mutation or by introduction of anti-sense oligonucleotides results in a cell division defect14,15. Survivin is abundantly expressed in all the most common human cancers and in transformed cell lines16, while most normal differentiated adult tissues do not express this molecule. However, several adult tissues, including spleen, testes, thymi, placentas, and the colonic crypts, express survivin.
A study has shown that plasma and synovial fluid survivin levels are increased in patients with rheumatoid arthritis (RA)16. High levels of survivin are associated with the erosive type of RA. Moreover, it was demonstrated that autoantibody response to survivin is related to a more benign (nonerosive) course of RA. We recently found that serum levels of autoantibodies against caspase-3 are elevated in patients with SSc17. In addition, this autoantibody inhibits caspase-3 enzymatic activity and is related to the severity of pulmonary fibrosis, vascular damage, and inflammation. Therefore, we hypothesized that survivin might contribute to the development of SSc by modulating apoptosis. To evaluate a role of survivin in the development of SSc, we investigated the presence of autoantibodies against survivin and their clinical correlation, and serum survivin concentrations in patients with SSc.
MATERIALS AND METHODS
Serum samples
Blood samples were obtained from 61 Japanese patients with SSc (53 women, 8 men); all fulfilled the criteria proposed by the American College of Rheumatology (ACR)18. These patients were grouped according to the classification system proposed by LeRoy, et al19: 37 patients (30 women, 7 men) had diffuse cutaneous SSc (dSSc) and 24 patients (23 women, 1 man) had limited cutaneous SSc (lSSc). The mean age of patients was 49 ± SD 16 years. Patients with dSSc were 48 ± 18 years old, and those with lSSc were 51 ± 13 years old. The disease duration of patients with dSSc and lSSc was 3.0 ± 2.9 and 9.7 ± 9.9 years, respectively. No patient with SSc was treated with oral corticosteroid, D-penicillamine, or other immunosuppressive therapy at the evaluation.
Antinuclear antibody was determined by indirect immunofluorescence analysis using HEp-2 cells as substrate. Specific ELISA kits were used for measuring serum anticentromere antibody (MBL, Nagano, Japan), anti-topoisomerase I antibody (MBL), and anti-U1RNP antibody (MBL), according to the manufacturer’s protocol. Anti-U3RNP and anti-Th/To antibodies were detected by RNA immunoprecipitation using 32P labeled HeLa cell extract. Anti-RNA polymerases I and III antibody was detected by protein immunoprecipitation using 35S-methionine labeled HeLa cell extract. Anticentromere antibody was positive in 21 patients, anti-topoisomerase I in 28, anti-U1RNP in 2, anti-U3RNP in 1, anti-RNA polymerases I and III in 6, and anti-Th/To in 1. The remaining 2 patients were negative for autoantibody.
Twenty patients with systemic lupus erythematosus (SLE) who fulfilled the ACR criteria20 were also examined as disease controls. No patient with SLE was treated with oral corticosteroid or other immunosuppressive therapy at the evaluation. Twenty-nine age- and sex-matched healthy Japanese individuals were used as controls. Patients with SSc, patients with SLE, and controls with a history of malignant tumors were excluded. Fresh venous blood samples were centrifuged shortly after clot formation. All samples were stored at −70°C prior to use.
Clinical assessment
Complete medical histories, physical examinations, and laboratory tests including vital capacity (VC) and diffusion capacity for carbon monoxide (DLCO) were conducted for all patients 3 to 5 weeks after serum collection. Skin score was measured by the modified Rodnan total skin thickness score (modified Rodnan TSS)21. Organ involvement was defined as described, with some modifications22, as follows: esophagus: hypomotility shown by barium radiography; joint: inflammatory polyarthralgias or arthritis; heart: pericarditis, congestive heart failure, or arrhythmias requiring treatment; kidney: malignant hypertension and rapidly progressive renal failure without any other explanation; muscle: proximal muscle weakness and elevated serum creatine kinase; pulmonary fibrosis: bibasilar fibrosis on chest radiography and high-resolution computed tomography; and isolated pulmonary hypertension: clinical evidence of pulmonary hypertension and increased systolic pulmonary arterial pressure (> 35 mm Hg) by Doppler echocardiography, in the absence of severe pulmonary interstitial fibrosis. When DLCO and VC were < 75% and < 80%, respectively, of predicted normal values, they were considered to be abnormal. The protocol was approved by our institutional review board and informed consent was obtained from all patients.
