
Abstract
Objective. To evaluate the prevalence and pattern of arterial calcification in patients with asymptomatic systemic lupus erythematosus (SLE) compared with control subjects. SLE patients are prone to adverse cardiovascular events; however, the underlying atherosclerotic process is unknown. Multidetector computed tomography (MDCT) measured arterial calcium score (CS) reflecting underlying atherosclerosis and is closely associated with cardiovascular events.
Methods. Fifty age and sex matched SLE patients and controls were enrolled. All subjects underwent 64 slice MDCT scan to evaluate CS in coronary, carotid arteries and the aorta.
Results. As compared with controls, SLE patients had higher mean CS and prevalence of CS > 0 across all vascular beds. After adjustment for age and sex, SLE patient odds of having CS > 0 in any vascular bed was 33.6 (95% CI: 9.5–165.2) were higher versus patients in the control group, mainly due to more prevalent coronary calcification (OR 30.0, 95% CI: 6.7–203.8). In SLE patients, the most frequent vessel with CS > 0 was coronary (42%) followed by carotid artery (24%). Further, arterial calcification occurred early involving 40% of SLE patients at age < 40 years, with increasing prevalence as age advanced.
Conclusion. Our study confirms that patients with SLE have significantly higher prevalence and extent of systemic arterial calcification compared with age and sex matched controls.
- SYSTEMIC LUPUS ERYTHEMATOSUS
- VASCULAR CALCIFICATION
Systemic lupus erythematosus (SLE) is associated with an increased prevalence of subclinical atherosclerosis and cardiovascular events1,2. In female SLE patients aged between 35 and 44 years there was a 52-fold increased risk of having myocardial infarction as compared with age- and sex-matched healthy subjects1. Although the mechanisms for premature atherosclerosis are unknown, it is likely to be contributed by multiple factors, including immune-mediated damage, prevalent traditional cardiovascular risk factors, chronic inflammation, and prothrombotic factors3–6. With the use of electron beam computed tomography (CT), previous studies have demonstrated a higher prevalence of coronary calcification in SLE patients compared with age-matched controls7,8. As SLE is a systemic disease, the atherosclerosis related to SLE also likely involves the whole vascular system. Indeed, clinical ischemic events such as stroke and peripheral vascular disease are also more prevalent in SLE patients than in controls2,9. However, the extent and distribution of atherosclerosis in patients with SLE remains unclear.
Recent advances in multidetector computed tomography (MDCT) allows rapid, effective and noninvasive detection of extent and severity of atherosclerosis in different arterial beds by imaging calcified atherosclerotic plaque10,11. The purpose of our study was to investigate the distribution and extent of subclinical calcified atherosclerotic plaque in thoracic aorta and in coronary and carotid arteries using MDCT, in patients with SLE versus age-matched controls. In particular, we aimed to determine whether the prevalence and pattern of arterial calcification in asymptomatic SLE patients are different versus control subjects.
MATERIALS AND METHODS
Study population
To calculate the sample size needed for each group, we assumed the baseline prevalence of developing calcification in any vascular bed to be 0.5, and the prevalence of the control subjects to be about 25%. Using a one-sided test with a 0.05 level of significance with power of 0.8, we needed at least 46 subjects in each group. From January 2006 to January 2007, 50 consecutive Chinese patients age > 18 years who met classification criteria for SLE12 and suffered from the disease for at least one year were enrolled. Further, 50 age- and sex-matched controls who did not meet classification criteria for SLE or another inflammatory disease were also recruited as controls from a local health check program. No study subject had a history of cardiovascular diseases, including stroke, myocardial infarction, peripheral vascular disease, and angina. The study was approved by the institutional ethical review board, and all subjects gave their written informed consent.
Study protocols
Data on baseline demographic and clinical characteristics and blood sampling were obtained prospectively in the same day from study subjects. Cardiovascular risk factors, including tobacco smoking, diabetes mellitus, hypercholesterolemia, and hypertension were assessed. Body height and weight, blood pressure and body mass index of all subjects were measured as described13,14. Hypertension was defined as either resting systolic or diastolic blood pressure ≥ 140/90 mmHg at 2 different times or on medications. Diabetes mellitus was defined as a serum fasting glucose of ≥ 7.1 mmol/l or on oral hypoglycemic agent. Hypercholesterolemia was defined as a fasting total serum cholesterol level of ≥ 4.9 mmol/l or on medications. Smoking status was recorded as either smoker (past and current) or nonsmoker. A family history of coronary artery disease was defined as a first-degree relative having a myocardial infarction or stroke before age 55 years in men and age 65 years in women. For patients with SLE, demographic data including sex, age at onset of SLE, duration of disease, cumulative clinical manifestations, immune profiles including anti-double stranded DNA antibodies (anti-dsDNA), C3 and C4 levels; and their current and prior use of medications were retrieved from the patients’ medical record.
