
Abstract
Objective. Azathioprine is widely used in patients with autoimmune diseases and after organ allografting. A recognized carcinogen, azathioprine is also associated with the development of therapy-related myelodysplastic syndrome and acute myeloid leukemia (t-MDS/AML).
Methods. In 56 reported cases, azathioprine had been administered for a median of 65 months (range 6–192) to a median cumulative dose of 146 g (range 19–750) before t-MDS/AML developed.
Results. In 11 patients, repeated episodes of cytopenias developed during azathioprine therapy, ante-dating the development of t-MDS/AML. In 33 cases with successful karyotypic analysis, 26 cases (79%) showed monosomy 7, deletion of the long arm of chromosomes 7 and 5, and rearrangement of chromosome 11q23. These changes were cytogenetic hallmarks of MDS/AML secondary to known leukemogenic agents and radiotherapy.
Conclusion. The observations implicate azathioprine as a leukemogenic agent. It will be prudent to review the need for azathioprine therapy when unexpected cytopenias occur and prescription has been prolonged.
- AZATHIOPRINE
- MYELODYSPLASTIC SYNDROME
- ACUTE MYELOID LEUKEMIA
- CYTOGENETICS
Azathioprine is a thiopurine popularized in the 1960s as an immunosuppressive drug in renal allografting1. The efficacy of azathioprine as an immunosuppressant soon led to its application in rheumatologic diseases2. This was followed by an expansion of its indications to autoimmune blood diseases3, inflammatory bowel disorders4,5, and multiple sclerosis6. More than 4 decades since its initial use, azathioprine continues to be part of the treatment algorithms of these disorders.
Pharmacology and metabolism of azathioprine
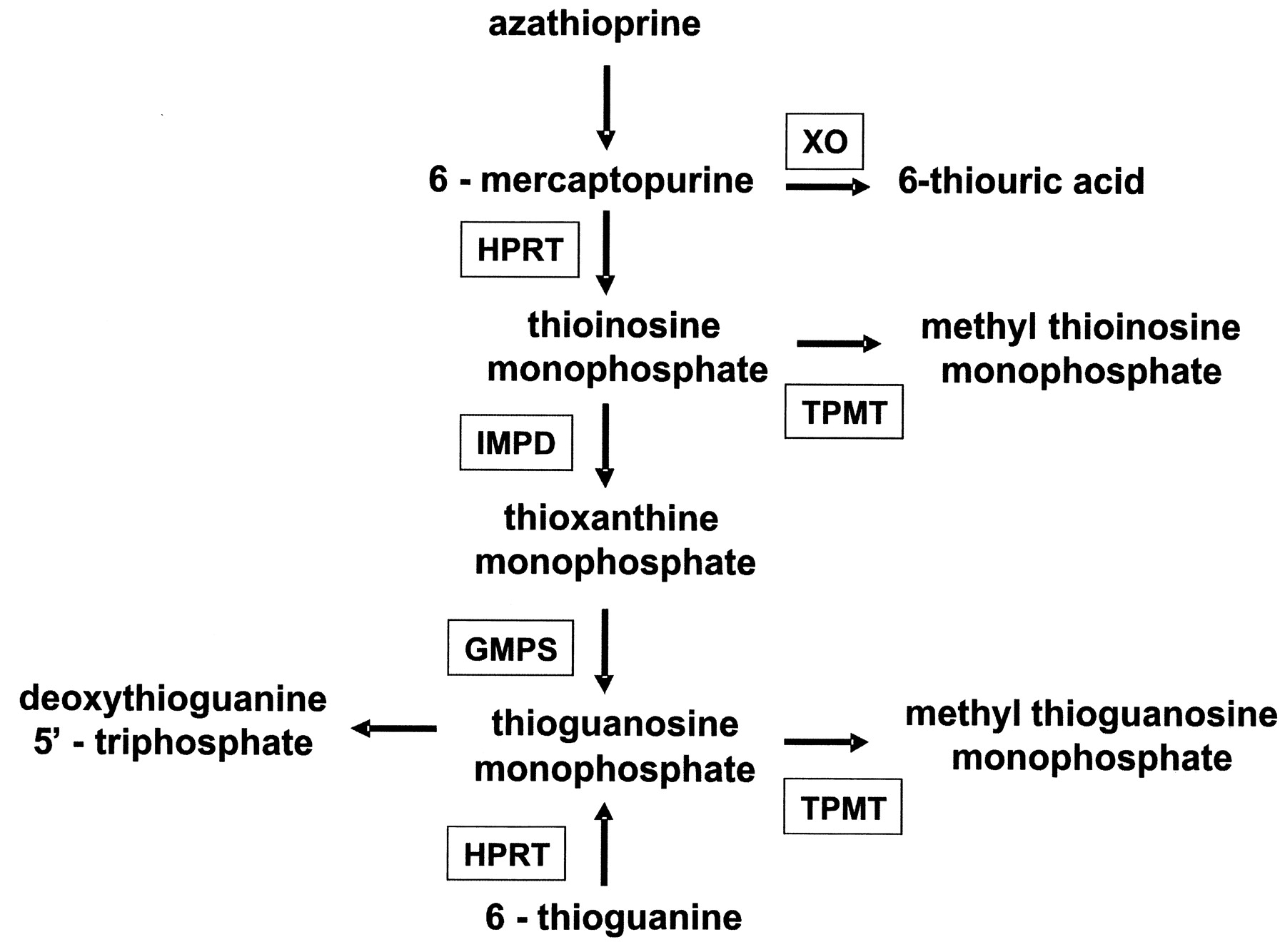
