
Abstract
Objective. To determine if hospitalizations for specific infectious exposures are associated with hospital admissions for Henoch-Schönlein purpura (HSP).
Methods. We conducted a retrospective cohort study using administrative data of children admitted to 40 children’s hospitals between January 1, 2002, and December 31, 2008. We examined the association of standardized rates of group A ß-hemolytic Streptococcus (GABS), Staphylococcus aureus, parainfluenza, influenza, adenovirus, and respiratory syncytial virus (RSV)-associated hospital admissions with standardized rates of HSP hospital admissions on a month by month basis using autoregressive moving average process models to account for temporal autocorrelation and clustering by hospital.
Results. Among the 3,132 admissions for HSP observed over the 7-year study period, hospital admissions were most frequent September through April, but with substantial variability between hospitals for each month. Accounting for these month by month differences within each hospital, the rate of HSP admissions in a given month increased significantly as the standardized rates of GABS (p = 0.01), S. aureus (p < 0.01), and parainfluenza (p = 0.03) admissions increased.
Conclusion. Our results demonstrate a local month by month temporal association between hospitalization for GABS, S. aureus, and parainfluenza and hospitalization for HSP. Future investigations will be required to determine causality.
- PEDIATRIC RHEUMATOLOGY
- EPIDEMIOLOGY
- VASCULITIS
- INFECTION
- HENOCH-SCHÖNLEIN PURPURA
Henoch-Schönlein purpura (HSP) is an acute vasculitis, affecting 8 to 20 per 100,000 children each year and accounting for half of all childhood vasculitis in the United States1,2. According to the European League Against Rheumatism (EULAR), HSP is defined as occurring when there is palpable purpura plus one of the following: diffuse abdominal pain, any biopsy showing predominant IgA deposition, arthritis or arthralgias, and renal involvement (any hematuria or proteinuria)3. HSP is characterized by prominent seasonal variation, with most cases occurring in the winter or spring. While the precise etiology of HSP is unknown, IgA, genetics, and infections each appear to contribute to the pathogenesis. Decreased glycosylation of IgA1 increases its propensity to aggregate, activates the alternative complement pathway, and results in tissue deposition4,5. Familial genetic aggregation studies6,7 and an established association with familial Mediterranean fever syndrome8 lend support for a genetic predisposition for HSP. Additionally, the seasonal nature suggests that antecedent infections contribute to disease pathogenesis in genetically susceptible children. HSP is preceded by an upper respiratory tract infection in 30%–50% of cases9,10,11, but there is no clear and consistent evidence for an etiologic role of any single organism.
Infectious triggers reportedly associated with HSP are numerous and include Group A ß-hemolytic Streptococcus (GABS), Staphylococcus aureus, Kingella kingae, Barton-ella henselae, Helicobacter pylori, Pertussis, Mycobac terium avium-intracellulare complex, Salmonella, Shigella, Campylobacter, Mycoplasma pneumoniae, influenza, Epstein-Barr virus, hepatitis A, hepatitis B, human immunodeficiency virus, parvovirus B-19, adenovirus, varicella, Coxsackie virus, and herpes simplex virus. The number of purported infectious associations raises the possibility that several microbial agents trigger the necessary immunologic response, in susceptible individuals, that results in HSP.
How can the various hypotheses regarding associations between these infectious agents and the onset of HSP be tested? A direct method, involving a large cohort (or case-control study) of children screened for these agents and monitored (or selected) for onset of HSP would be ideal. An indirect method, however, would be to observe at a population level whether the timing of outbreaks of specific infectious agents is tightly correlated with outbreaks of new-onset HSP. Similar studies have been done for evaluating the association of air pollution and asthma12. Data to perform such a study exist within the Pediatric Health Information System (PHIS) database, an administrative database that contains comprehensive inpatient data from more than 40 pediatric hospitals from all regions of the United States. Of note, the PHIS database does limit the sample to only those children who are sufficiently ill to require hospitalization, due to either a specific infectious agent or HSP, so the association would be among the most severe cases. Nonetheless, the analysis would provide evidence for an association that could then be tested by either other indirect or direct methods.
This study employs a retrospective cohort study design to preliminarily evaluate a local month by month temporal association of hospitalization due to several common upper respiratory pathogens and hospitalization for HSP. Specifically, we analyzed the PHIS database, which contains clinical data regarding all children admitted to 40 non-competing children’s hospitals located throughout the US; the large sample size and diverse geographic locations of the participating hospitals enable this design to estimate the association of hospitalization due to infections and hospitalizations due to HSP across hospitals.
MATERIALS AND METHODS
Human subjects protections
This study was reviewed by The Children’s Hospital of Philadelphia Committee for the Protection of Human Subjects and institutional review board and declared not human subjects research.