Fasting blood samples were obtained from all subjects to determine serum creatinine, glucose, and lipid levels. C-reactive protein (CRP) level was measured by using a Hitachi 747 analyzer (Boehringer Mannheim, Mannheim, Germany), and a particle-enhanced immunoturbidimetric assay (Roche Diagnostics, Mannheim, Germany) as described13.
MDCT imaging
All subjects underwent CT imaging of coronary, carotid artery and aorta using a 64 slice MDCT (Lightspeed, VCT, GE Healthcare, xxxx USA). In brief, all scans were performed with subjects in supine position, which included regions from the arch of the aorta to the fundus of the heart. Prospective electrocardiogram-gated cardiac scan was obtained with the following scan variables: rotation time = 0.35 s; slice thickness = 2.5 mm; 120 kV; 250 mA; trigger delay = 70% R-R interval. Carotid artery scan was performed from the level of C6 vertebral body to C2 vertebral body with following variables: rotation time = 0.35 s; slice thickness = 2.5 mm; 120 kV; 250 mA; trigger delay = 70% R-R interval. Aorta scan included the ascending aorta, aortic arch, and proximal 10 cm of the thoracic descending aorta. Patients were instructed to hold breath for 30 s during scanning.
The acquired MDCT images were reviewed at the post-processing image workstation (Advantage windows 4.02, GE Healthcare). Complete data were available from all scans, with no misregistration of slices due to artifacts of motion, respiration, or asynchronous electrocardiographic triggering. To ensure continuity and consistency of interpretation of calcium scores (CS), 2 expert investigators (SW, GCO), who were unaware of subjects’ clinical status, analyzed all scans. The interobserver and intraobserver variability correlation coefficients of CS measurements were 0.92 and 0.91, respectively.
Analysis of MDCT CS
Measurement of CS was performed by a commercially available software “smart score” (GE Healthcare) using the threshold option set for pixels > 130 Hounsfield units and expressed in Agaston units. Coronary CS was calculated as sum of CS in the left main coronary artery, left anterior descending artery, left circumflex coronary artery, right coronary artery, and posterior descending artery. Carotid artery CS was calculated as the sum of CS in carotid arteries including common carotid artery, internal carotid artery, and bulb. Aortic CS was defined as sum of CS in ascending and descending thoracic aorta in the scanning region. Total CS is the summation of coronary, carotid, and aortic CS.
Statistical analysis
Continuous variables were presented as mean ± standard deviation or median (IQR) as appropriate. Categorical data were presented as frequencies and percentages. Mann-Whitney U test was used to evaluate statistical differences of continuous variables and Fisher’s exact test was applied to test for statistical associations between 2 categorical variables. Logistic regression analysis was used to evaluate the odds ratios (OR) of having coronary, carotid, aortic and total CS > 0 in SLE patients to the control subjects, after adjusting for age and sex. Spearman’s rank correlation test was used to evaluate the correlation between CS and disease duration of patients. All statistical analyses were performed using the statistical package SPSS for windows (Version 15.0, SPSS, Chicago, IL, USA). P value < 0.05 was considered to be statistically significant.
RESULTS
Clinical characteristics
Demographic characteristics of the study populations are shown in Table 1. The majority of SLE patients and controls were female. For patients with SLE, their mean duration of disease was 14.2 ± 8.0 years and the mean anti-dsDNA level was 21.7 ± 41.7 IU/ml. There were no significant differences in age, sex, prevalence of hypertension, hyperlipidemia, smoking, diabetes, and family history of coronary artery disease between SLE patients and controls (Table 1, all p > 0.05). Both groups have similar prevalence of family history of medical illness (Table 1, p > 0.05), except that patients with SLE had a significantly higher prevalence of family history of SLE than the controls (22% vs 0%, p = 0.001).
Clinical characteristics of study subjects.
Prevalence and extent of vascular calcification
Table 2 summarizes the coronary, carotid, aortic, and total CS in patients with SLE and controls. For the presence of calcification in different vascular beds, SLE patients had the highest prevalence of CS > 0 in the coronary arteries, followed by carotid, and aortic arteries. Similarly, controls had the highest prevalence of CS > 0 in the coronary arteries, but followed by the aorta, and with no calcification in the carotid artery.