ELISA for anti-survivin antibody
We used purified full-length recombinant human survivin-His6 (R&D Systems, Minnepolis, MN, USA). ELISA was performed as described23. Briefly, 96-well plates were coated with recombinant human survivin (250 ng/ml) at 4°C overnight. The wells were blocked with 2% bovine serum albumin and 1% gelatin in Tris-buffered saline (TBS) for 1 h at 37°C. After 2 washes with TBS, serum samples (100 μl) diluted to 1:100 in TBS containing 1% bovine serum albumin were added to wells and incubated 90 min at 20°C. After 4 washes with TBS containing 0.05% Tween-20, the plates were incubated with alkaline phosphatase-conjugated goat anti-human IgG or IgM antibody (Cappel, Durham, NC, USA) for 1 h at 20°C. After 4 washes with TBS containing 0.05% Tween-20, substrate solution containing 0.91 μg/μl p-nitrophenyl phosphate (Sigma-Aldrich Co., St. Louis, MO, USA) in diethanolamine buffer (1 M diethanolamine, 0.5 M MgCl2) was added and the optical density (OD) of the wells at 405 nm was determined. We examined several concentrations (250 ng/ml, 500 ng/ml, 1 μg/ml, and 2 μg/ml) of survivin for coating the microtiter plates; as a result, similar results were obtained using several representative serum samples from patients with SSc and controls (data not shown). Therefore, we used the lowest concentration of survivin for this study. Further, we ran the assay in triplicate to minimize the inter-well variation: the mean of SD of triplicate OD values was 0.052. The average of the triplicate OD values was used for further analysis.
Immunoblotting
Immunoblotting was performed using full-length recombinant human survivin-His6 (16.5 kDa; R&D Systems) as described24. Recombinant human survivin (25 ng per lane) was subjected to electrophoresis and electrotransferred to nitrocellulose sheets. The nitrocellulose sheets were cut into strips and incubated overnight at 4°C with serum samples diluted 1:100. Then the strips were incubated for 1.5 h with alkaline phosphatase-conjugated goat anti-human IgG antibody. Color was developed using 5-bromo-4-chloro-3-indolyl phosphate and nitro blue tetrazolium (Sigma-Aldrich). Twelve patients with SSc who were positive for IgG anti-survivin antibody by ELISA and 12 healthy controls were evaluated.
ELISA for serum survivin levels
Specific ELISA kits were used for measuring serum survivin levels (R&D Systems), according to the manufacturer’s protocol25. Each sample was tested in duplicate.
Statistical analysis
Statistical analysis was performed using the Mann-Whitney U-test for determining the level of significance of differences between sample means, Fisher’s exact probability test for comparison of frequencies, and Bonferroni’s test for multiple comparisons. A p < 0.05 was considered statistically significant. All data were shown as means ± SD unless otherwise indicated.
RESULTS
Autoantibodies to survivin by ELISA
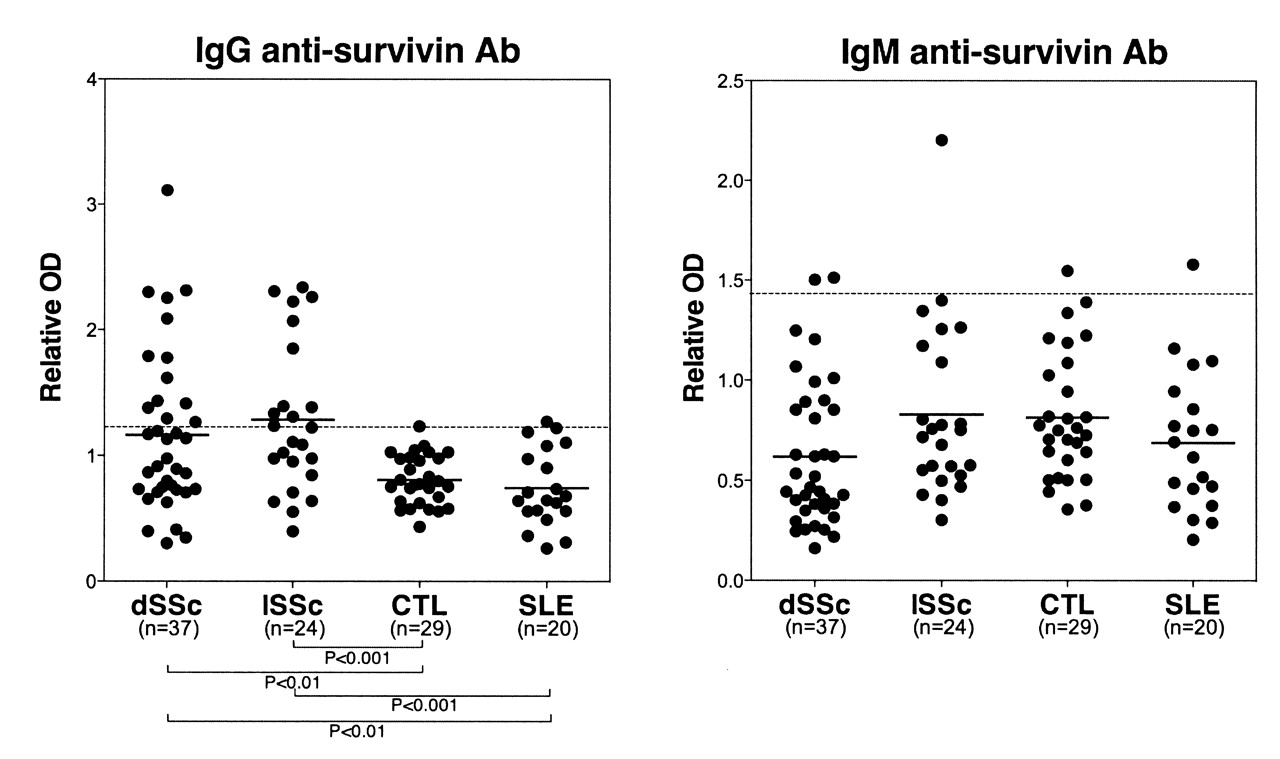