Study design
This retrospective cohort study utilized the PHIS administrative database to determine if specific infectious exposures are associated with hospital admission for HSP.
Data source and quality
The PHIS database is an administrative database that contains comprehensive inpatient data from pediatric hospitals from all regions of the US. Participating hospitals are affiliated with the Child Health Corporation of America (CHCA; Shawnee Mission, KS), a business alliance of children’s hospitals. The database contains administrative inpatient demographic, diagnostic, and procedural data from noncompeting freestanding tertiary care pediatric hospitals in the US. Data are de-identified and subjected to rigorous reliability and validity checks prior to inclusion in the database. Data that do not meet an established error threshold are rejected and must be corrected before resubmission13.
Forty-one hospitals contributed to the PHIS database between January 1, 2002, and December 31, 2008. After exclusions for data quality issues, 40 hospitals and 2,377 hospital-months of data remained for the final analysis.
Eligibility
Eligible subjects were children younger than 18 years of age at admission with discharge dates from a CHCA-participating hospital between January 1, 2002, and December 31, 2008 (N = 3,275,947). Inclusion criteria were an International Classification of Diseases-9-Clinical Modification (ICD-9-CM) code indicating a discharge diagnosis of HSP, GABS, S. aureus, parainfluenza, influenza, adenovirus, or respiratory syncytial virus (RSV) (See Appendix for list of ICD-9-CM codes included). Subjects with a discharge diagnosis of another rheumatic condition such as Wegener’s granulomatosis (WG), systemic lupus erythematosus, juvenile dermatomyositis, or polyarteritis nodosa, were excluded.
Outcomes
The primary outcome was an estimate of a temporal association between admission for HSP and GABS, S. aureus, parainfluenza, influenza, adenovirus, or RSV.
Independent variables
Prespecified fixed-effects covariates included standardized rates of admission for each infection, admission month, and admission year. Admitting hospital was included as a prespecified random-effects covariate. Hospital-specific admission rates were calculated based on counts of monthly admissions assigned a discharge diagnosis of HSP or any of the infections in a given 12-month period (August to July).
Statistical analysis
We used autoregressive moving average (ARMA) process modeling on the time series data to study the association between standardized rates of admission for HSP and each infection. The relation of the outcome at time yt to previous forecasting errors is called a moving average (MA) process. The dependence of the outcome at time yt on lagged values is called an autoregressive (AR) process. The ARMA model consists of 2 parts, an AR part for correlation