
Abstract
Objective. A CD30-CD153 mast cell axis has been described in skin inflammations and Hodgkin’s lymphoma. We investigated if a soluble form of CD153 is present in the serum and synovial fluid (SF) of patients with rheumatoid arthritis (RA), and determined whether mast cells express CD153 in the synovium of these patients.
Methods. Soluble forms of CD30 and CD153 were quantified in serum and SF of patients with RA by ELISA. Consecutive sections of synovial biopsies from 12 patients were stained against tryptase (mast-cell marker), CD30, and CD153.
Results. Elevated concentrations of the soluble form of CD153 were found in serum from 14/15 RA patients. In the SF, 11/20 patients had detectable levels of soluble CD153. CD30 and CD153 were expressed in all biopsies that were studied. Mast cells were present in all the synovial biopsies, and expressed CD153 in one-third of the cases.
Conclusion. We observed that CD153 was expressed in the synovium of patients with RA and we were able to correlate the serum levels of soluble CD153 with SF levels in the same patients. Because CD30 can activate mast cells to release chemokines without degranulation, our finding that mast cells express CD153 in RA synovium raises the possibility that a CD30-CD153 axis may contribute to the activation of synovial mast cells in the absence of degranulation.
- CD153
- CD30
- MAST CELL
- RHEUMATOID ARTHRITIS
Rheumatoid arthritis (RA) is an autoimmune disorder characterized by chronic inflammation, cartilage destruction, bone erosion, and changes in joint integrity and function. Although widely studied, its cause and pathophysiological process remain unclear. Mast cells are immune cells that are commonly designated as body sentinels due to their localization at sites prone to infection and to their capacity to rapidly release a considerable quantity of mediators upon activation. Among the mediators released are proinflammatory mediators such as histamine, prostaglandins, leukotrienes, proteolytic enzymes, tumor necrosis factor-α(TNF-α), and other multifunctional cytokines (reviewed by Mekori and Metcalfe1). Mast cells are described as important agents in several inflammatory disorders, including RA2,3. The mast cell population in the synovium of RA patients has long been known to be elevated, and this has caught researchers’ attention given their potential to release proinflammatory mediators4–6. Indeed, between 10% and 15% of mast cells in the rheumatic synovium appear to be degranulated7, and mast cell mediators such as histamine and tryptase can be detected in the synovial fluid (SF)8–10, suggesting that they are activated and have released the proinflammatory mediators stored in their granules. Mast cells present at sites of cartilage erosion are associated with the microenvironmental expression of proinflammatory cytokines and metalloproteinases by neighboring cells11. Strong evidence for involvement of mast cells in inflammatory arthritis was obtained from the K/B×N arthritis model12, where wild-type mice, but not mast cell-deficient mice, developed arthritis13. Most important, this was overcome by engraftment of mast cell-deficient mice with wild-type mast cells13, implicating mast cells as key agents in the onset of the disease.
The costimulatory molecule CD30 and its ligand CD153 (CD30 ligand; CD30L) are members of the TNF receptor (TNFR) and TNF superfamilies, respectively14,15. CD30 consists of a 120-kDa type I membrane-bound glycoprotein that was first described as a marker for Hodgkin and Reed-Sternberg cells16, but was later found to be expressed in other non-Hodgkin’s lymphomas17, Th2 cells18,19, and Th1 and Th0 cells20,21. Its extracellular domain can be proteolytically cleaved by a zinc-metalloproteinase, originating a soluble form of the molecule, sCD3022. sCD30 is normally absent, or present at very low levels, in the serum of healthy people, but in patients with Hodgkin’s lymphoma23,24 and some inflammatory disorders, such as atopic dermatitis25 and RA26, increased levels of circulating sCD30 have been reported. Activation by CD30 results in translocation of nuclear factor-κB to the nucleus, where it has been shown to activate genes involved in the regulation of the cell cycle, proliferation, or apoptosis (reviewed by Horie and Watanabe27).