Azathioprine, 6-mercaptopurine (6-MP), and 6-thioguanine (6-TG) constitute the thiopurine group of antimetabolites (Figure 1)7. Azathioprine is converted by glutathione to 6-MP8. 6-MP is converted by hypoxanthine phosphoribosyltransferase to thioinosine monophosphate (TIMP). TIMP is subsequently converted to thioguanosine monophosphate, which is then converted by deoxynucleotide kinases and reductase to deoxythioguanine 5’ triphosphate, a substrate for DNA polymerase in DNA synthesis. Azathioprine is catabolized by 2 enzymes: xanthine oxidase, which converts 6-MP to 6-thiouric acid, and thiopurine methyltransferase (TPMT), which converts TIMP to methyl-TIMP.
{kind=link}
Metabolism of azathioprine and the other thiopurines. HPRT: hypoxanthine phosphoribosyltransferase; XO: xanthine oxidase; TPMT: thiopurine methyltransferase; IMPD: inosine monophosphate dehydrogenase; GMPS: guanine monophosphate synthetase.
The biologic effects of azathioprine may be affected by its catabolism. Allopurinol inhibits xanthine oxidase, and its administration increases the effective azathioprine dosage 4-fold. Polymorphic variants of the TPMT gene encode proteins with reduced activities. Heterozygotes for these variants require lower doses of azathioprine. Homozygotes may develop serious to fatal marrow toxicity after azathioprine administration7.
Toxicity of azathioprine
In addition to problems associated with immunosuppression, azathioprine has other adverse effects. Azathioprine-induced pancreatitis is well known9. The use of azathioprine in inflammatory bowel diseases may be associated with hepatotoxicity10,11.
The carcinogenic potential of azathioprine is not as well known. The International Agency for Research on Cancer classified azathioprine as a human carcinogen12. Malignancies attributed to azathioprine therapy are in general rare tumors13, and during oncogenesis other co-carcinogenic factors, such as graft-vs-host disease after allogeneic hematopoietic stem cell transplantation, may be involved14. However, recent data have shown an association between azathioprine treatment and therapy-related myelodysplastic syndrome and acute myeloid leukemia (t-MDS/AML), a complication unknown to most prescribing physicians.