of outcomes within a hospital, and an MA part for the variance caused by unobserved events. The ARMA (1,1) model fit the variance structure better than a first-order autoregressive model (AR (1)) and antedependence covariance structure (ANTE (1)). The residual plot demonstrated evenly distributed residuals around 0. The mixed-effect models were fitted using the PROC MIXED function with ARMA (1,1) covariance structure in SAS 9.2 for Windows (SAS Institute, Cary, NC, USA). Descriptive statistics were conducted using Stata 10.1 (StataCorp, College Station, TX, USA).
RESULTS
Hospital admissions
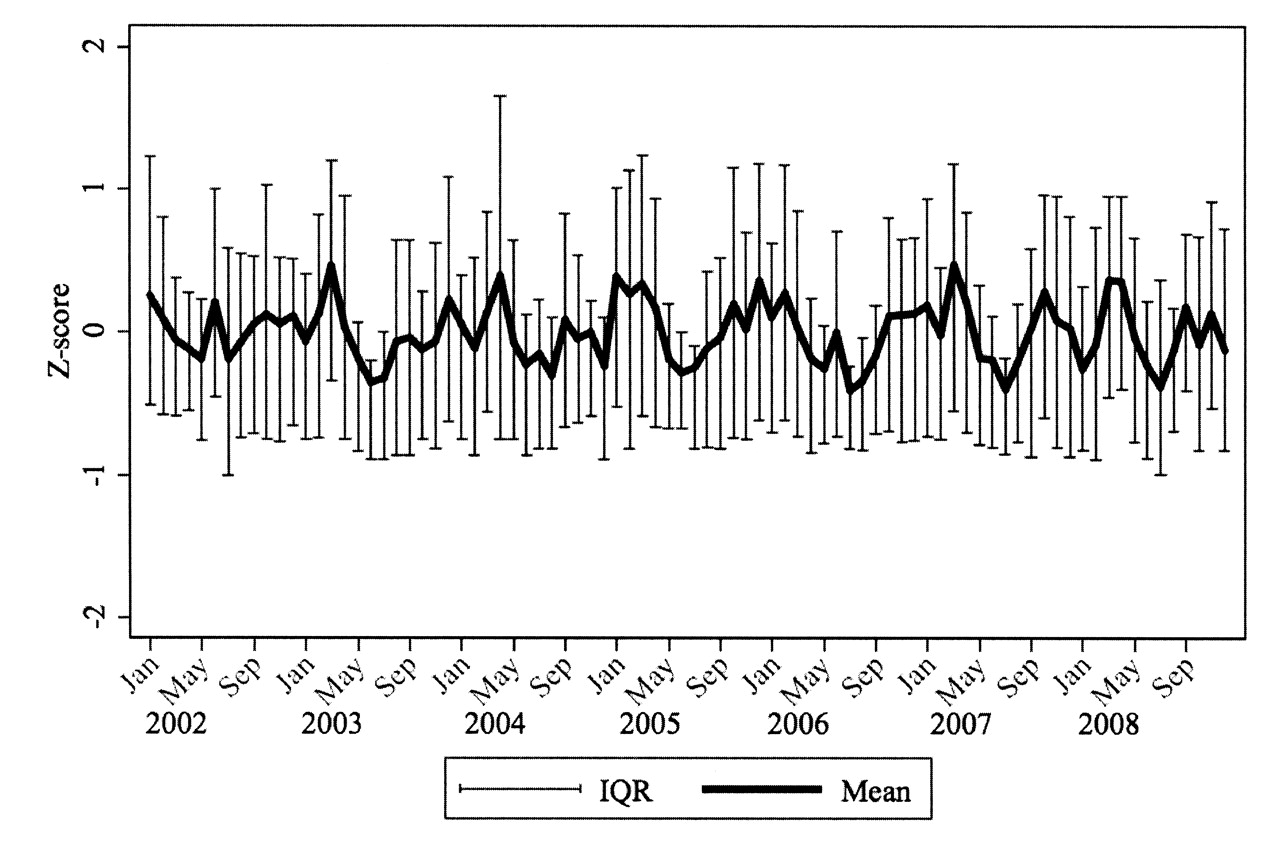
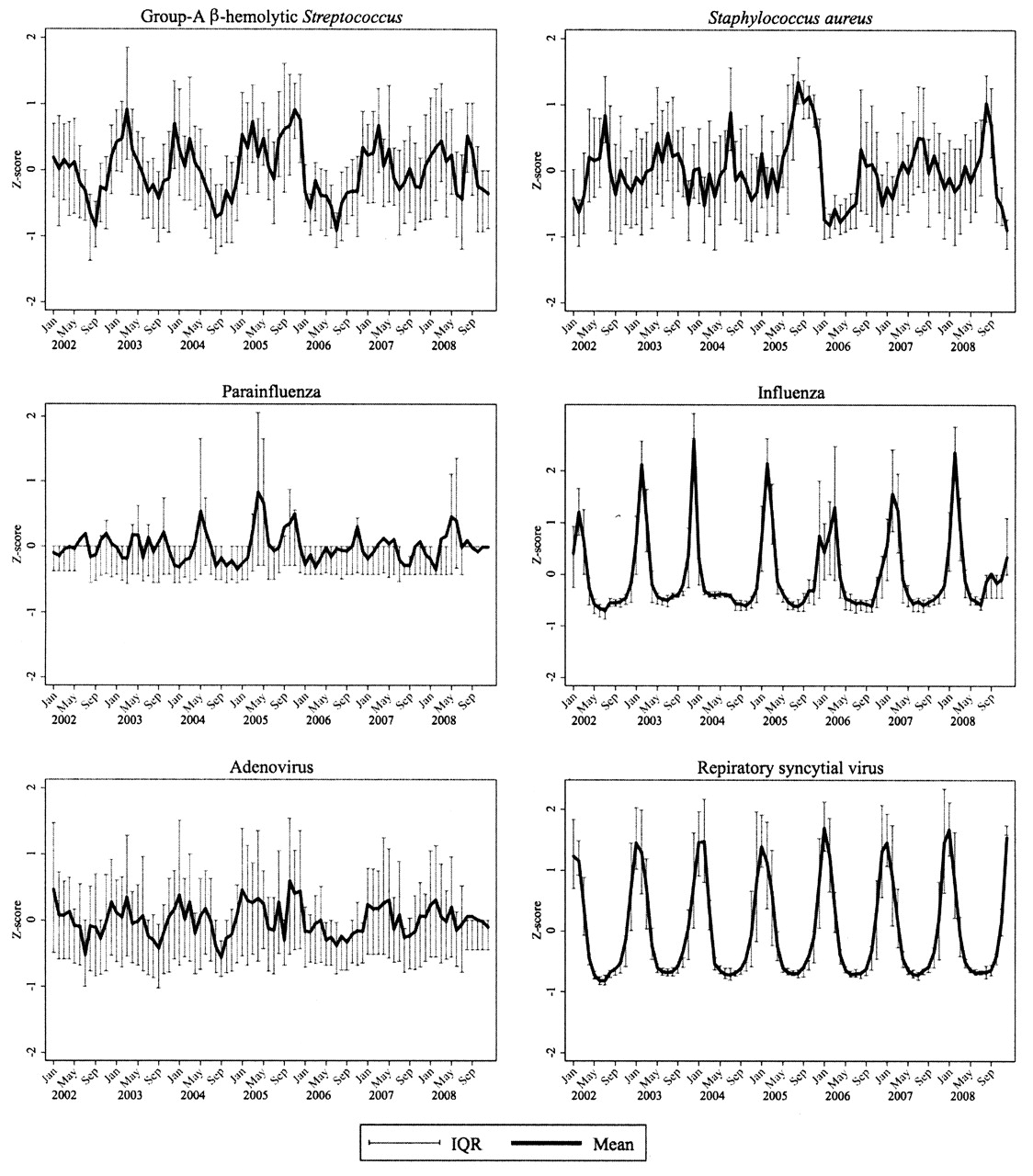
During the 7-year study period there were a total of 3,132 hospital admissions for HSP. Subject characteristics are presented in Table 1. Hospital admissions for HSP were most frequent September through April, but with substantial variability between hospitals for each month (Figure 1). This seasonal variation is consistent with observations in previous studies14,15,16,17. Similar to HSP hospitalizations, there was prominent seasonal variation in hospitalizations for each infection, with wide variability in rates between hospitals for each month (Figure 2).
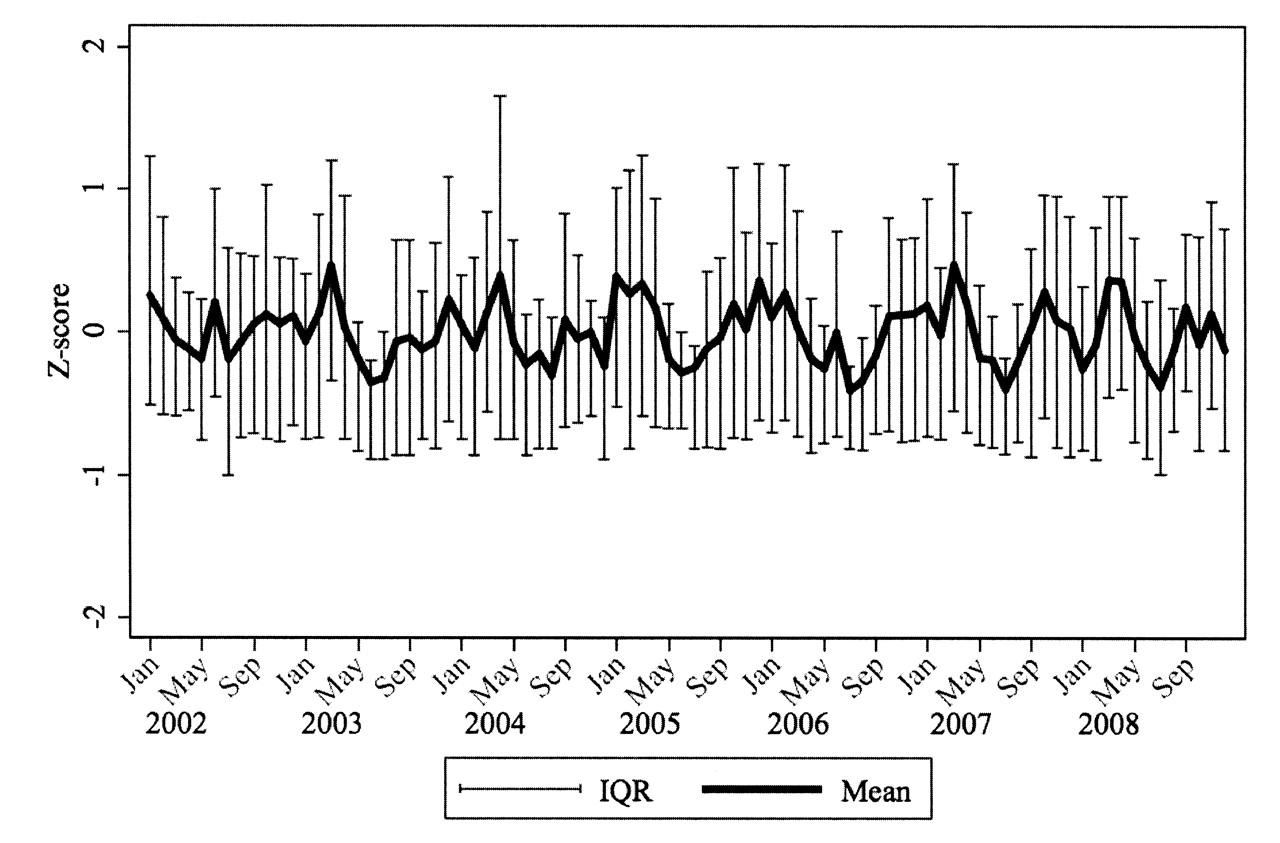
Hospitalizations for Henoch-Schönlein purpura (HSP). Data are Z scores and interquartile ranges (IQR) across hospitals for HSP admissions each month 2002–2008.