CD153 is a 40-kDa type II membrane glycoprotein expressed on activated T cells and macrophages as well as on B cells, mast cells, neutrophils, eosinophils, and various cancer cells15,28–31. CD153 has the capacity to induce CD30 expression and shedding and proliferation of CD30+ T cells, and is also capable of reverse-signaling via its N-terminal cytoplasmic tail32. Cross-linking of CD153 in T cells and neutrophils induces gene expression and increases the cellular metabolic activity32. We have previously shown that mast cells express functional CD15333. CD30 activation of cord blood-derived mast cells (CBMC) results in a degranulation-independent activation of CBMC, with release of the newly formed proinflammatory cytokines IL-8, macrophage inflammatory protein-1αand 1ß, and monocyte chemoattractant protein-134. We have also demonstrated that mast cells constitute the predominant CD153-positive cells in the CD30-associated diseases Hodgkin’s lymphoma, atopic dermatitis, and psoriasis33,34.
Increased concentrations of sCD30 have previously been found in the serum of patients with inflammatory diseases. Elevated levels of sCD30 were found in the serum and SF of RA patients26,35. It has also been shown that serum levels of sCD30 are higher in the early stages of RA35. In addition, elevated serum levels of sCD30 correlated negatively with levels of C-reactive protein in patients with early RA, and correlated positively to the response to disease modifying antirheumatic drugs36. These findings suggest involvement of CD30+ cells in an antiinflammatory response in the early stages of RA35. To our knowledge, there are currently no studies on soluble CD153 in RA or any other disease.
We investigated the expression of CD153 by synovial mast cells and quantified the concentrations of sCD30 and sCD153 in the serum and SF of patients with RA.
MATERIALS AND METHODS
Patients.
Serum samples from 25 healthy controls and 15 patients with RA, and SF from 20 patients with RA, were collected. The majority of the patients were rheumatoid factor-positive, and 13 were treated with at least one of prednisolone, nonsteroidal antiinflammatory drugs, or methotrexate. Biopsies from the rheumatic synovium of 6 RA patients were collected at the time of surgery. Arthroscopic biopsies were also collected from 6 patients. All the RA patients fulfilled the 1987 diagnostic criteria of the American College of Rheumatology37.
Approval of the study was granted by the Ethics Committee at the Karolinska University Hospital, and all patients and control subjects gave informed consent.
Measurement of sCD30 and sCD153 by ELISA.
sCD30 and sCD153 were quantified in the serum and SF using commercial ELISA kits (Bender MedSystems GmbH, Vienna, Austria) according to the manufacturers’ instructions. The detection limit of each ELISA was 0.33 U/ml for sCD30 and 0.5 ng/ml for sCD153.
Immunohistochemistry and immunofluorescence.
For immunohistochemistry we used a mouse monoclonal anti-CD30 antibody (Dako Cytomation, Copenhagen, Denmark), mouse monoclonal anti-CD153 antibody (R&D Systems, Minneapolis, MN, USA, or BD Biosciences, San Jose, CA, USA), and a rabbit polyclonal antitryptase antibody38, in consecutive sections of synovial biopsies collected at surgery from 6 different RA patients. Sections were selected from an area of active inflammation. Anti-human CD30 and CD153 antibodies were diluted to 5 μg/ml and anti-human tryptase antibody was diluted 1:40,000 in phosphate buffered saline (PBS) with 0.1% saponin. The avidin-biotin-peroxidase (ABC) technique using the Vectastain Elite ABC kit (Vector Laboratories, Burlingame, CA, USA) was used to amplify the signal. Unrelated mouse immunoglobulins and rabbit serum were used as controls at the same concentration as the specific antibodies. Sections were visualized with a Reichert Polyvar 2 microscope.
Colocalization was performed using the same antibodies in arthroscopic sections from the same patients. Anti-mouse biotinylated antibody (Immunkemi, Järfälla, Sweden) was added (1:600 in PBS + saponin) followed by incubation with streptavidin-conjugated Alexa 488 antibody (1:600; Molecular Probes, Eugene, OR, USA). After blocking for streptavidin/biotin, anti-rabbit biotinylated antibody (Immunkemi) was added (1:800) followed by incubation with diluted (1:500) streptavidin-conjugated Alexa 546 antibody (Molecular Probes). Sections were visualized on a Leica fluorescence microscope.
Statistical analysis.