IgG anti-survivin antibody levels in total patients with SSc were significantly higher than those in healthy controls (p < 0.0001; Figure 1). Regarding the disease subsets, IgG anti-survivin antibody levels in patients with dSSc were significantly elevated compared with patients with SLE (p < 0.01) and controls (p < 0.01). Similarly, patients with lSSc exhibited significantly increased IgG anti-survivin antibody levels relative to patients with SLE (p < 0.001) and controls (p < 0.001). However, IgM anti-survivin antibody levels in patients with dSSc or lSSc were similar to those of controls and patients with SLE. OD values greater than the mean + 2 SD (1.202 for IgG anti-survivin antibody and 1.447 for IgM anti-survivin antibody) of controls were considered positive in this study (Figure 1). Among total patients with SSc, IgG anti-survivin antibody was detected in 41% (25/61). IgG anti-survivin antibody was detected in 35% (13/37) of patients with dSSc and positivity was also observed in patients with lSSc (50%, 12/24). In contrast, IgG anti-survivin antibody was detected in only 1 healthy individual (3%, 1/29) and 1 patient with SLE (5%, 1/20). IgM anti-survivin antibody was positive in 5% (2/37) of patients with dSSc, 4% (1/24) of patients with lSSc, 3% (1/29) of controls, and 5% (1/20) of patients with SLE. Thus, IgG but not IgM anti-survivin antibody levels were elevated in SSc.

IgG and IgM anti-survivin antibody (Ab) levels in serum samples from patients with dSSc, lSSc, healthy controls, and patients with SLE. Anti-survivin antibody levels were determined by ELISA using recombinant human survivin. Short bar indicates the mean value in each group; broken line indicates the mean + 2 SD of control.
Clinical correlation of anti-survivin antibody positivity
To investigate the clinical association of anti-survivin antibody positivity, physical and laboratory findings were compared between patients with SSc who were positive for IgG anti-survivin antibody and those who were negative (Table 1). Patients with SSc who were positive for IgG anti-survivin antibody had significantly longer disease duration (6.4 ± 8.2 yrs vs 4.9 ± 6.3 yrs in those who were negative; p < 0.05). IgG anti-survivin antibody-positive patients with SSc tended to have higher frequency of lSSc than negative patients; however, the difference did not reach statistical significance (48% vs 33%, respectively; p = 0.29). Prevalence of pulmonary hypertension tended to be lower in IgG anti-survivin antibody-positive patients relative to negative patients; however, the difference did not reach statistical significance (4% vs 18%; p = 0.12). On the other hand, there was no significant association of IgM anti-survivin antibody with clinical measures (data not shown). Thus, presence of IgG anti-survivin antibody was associated with longer disease duration in SSc.
Clinical and laboratory features of patients with SSc positive for IgG anti-survivin antibody. IgG anti-survivin antibody levels were determined by ELISA using human recombinant survivin. Optical density values greater than mean + 2 SD of healthy controls were considered positive.