The development of t-MDS/AML when azathioprine is used to treat nonmalignant diseases is catastrophic. Therefore, the association between azathioprine and t-MDS/AML must be critically appraised, in order to define risk factors that may predispose patients to this fatal complication.
MATERIALS AND METHODS
English publications indexed in Medline were searched using the key words azathioprine, secondary, therapy-related, myelodysplasia, myelodysplastic syndrome, and acute myeloid leukemia. Articles with complete patient demographics, diagnosis, and treatment outcome were reviewed. References in these publications were also scrutinized to ensure that all relevant articles were included.
RESULTS
Patients
A total of 56 patients were identified15–42. Their characteristics are described in Table 1. Details for each patient are given in the Appendix. The underlying indications for azathioprine treatment were autoimmune diseases in half of the cases, and solid-organ allografting in the other half. Men and women were equally affected.
Characteristics of 56 patients with therapy-related myelodysplastic syndrome/acute myeloid leukemia, after azathioprine treatment.
Azathioprine treatment
In organ allograft recipients, azathioprine was part of the triple therapy that included cyclosporine and prednisolone. For the remaining patients, azathioprine was the only relevant medication in 25% (10/41) of cases. Five patients had received other medications, including cyclophosphamide (n = 4), gold (n = 2), penicillamine (n = 1), and levamisole (n = 1). Of all the medications accompanying azathioprine therapy, only cyclophosphamide is known to be potentially leukemogenic. The median duration of azathioprine therapy was 65 months (range 6–192), at a median cumulative dose of 146 g (range 19–750).
Hematologic toxicity of azathioprine
Of 27 cases where information on hematologic toxicity during azathioprine therapy was available, 11 patients developed cytopenias before the development of t-MDS/AML (Table 2). The presentation included anemia, leukopenia, thrombocytopenia, or their combinations. The cytopenias necessitated a reduction of dose or temporary cessation of azathioprine. However, in all cases azathioprine was readministered after the cytopenias recovered. Although the cytopenias were attributed to marrow toxicity of azathioprine, in 1 case it was associated with the concomitant use of allopurinol33.
Clinicopathologic features of 56 cases of therapy-related myelodysplastic syndrome/acute myeloid leukemia, after azathioprine treatment.
t-MDS/AML
AML was the diagnosis in 55% of cases. For patients presenting with MDS, 18 (32%) had excessive leukemic blasts (refractory anemia with excess of blasts, refractory anemia with excess of blasts in transformation) or finally transformed into AML. Hence, 87% of patients presented with a leukemic disease. Only 13% of patients had MDS with a more chronic course (refractory anemia, refractory anemia with ringed sideroblasts, and refractory anemia with multilineage dysplasia).
Karyotypic aberrations
Cytogenetic analysis was performed in 33 cases. Aberrations of chromosome 7, either as monosomy 7 (absence of one of the homologues), or del(7q) (deletion of the long arm), were the predominant abnormalities, occurring in 22 cases (66%). Five other aberrations were found: del(5q) in 3 patients, del(20q) in 2, rearrangement of 11q23 in 1, inversion of chromosome 16 in 1, and complex (≥ 3 abnormalities) in 2. Two patients had normal cytogenetics.
Outcome
Treatment outcome was dismal, with 37 patients (66%) having died of disease at the time of reporting.
DISCUSSION
This review identified 56 cases of t-MDS/AML after azathioprine treatment. Although in 31 cases other medications had been used previously or concomitantly, most of the drugs, including cyclosporine, prednisolone, gold, penicillamine, and levamisole, were not known to be oncogenic. Cyclophosphamide was the only medication that might contribute to leukemogenesis, but it was used in just 4 cases. Therefore, azathioprine was the only medication that might be related to the leukemogenesis in the majority of cases.
The duration and cumulative dosages of azathioprine preceding t-MDS/AML were variable. For the cohort, a cumulative dose of 146 g (corresponding to a mean daily dosage of 75 mg) of azathioprine was prescribed and the median duration was 65 months before t-MDS/AML developed. Therefore, azathioprine apparently had to be given for a prolonged period before leukemogenesis occurred.