Statistical analysis was performed using GraphPad Prism 4.03. Serum levels of sCD30 and sCD153 were compared to healthy control levels using the Mann-Whitney test, assuming a nonparametric and nonpaired distribution of both groups. sCD30 and sCD153 levels in both serum and SF were correlated using Spearman rank-order coefficient (Rs). A nonparametric distribution of the 2 variables was assumed.
RESULTS
Quantification of sCD30 and sCD153 in RA serum and synovial fluid.
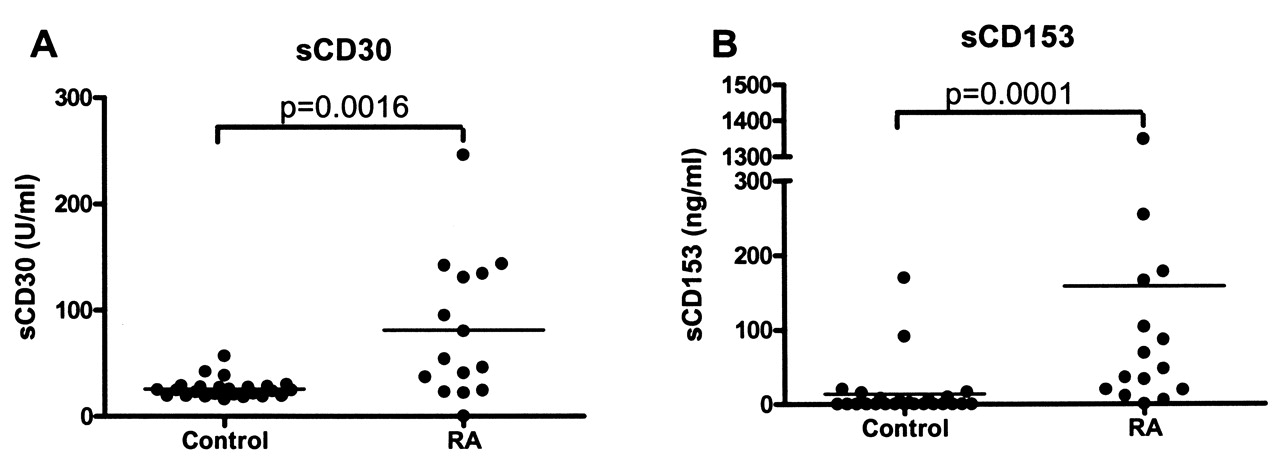
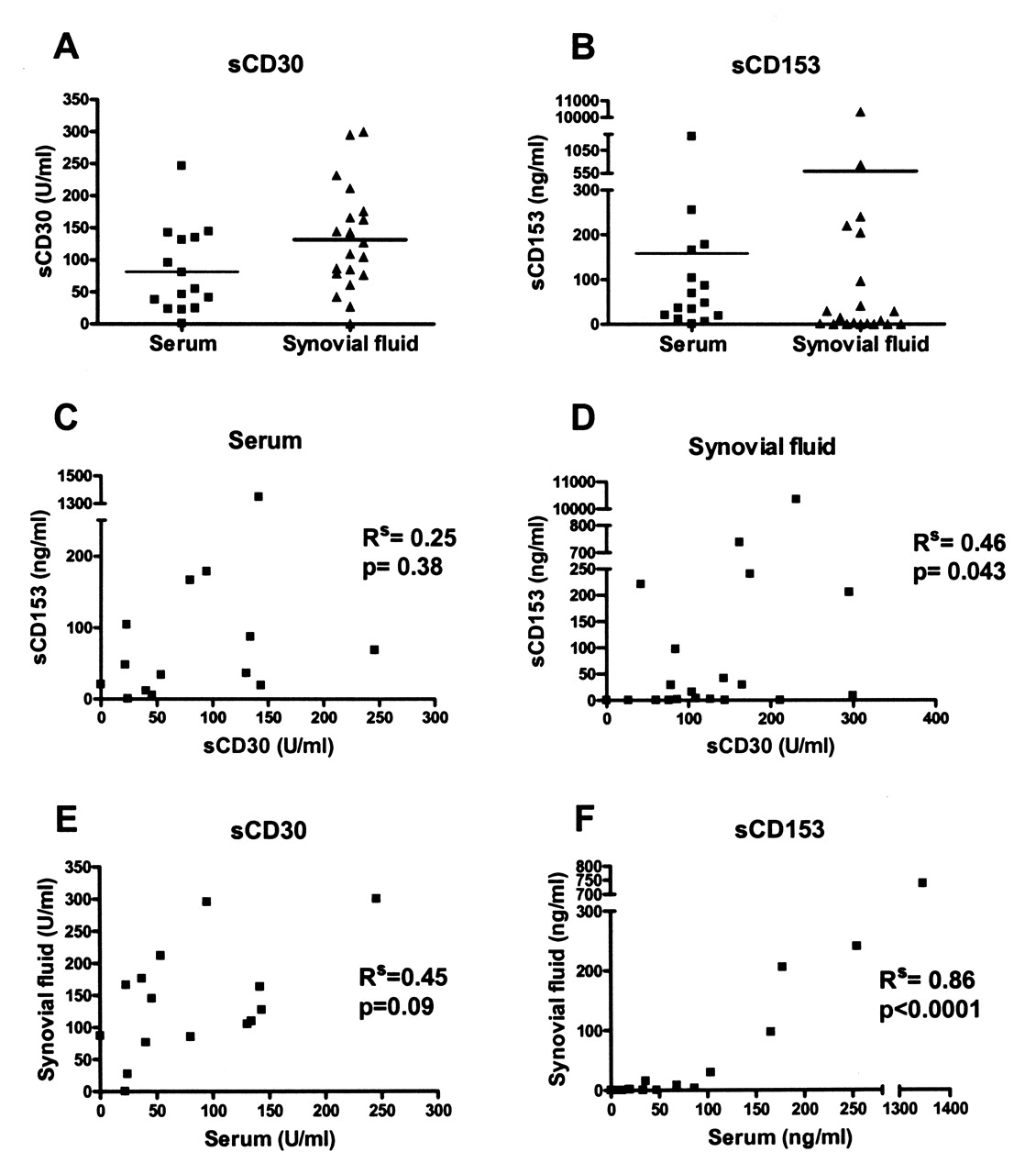
Soluble CD30 has been shown to be present in RA serum and SF26; however, there are currently no data about its ligand CD153. Serum concentrations of sCD30 and sCD153 were measured in 25 healthy controls and in 15 patients with RA (Figures 1, 2A, 2B). Levels of both sCD30 and sCD153 were significantly higher in RA patients compared to controls. In the controls, the mean value of sCD30 was 25.8 U/ml (minimum 16.1, maximum 56.8 U/ml) and the mean value of sCD153 was 13.72 ng/ml (minimum below the detection limit, maximum 169.7 ng/ml). In the sera from RA patients the mean value of sCD30 was 81.3 U/ml (minimum below the detection limit, maximum 246.0 U/ml) and the mean value of sCD153 was 158.5 ng/ml (minimum below the detection limit, maximum 1348.4 ng/ml). sCD30 and sCD153 levels were also quantified in SF samples collected from 20 RA patients (Figures 2A, 2B). sCD30 was expressed at detectable levels in 19/20 patients, with a mean value of 131.4 U/ml (minimum below the detection limit, maximum 246.0 U/ml), whereas sCD153 showed a more heterogenic pattern: sCD153 was measured in 11 out of 20 of the SF samples, with a mean value of 598.6 ng/ml (minimum below the detection limit, maximum 10.3 μg/ml).

sCD30 and sCD153 quantification in serum from healthy controls and patients with RA (both groups compared by Mann-Whitney test). A. sCD30: mean value in control serum was 25.82 U/ml and in RA 81.3 U/ml. B. sCD153: mean value in control serum was 13.72 ng/ml and in RA 158.5 ng/ml.