Immunoblotting analysis
Presence of IgG anti-survivin antibody was further evaluated by immunoblotting using recombinant human survivin. Serum samples from patients with SSc positive for IgG anti-survivin antibody by ELISA exhibited reactivity with survivin (16.5 kDa) by immunoblotting (Figure 2, lanes 3–8). In contrast, no reactivity with survivin was observed using serum samples with anti-topoisomerase I, anticentromere, or anti-U1RNP antibody, but without IgG anti-survivin antibody by ELISA (lane 9 and data not shown). Further, control serum samples did not react with survivin (lane 10). Thus, the presence of anti-survivin antibody in patients with SSc was confirmed by immunoblotting analysis.

Representative immunoblotting of IgG anti-survivin antibody in serum samples from patients with SSc. Lane 1: markers for molecular weights (kDa). Lane 2: colloidal gold-stained survivin. Lanes 3–8: serum samples from patients with SSc who were positive for IgG anti-survivin antibody by ELISA. Lane 9: serum sample from a patient with SSc who was positive for anti-topoisomerase I antibody, but not for IgG anti-survivin antibody, by ELISA. Lane 10: healthy control sample.
Immunofluorescence analysis
We examined staining patterns by SSc sera positive for IgG anti-survivin antibody using HEp-2 cells as substrate in immunofluorescence analysis. A homogeneous pattern was observed in 56% (14/25) of patients with SSc positive for IgG anti-survivin antibody, a discrete speckled pattern in 36% (9/25), and a speckled pattern in 8% (2/25). Centrosomes, mitotic spindles, and midbodies were not stained by any serum samples positive for anti-survivin antibody.
Serum survivin levels by ELISA and clinical correlation
Serum survivin levels in patients with SSc, controls, and patients with SLE are shown in Figure 3. Serum survivin levels were significantly elevated in total patients with SSc (177 ± 75 pg/ml) compared with controls (138 ± 42 pg/ml; p < 0.001). For the subgroups of SSc, patients with dSSc (182 ± 86 pg/ml) exhibited higher survivin levels than those in controls (p < 0.01). Similarly, patients with lSSc (168 ± 53 mg/ml) exhibited significantly increased survivin levels relative to controls (p < 0.05). No significant difference in survivin levels between patients with dSSc and those with lSSc was observed. Serum survivin levels in patients with SLE (114 ± 29 pg/ml) were significantly decreased compared to controls (p < 0.05) and patients with dSSc (p < 0.0001) and patients with lSSc (p < 0.001). Serum survivin levels in patients with SSc showed no clinical correlation, including for disease duration (data not shown). IgG or IgM anti-survivin antibody levels did not correlate with serum survivin levels (Table 1 and data not shown). Thus, like anti-survivin antibody levels, serum survivin levels were increased in patients with SSc but not in patients with SLE.

{kind=link}
{kind=link}
{kind=link}
Survivin levels in serum samples from patients with dSSc, lSSc, healthy controls, and patients with SLE. Serum survivin levels were determined by a specific ELISA. Each histogram shows the mean + SD.
DISCUSSION
In this study, IgG anti-survivin antibody levels were detected in 41% of patients with SSc by ELISA, and the presence of anti-survivin antibody in patients with SSc was confirmed by immunoblotting analysis. The presence of IgG anti-survivin antibody was associated with longer disease duration. Serum survivin levels in patients with SSc were significantly higher than those in controls. These results suggest that serum levels of survivin, a member of the IAP family, are elevated in SSc and that autoimmune responses to survivin are generated in SSc with a long disease duration. However, there was no correlation between serum survivin levels and anti-survivin antibody levels or positivity. Our finding that patients with SSc who were positive for IgG anti-survivin antibody had significantly longer disease duration suggests that the period of existence of survivin in sera may be more important for B cell activation than serum survivin levels at one single timepoint. Further, the finding that anti-survivin antibody and serum survivin levels did not increase in patients with SLE, a multisystem disorder of connective tissue like SSc, suggests that the involvement of survivin in disease development and autoimmune responses to survivin differ between SSc and SLE.