Although the association between azathioprine and t-MDS/AML appears strong, a causal relationship is more difficult to establish. An inherent risk of malignancies is increased in patients with autoimmune diseases43 and organ allografts44. Chronic inflammation is an important disease component in these disorders. Inflammatory mediators including chemokines, cytokines, and prostaglandins affect numerous tissue and cellular functions, which may contribute to oncogenesis by promoting the growth and survival of transformed cells, increasing angiogenesis, or interfering with effective immunosurveillance45. The concomitant use of immunosuppressive drugs also impairs humoral and cellular immune responses against neoplastic cells. Therefore, it is conceivable that these factors may play a co-carcinogenic role, collaborating with azathioprine in leukemogenesis. Another important observation indicating a leukemogenic role of azathioprine was the cytogenetic findings. In 22 patients, monosomy 7 and/or del(7q) was found. These abnormalities of chromosome 7 are highly characteristic of t-MDS/AML secondary to alkylator-based chemotherapy46,47. In 4 other cases, del(5q) and rearrangement of chromosome 11q23 were observed. These changes are also typical of t-MDS/AML secondary to leukemogenic agents such as topoisomerase inhibitors and radiotherapy46–48. Therefore, of 33 azathioprine-treated patients successfully karyotyped, 26 cases (79%) showed karyotypic aberrations typical of t-MDS/AML secondary to known leukemogenic agents. In vitro data have also suggested that azathioprine might select for mismatch repair deficient cells in the bone marrow. t-MDS/AML developing after azathioprine often showed mismatch repair deficiency, as reflected by microsatellite instability49, again supporting a leukemogenic role of azathioprine. These observations strongly implicate azathioprine as a causative agent in t-MDS/AML.
It is unclear whether the occurrence of t-MDS/AML after azathioprine is dose/duration related, or associated with individual susceptibility. Given that a large number of patients receive azathioprine for various indications, and only a relatively limited number of patients develop t-MDS/AML, risk factors in addition to dose/duration may also be involved. Interestingly, of 27 patients where hematologic toxicity was documented, 11 (40%) of them had cytopenias preceding t-MDS/AML, often by years. The reasons for these cytopenias were not given and might be related to excessive doses of azathioprine. However, problems with azathioprine metabolism might be contributory. In 1 case, concomitant allopurinol was prescribed inadvertently, leading to repeated episodes of pancytopenia before t-MDS/AML finally supervened33. Further, genetic variants encoding for low-activity TPMT may lead to undue marrow toxicity when azathioprine is prescribed. It has been estimated that 10% of the population may have a single deficient gene, and 0.3% may be homozygously deficient50. Hence, genetic variants of TPMT, by increasing the effective dose of azathioprine, may enhance the genotoxicity of azathioprine and thus predispose to t-MDS/AML. Therefore, whether antecedent cytopenias during azathioprine treatment reflect genetic problems of drug metabolism and may be harbingers of t-MDS/AML will need to be studied. Unfortunately, none of the reported cases of t-MDS/AML after azathioprine treatment were investigated for possible genetic variants of TPMT.
Because a small but significant number of patients treated with azathioprine developed t-MDS/AML, which bears the genetic hallmarks characteristic of leukemogenic agents, precautions are required during azathioprine treatment. Concomitant allopurinol must be avoided. Routine testing for TPMT variants does not appear warranted50. However, when unexpected cytopenias develop, and if facilities are available, testing for TPMT variants may provide useful guidance for future dose adjustments. Finally, until more mechanistic data are available on the risk factors or susceptibility to t-MDS/AML in patients treated with azathioprine, it will be prudent to review the need for azathioprine when it has been prescribed for more than 5 years, or for a cumulative dose exceeding 140 g.
APPENDIX

Footnotes
- Accepted for publication October 2, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.