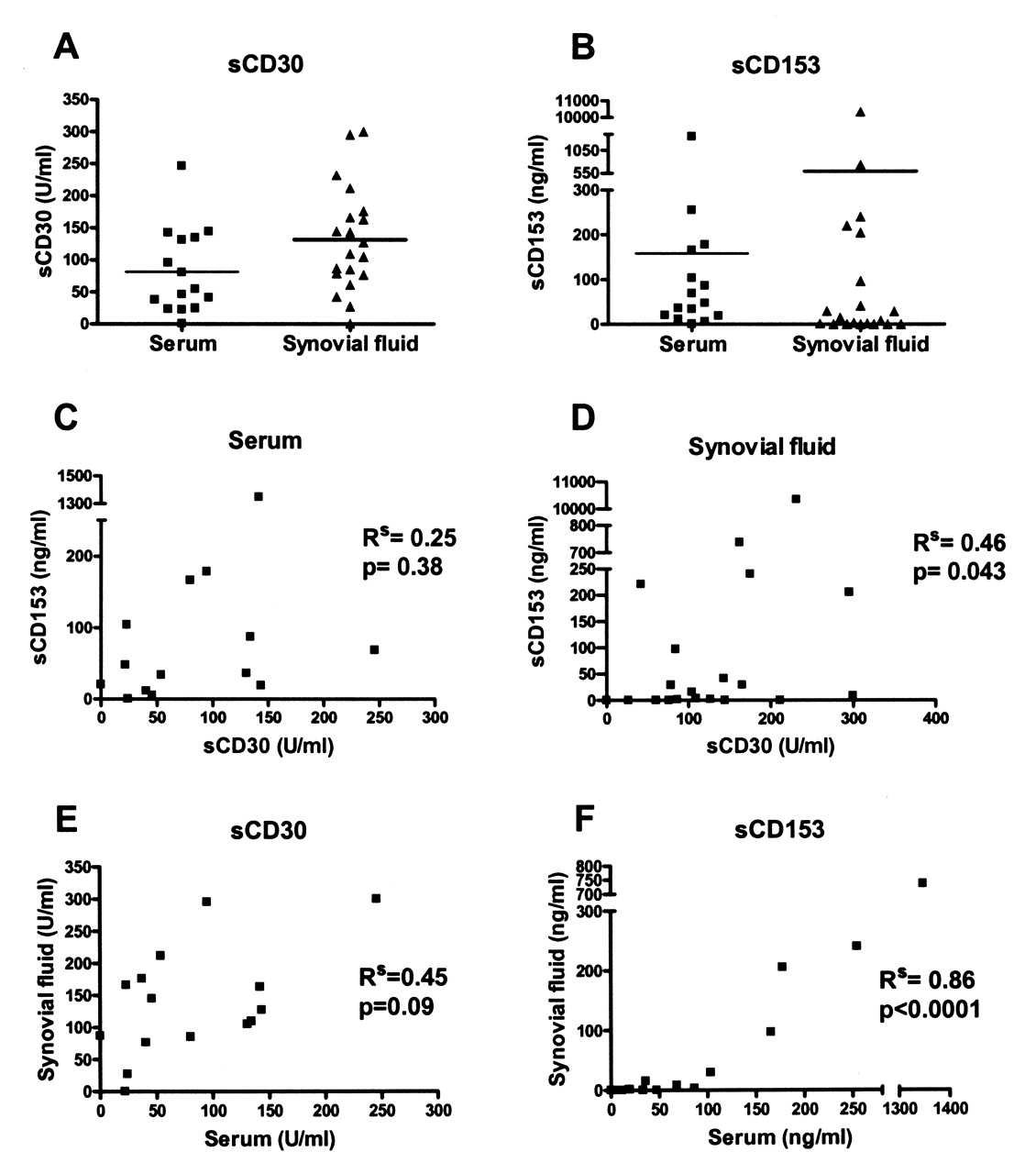
sCD30 and sCD153 quantification in serum and SF from patients with RA. A. sCD30: mean value in serum was 81.3 U/ml and in synovial fluid 131.4 U/ml. B. sCD153: mean value in serum was 158.5 ng/ml and in synovial fluid 598.6 ng/ml. C and D. Correlation between sCD30 and sCD153 in serum (C) and in synovial fluid (D). E and F. Correlation between serum and SF levels of sCD30 (E) and sCD153 (F). Rs: Spearman r.