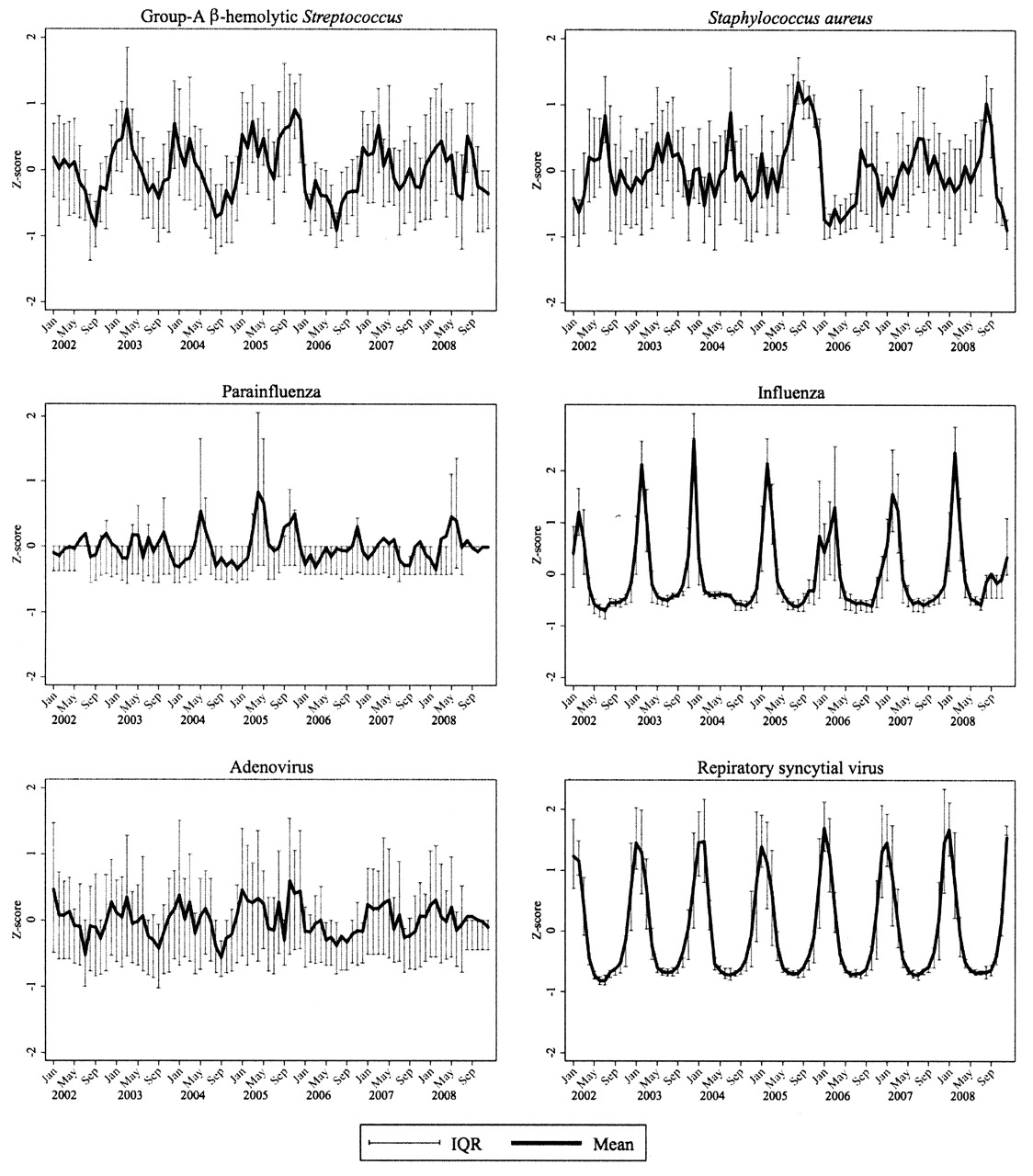
Hospitalizations for group A ß-hemolytic Streptococcus (GABS), S. aureus, parainfluenza, influenza, adenovirus, and respiratory syncytial virus (RSV). Data are Z scores and interquartile ranges (IQR) across hospitals for HSP admissions each month 2002–2008.