Apoptosis is detected in endothelial cells at an early stage in SSc26. It has been shown that cleavage of certain autoantigens during apoptosis reveals immunocryptic epitopes that could induce an autoantibody immune response in systemic autoimmune diseases27. Many studies have shown that SSc is characterized by increased oxidative stress28. Indeed, ischemia and reperfusion injury following Raynaud’s phenomenon can generate reactive oxygen species that may result in vascular endothelial apoptosis29,30. Further, it is well known that Raynaud’s phenomenon is observed in patients with SSc from an early stage. Since survivin is one of the important components that can inhibit apoptosis, these results suggest that anti-survivin antibody may be produced during the process of apoptosis induced by oxidative stress. Our finding that the presence of anti-survivin antibody was associated with longer disease duration in SSc could support this hypothesis. To further evaluate the association between the development of anti-survivin antibody and Raynaud’s phenomenon as the early stage of endothelial vascular damage, we divided SSc patients with Raynaud’s phenomenon into 2 groups according to Rodnan TSS ≥ 13 points: (1) a group with mild skin sclerosis and (2) a group with severe skin sclerosis. Then we compared the positivity of IgG anti-survivin antibody between these 2 groups. As a result, the positivity of anti-survivin antibody was similar between the mild skin sclerosis group (46%; 11/24) and the severe skin sclerosis group (40%; 10/25). This result may be consistent with the notion that the development of anti-survivin antibody is related to endothelial damage in the early stage of the disease. Alternatively, one study16 has shown that autoantibody response to survivin is related to a more benign (nonerosive) course of RA, suggesting that anti-survivin may be a protective antibody. Our finding that IgG anti-survivin antibody positivity was higher in lSSc, a relatively milder disease subset, compared to dSSc suggests that anti-survivin may also be a protective antibody in SSc. The role of anti-survivin antibody in the development of SSc requires further studies.
In our study, centrosomes, mitotic spindles, and midbodies were not stained by any SSc serum samples positive for anti-survivin antibody. A previous study has shown that the monoclonal antibody 8E2, which reacted with centrosomes, mitotic spindles, and midbodies by immunofluorescence analysis, recognized only a conformational epitope within Cys57-Trp67; therefore, this antibody did not react with survivin by immunoblotting13. Another monoclonal antibody, 32.1, that recognized an epitope within Ala3–Ile19, reacted with nuclear centromeres but not centrosomes, mitotic spindles, and midbodies by immunofluorescence analysis and also reacted with survivin by immunoblotting analysis13. Thus, staining patterns by anti-survivin antibody may depend on epitopes recognized by each anti-survivin antibody. Our finding that autoantibody against survivin detected in SSc sera reacted with survivin by immunoblotting suggests that this autoantibody does not recognize the conformational epitope required for staining centrosomes, mitotic spindles, and midbodies, which could explain the lack of staining patterns of centrosomes, mitotic spindles, and midbodies by autoantibody to survivin. Rather, this autoantibody may exhibit a discrete speckled pattern that is usually generated by anticentromere antibody. A discrete speckled pattern was observed in only 36% of patients with SSc who had anticentromere antibodies in addition to anti-survivin antibody. It is possible that the homogeneous or speckled staining patterns detected in other patients with SSc who had anti-survivin antibodies masked the discrete speckled pattern of anti-survivin antibody.
Some recent studies have revealed the existence of anti-survivin antibody, mostly in patients with carcinoma. It has been reported that anti-survivin antibody was detected in 22% of sera from patients with lung cancer and in 8% of sera from patients with colorectal cancer by ELISA, and was not found in normal control sera31. Further, 2%–15% of patients with 11 different types of cancer possessed anti-survivin antibodies, while only 2% of healthy individuals had them. We showed that IgG anti-survivin antibody was positive in 41% of patients with SSc who had no history of malignant tumors. Another study detected anti-survivin antibody in 2% of patients with SLE and none of the patients with Sjögren’s syndrome who were investigated32. This frequency of positive anti-survivin antibody in patients with SLE was similar to that in our study (5%). When the cutoff was set at mean + 3 SD, the positivity of IgG anti-survivin antibody was 26% (16/61) of patients with SSc, which was still higher than the positivity reported in patients with SLE or Sjögren’s syndrome — 0% to 2%32. On the other hand, all healthy controls and patients with SLE are negative for IgG anti-survivin antibody at this cutoff value. The serum dilution for ELISA was different between our study (1:100) and the other studies (1:200)32. However, this could not explain the high prevalence of anti-survivin antibody in patients with SSc, since similar results were obtained using a serum dilution of 1:200 (data not shown). Therefore, these results suggest that patients with SSc have anti-survivin antibody more frequently than patients with various carcinomas, and that anti-survivin antibody is specific to SSc, compared to SLE or Sjögren’s syndrome.
Footnotes
-
Supported by a grant for Research on Intractable Diseases from the Ministry of Health, Labour and Welfare of Japan.
- Accepted for publication April 5, 2010.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.