The levels of sCD30 and sCD153, in both the serum and the SF, were compared to each other (Figures 2C, 2D). No statistically significant correlation between sCD30 and sCD153 was found in the patient serum. In contrast, in SF we found a statistically significant correlation between the levels of sCD30 and sCD153 (Spearman test, Rs = 0.46, p < 0.05). A statistically significant correlation was also observed (Figure 2F) when sCD153 levels in the serum and SF were compared (Spearman test, Rs = 0.86, p < 0.0001). No correlation was found when sCD30 levels in the serum and SF were compared (Figure 2E).
Expression of CD30 and CD153 in synovial tissue.
RA knee synovial biopsies were collected by arthroscopy or surgery. CD30, CD153, and tryptase were detected by immunohistochemistry in consecutive sections from these patients, as shown in Table 1.All the sections stained positive for CD30, CD153, and tryptase, and some patients showed higher levels of these proteins than others. Figure 3 shows stainings of biopsies collected by arthroscopy from Patients H and I shown in Table 1. Mast cells are present in synovium sections from both patients, as shown by the tryptase staining. CD30 and CD153 are also expressed in Patient I and Patient H, but to different degrees. Together, these results show there is a high degree of heterogeneity in the expression of these different proteins between patients.

CD30, CD153, and tryptase expression in synovial biopsies obtained from 2 patients by arthroscopy. Section from Patient H shows lower expression of CD30 and CD153 than in Patient I, as well as lower number of mast cells, as observed by the number of tryptase-positive cells.
Expression of CD30, CD153, and tryptase in synovial tissue collected at surgery (Patients A–F) and by arthroscopy (Patients G–L).
Based on previous studies from our group, where we described that mast cells are the predominant CD153- expressing cells in Hodgkin’s lymphoma33 and inflammatory skin diseases34, we investigated the expression of CD153 on mast cells in the synovial tissue using immunofluorescence. We observed that in one-third of the patients, mast cells expressed CD153 (Figure 4), whereas in the other twothirds CD153 was observed in other cells (data not shown), but not in mast cells. Thus, the expression pattern of CD153 in RA is much more heterogeneous compared to other inflammatory diseases previously investigated33,34.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Colocalization of CD153 and tryptase by immunofluorescence. RA synovial biopsy stained for (A) CD153 (green) and (B) tryptase (red) shows the presence of double-positive cells (C) in yellow.
DISCUSSION
Our study focused on quantification of sCD153 in serum and SF from patients with RA and in CD153-expressing cells in the rheumatic synovium. Increased concentrations of sCD30 have been found in several inflammatory diseases27. sCD30 has been shown to be increased in the serum of RA patients compared to healthy controls26, and its presence was also noted in the SF, as confirmed in our study (Figures 1 and 2A). Increased levels of sCD30 have been correlated to a better response to second-line treatment in early RA36, where a specific subset of preactivated CD30+ T cells seems to be involved in the control of the inflammatory response35. sCD30 has been shown to decrease CD153 expression by peripheral blood lymphocytes and inhibit CD153-mediated apoptosis39. CD30 expression is upregulated in preactivated T cells cocultured with transgenic CD153-expressing cells40, which shows that CD153-expressing cells might have a role in the development of T-lymphocyte-associated diseases. In addition, cross-linking of CD153 in T cells induces proliferation and cytokine production, further supporting this hypothesis32. The physiological role of sCD30 remains to be determined.
Our finding that sCD153, the ligand for CD30, is also present in high concentrations in RA patient serum (Figures 1B, 2B) suggests an upregulation of the CD30-CD153 pathway in the synovium, and this is further substantiated by the presence of sCD153 in the SF of more than 50% of samples we analyzed (Figure 2B). Several different mediators can be released upon in vitro activation of different cells via the CD30-CD153 pathway41, which can result in inflammatory cell recruitment and spreading of the inflammatory condition. In vitro studies have shown that CD153 has the capacity not only to induce CD30 expression in preactivated T cells, but also to induce CD30 release from these cells40. The positive correlation observed between sCD153 levels in the serum and in SF (Figure 2F) is an indication for a common origin in the patients where both molecules are detected in serum and SF. As shown in Figure 3 and Table 1, CD153 is present at high levels in the synovium of RA patients. We can speculate that the sCD153 found in the RA SF and serum might originate from CD153-expressing cells resident in the synovium of inflamed joints. The presence of soluble forms of CD30 and CD153 is an indication for biological activity of this pathway, but further studies are needed to confirm this.