Subjects’ demographic data. Data are percentages.
Association of hospitalization due to HSP with hospitalizations due to group A ß-hemolytic Streptococcus, S. aureus, and parainfluenza
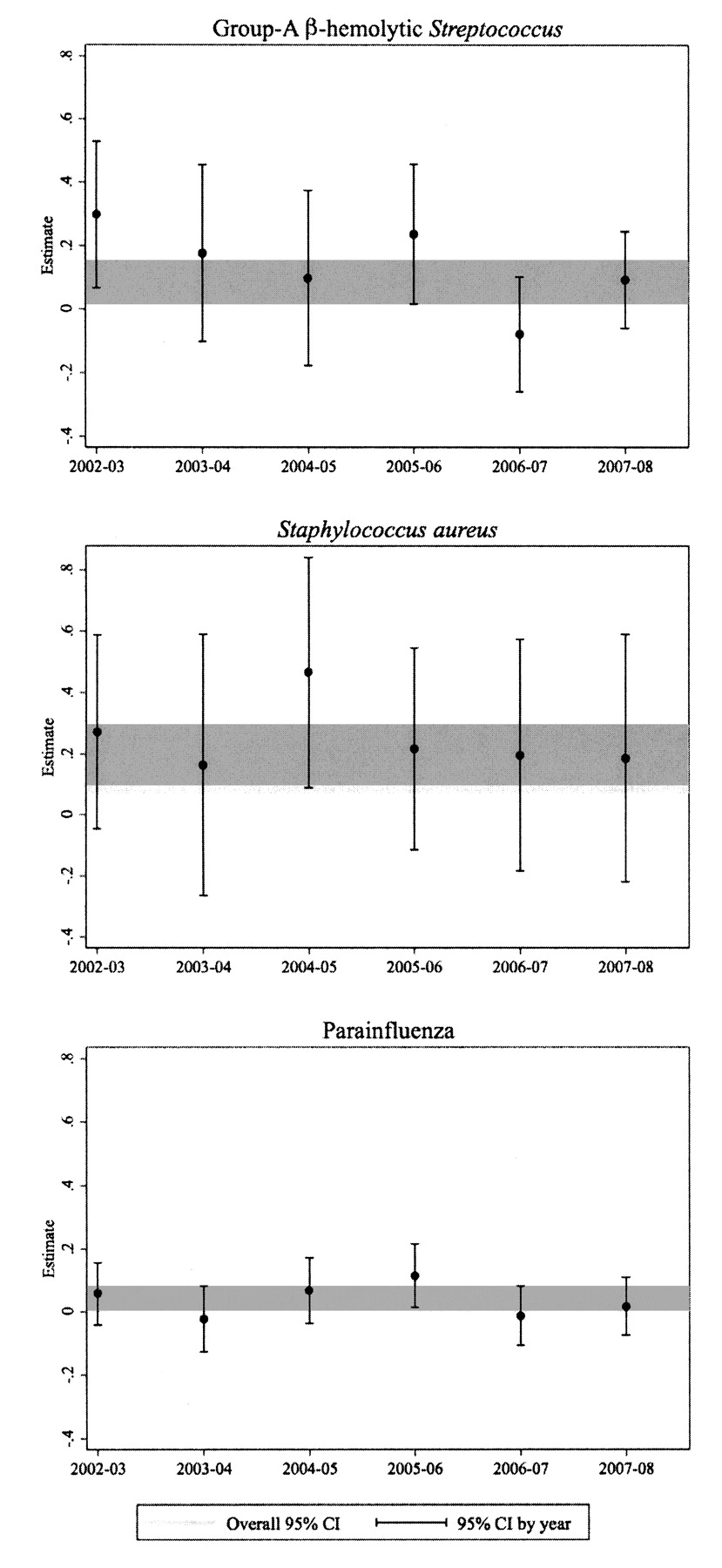
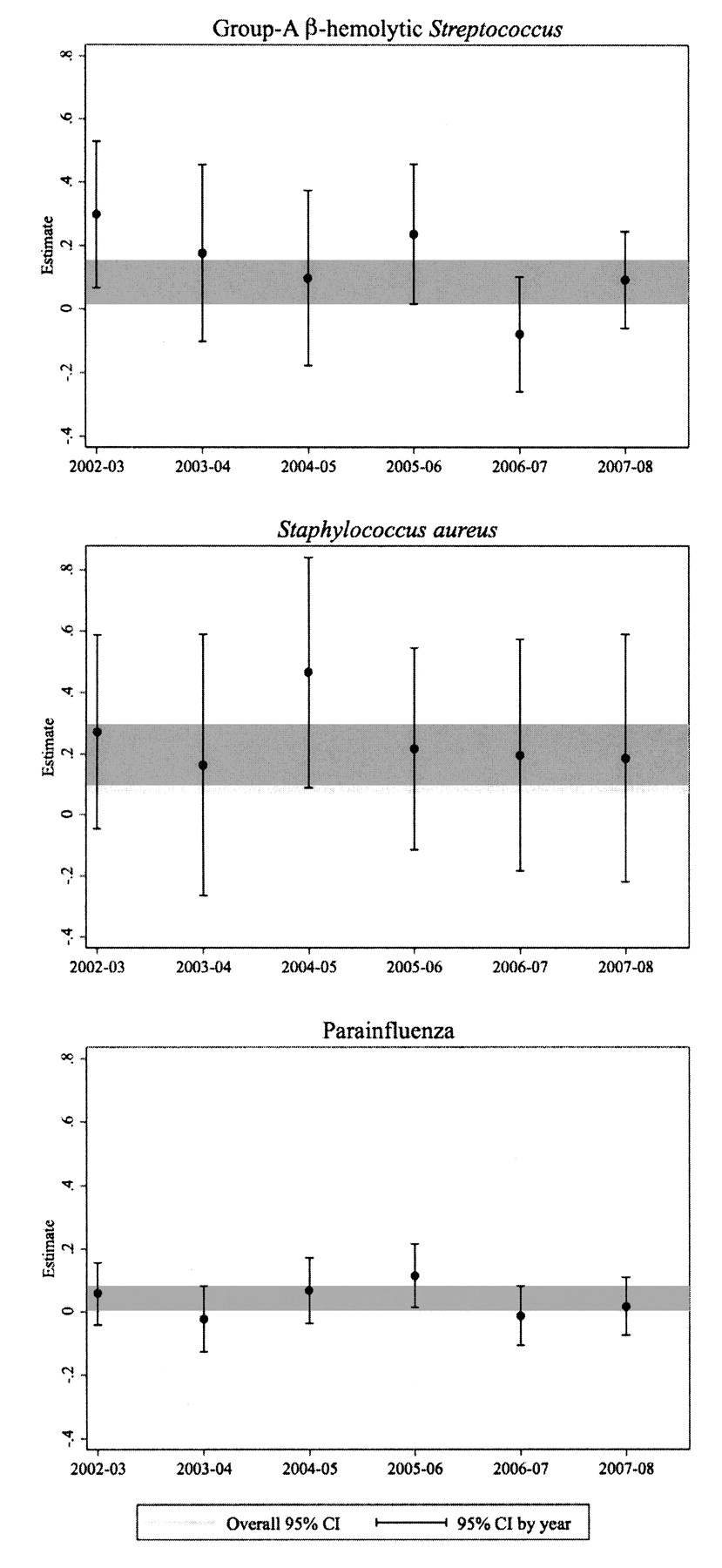
Accounting for the month by month differences within each hospital, HSP admissions in a given month increased significantly as admissions for GABS, S. aureus, and parainfluenza increased (Table 2). When S. aureus was subdivided into methicillin-sensitive S. aureus (MSSA) and methicillin-resistant S. aureus (MRSA) infections, both were significantly associated with HSP admissions. The association between HSP and GABS admissions was stronger for years 2002–03 and 2005–06 and weaker for 2006–07 (Figure 3). The association between HSP and S. aureus admissions was consistent across years, except for a slightly stronger association for 2004–05 (Figure 3). The estimate of association for HSP and parainfluenza was consistent across years (Figure 3). Overall, across all study years, there was no significant association between admission for HSP and several other infections with prominent peaks in the fall and winter including influenza, adenovirus, or RSV (Figure 2).
{kind=link}
{kind=link}
{kind=link}
Association of admissions for Henoch-Schönlein purpura and for group A ß-hemolytic Streptococcus (GABS), S. aureus, and parainfluenza 2002–2008. Data generated by ARMA(1,1) process; shaded area shows overall 95% CI.
Henoch-Schönlein purpura admissions associated with infection admissions. Estimates for the standardized rate of HSP admission were calculated using the autoregressive moving average (1,1) process for each infection.
DISCUSSION
This study demonstrates a significant temporal association between admissions for HSP and admissions for GABS, S. aureus, and parainfluenza in US children’s hospitals from 2002 to 2008. The positive association with GABS is in accord with the observations of smaller pediatric cohort studies at single institutions18,19,20,21. Similarly, positive association of HSP with S. aureus22,23,24,25,26,27 has been reported in single-center small case series or case reports. To our knowledge an association of HSP and parainfluenza has never been reported. This study surpasses existing reports by examining the relationship of multiple upper respiratory agents in a rigorous, large, multicenter approach.