Most members of the TNF family are expressed as membrane- bound forms, but some can be cleaved by specific proteases and thus release a soluble active form42. This soluble form is capable of exerting its activity by binding to the receptor without the need for cell-cell contact. For example, soluble Fas ligand is capable of inducing apoptosis in epithelial cells43. Soluble BAFF (B-cell activating factor belonging to the TNF family) induces proliferation of antiimmunoglobulin M-stimulated peripheral blood B lymphocytes44. To date, there are no reports about sCD153 or a protease that specifically cleaves CD153. We found elevated levels of sCD153 in the serum and SF of patients with RA. Based on what is known about other soluble molecules of the TNF family, it is possible that this soluble form is capable of binding and activating cells expressing its receptor, CD30, and thus exerting its function on distant cells. Since CD30-positive cells in RA appear to have an antiinflammatory effect, by releasing interferon-γand interleukin 435, it is possible that the presence of sCD153 is an attempt to stimulate the population of CD30-expressing cells to release these antiinflammatory cytokines and downregulate the inflammation.
Although it has long been known that mast cell numbers are increased in the inflamed synovium of patients with RA6 and that mast cell mediators are present in the SF8, their contribution to the pathogenesis of the disease is still not clear. They have the potential to release a vast variety of mediators that have the potential to facilitate synovial inflammation by increasing vascular permeability, recruiting other leukocytes, activating fibroblasts/chondrocytes and B and T lymphocytes, and promoting angiogenesis, among other functions (reviewed by Nigrovic and Lee45). One characteristic of mast cell activation is the release of its cytoplasmic granules. In inflamed synovium the number of degranulating mast cells is substantially higher than in normal synovium46,47. Despite this degranulation-dependent activation, where important molecules such as tryptase, histamine, or TNF are released, we have previously shown that mast cells can be activated by CD30 without induction of degranulation34, releasing newly formed chemokines. Here we describe that some mast cells express CD153 in at least one-third of the patients analyzed (Figure 4), although mast cells are not the predominant CD153-expressing cells. Despite this, the presence of large numbers of CD30-positive cells in the inflamed synovium (Figure 3) and the high levels of sCD30 (Figure 2A) illustrate the potential for mast cell activation via CD153 whenever mast cells express it.
The expression of CD30/CD153 in the synovium and the levels of sCD30 and sCD153 in the SF and serum both showed very heterogeneous patterns. In patient material used for this study (< 20 patients) we could find no correlation between these indicators and treatment, clinical scores, or duration of disease. To be able to perform statistical analysis one would need more patients. However, we observed the novel findings that (1) the soluble form of CD153 can be detected in the serum and SF of patients with RA; and (2) some mast cells in one-third of the patients we analyzed expressed CD153, which is in sharp contrast to other CD30-associated diseases previously analyzed, where mast cells were the predominant CD153-positive cell in all patients33,34. Several cells express both CD153 and CD30 in the rheumatic synovium, where mast cells constitute a part of the CD153-positive cell population. Given the increasingly important role in the development of RA that is being attributed to mast cells, it is necessary to determine all possible mechanisms by which the mast cells can be involved in the disease. Activation via CD153 is a possible mechanism of activation of mast cells, but its importance in the context of RA remains to be clarified.
Acknowledgments
We thank Dr. Andreas Stark, Karolinska University Hospital, Stockholm, for providing us with specimens from surgery.
Footnotes
-
Supported by the Swedish Research Council – Medicine, The Swedish Association Against Rheumatism, King Gustaf V 80-Years Foundation, The Swedish Cancer and Allergy Fund, The Konsul Th C Berghs Foundation, Ollie and Elof Ericsson’s Foundation, the Ellen, Walter and Lennart Hesselmans Foundation, and Karolinska Institutet. R.F.S. Carvalho is supported by a Marie Curie Early Stage Research Training Fellowship of the European Union’s Sixth Framework Programme under contract number 504926.
- Accepted for publication October 14, 2008.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.