The demographics of children with HSP in this study are similar to those reported in previous studies9,11,28,29. Our results should be interpreted with the knowledge that only the most seriously ill children with HSP and the most seriously ill children with these infections were evaluated. However, these are often the children with whom physicians are most concerned. We acknowledge that management of HSP and treatment of the infections evaluated are done on an outpatient basis most of the time. Future studies should test if the correlations remain significant when the milder forms of HSP and the infections are included. Despite these considerations, our findings indicate that the association of GABS, S. aureus, and parainfluenza and HSP, particularly for the most severely ill patients, warrants additional study.
Time series analyses are increasingly used in epidemiology research12,30,31. The PHIS database offered a unique opportunity to evaluate the association of HSP and each of the infections because each peaked at different times in different areas of the US, as demonstrated by the wide interquartile range for each condition for each month in Figure 2. In this study we analyzed data month by month at each of the 40 hospitals, and found a tight level of association down to the very local and small time scale. With this level of detail we discern that while influenza, adenovirus, and RSV wax and wane with the seasons, their outbreak epidemiology has no relation to HSP, whereas the hospital-specific monthly rates of GABS, S. aureus, and parainfluenza are highly associated with each hospital’s rate of HSP cases.
Importantly, the association of HSP and GABS, S. aureus, and parainfluenza has biologic plausibility, as each is associated with other autoimmune diseases in genetically susceptible individuals. The reasons for the link between infection and autoimmunity are unclear, but may relate to continued presence of the infectious organism itself, residual antigen from the infection, or self-antigen.
GABS is capable of causing a broad spectrum of postinfectious autoimmune diseases, with rheumatic fever being the paradigmatic example. Other autoimmune conditions that GABS is associated with include movement disorders (chorea, tics, Parkinsonism)32, Behçet’s disease33, and polyarteritis nodosa34. The immunopathogenesis of these diseases is incompletely defined but may be due, at least for some of the cases, to molecular mimicry (whereby, in the example of rheumatic fever, host antibodies to the GABS M-protein peptides also recognize host tissue components, namely peptides on the cardiac valves). In other conditions such as Guillain-Barré syndrome35,36 and antiphospholipid syndrome37,38 more than one organism can trigger the immune response, apparently resulting in molecular mimicry and subsequent disease. Similar mechanisms may also be at work in the pathogenesis of HSP, given the positive association of HSP with multiple infectious agents in our study and in the literature.
Similar to GABS, S. aureus is implicated in the pathogenesis of autoimmune diseases, including vasculitis. The pathogenesis of Kawasaki disease, a medium-size vessel vasculitis, is incompletely understood but an abnormal immune response to various microbes and superantigens derived from S. aureus have been suggested39. Additionally, chronic nasal carriage of S. aureus significantly increases the risk of disease relapse in WG40, an antineutrophil cytoplasmic antibody (ANCA)-associated small-vessel vasculitis. Theories to explain the underlying relationship between S. aureus and WG include superantigens41,42, polyclonal activation by cell wall components40, S. aureus binding of 1-antiproteinases resulting in persistent antiproteinase 3 (the antigen target of ANCA in WG)43, and molecular mimicry44.
Parainfluenza has not been as frequently reported in association with autoimmunity as GABS and S. aureus, but reports do exist, particularly with vasculitis. Association of antiparainfluenza IgM antibodies and the onset of giant cell arteritis and polymyalgia rheumatica has been reported45. Additionally, associations between parainfluenza and Kawasaki disease46,47 and mucocutaneous lymph-node syndrome have also been reported. In these diseases viral replication within the endothelium may cause vessel injury, which is important in the pathogenesis of vasculitis48,49.
To conclude, in pediatric tertiary care hospitals across the US, there is a positive association between admissions for HSP and for GABS, S. aureus, and parainfluenza. Our results provide preliminary evidence of a temporal, but not necessarily causal, relationship for the most severe subset of children with HSP that should be further examined in a prospective manner to investigate causality. If causality is proven, it is plausible that the association between these infections and development of HSP may be mediated through various mechanisms including molecular mimicry, superantigen production, and endothelial injury. Additional basic and clinical studies are warranted (1) to investigate if similar associations are present in the outpatient setting; (2) to test for causality using a prospective study design; (3) to elucidate the molecular basis by which HSP is associated with these infections; and (4) to explore whether clinical outcomes vary with different infectious triggers and early treatment of these infections.
Footnotes
-
Dr. Weiss was supported by the American College of Rheumatology Research and Education Foundation Clinical Investigator Fellowship Award.
- Accepted for publication July 27, 2010.
Appendix
ICD-9-CM codes used for infections of interest and Henoch-Schönlein purpura.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.