Prevalence and extent of calcium scores in patients with systemic lupus erythematosus (SLE) and controls.
As compared with controls, patients with SLE had significantly higher mean coronary, carotid, aortic, and total CS (Table 2, all p < 0.05). Further, the prevalence of CS > 0 in coronary and carotid arteries, aorta, and overall arteries (total) was also significantly higher in SLE patients compared with controls. After adjusting for age and sex, SLE patients had a significantly higher odds of developing calcification in any vascular bed (OR = 33.6, 95% CI: 9.5–165.2) mainly driven by a high frequency of coronary calcification (OR = 30.0, 95% CI: 6.7–203.8) (Table 2).
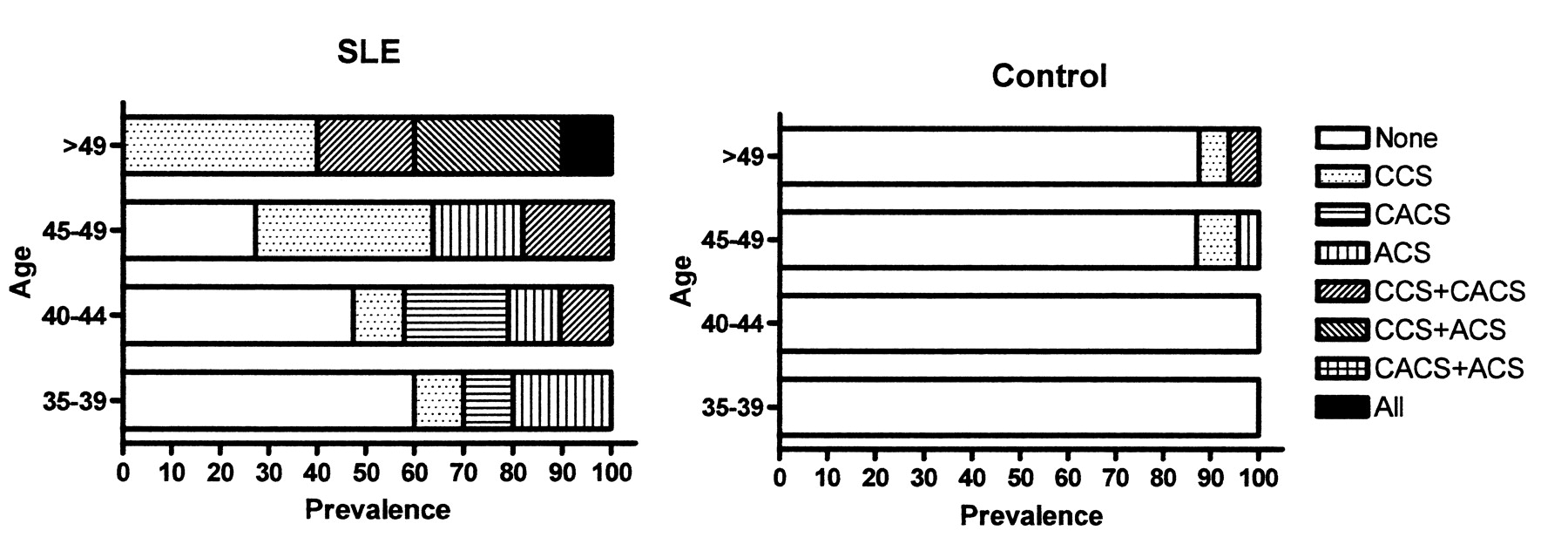
Figure 1 shows the distribution and prevalence of calcification (CS > 0) as stratified by vascular bed and age category (35–39, 40–44, and 45–49, and over 50 years). The prevalence of calcification across different age groups was significantly higher in patients with SLE compared with controls (all p < 0.05). In addition, simultaneous presence of calcification over thoracic aorta, coronary, and carotid arteries was observed only in patients with SLE and not in control subjects (Figure 1).
{kind=link}
Prevalence and distribution of vascular calcification, by age group, in patients with SLE and in controls and patients with SLE.
In the control group, calcification was only observed in patients aged > 45 years and clustered in the coronary arteries (Figure 1). In contrast, a significant proportion (40%) of SLE patients had arterial calcification even at age < 40 years, and this prevalence is even higher than in subjects aged > 49 years in the control group (~10%). For SLE patients > 49 years old, all had coronary arterial calcification, and 60% had calcification in 2 or more vascular beds (Figure 1).
Predictors for vascular calcifications in SLE patients
As shown in Table 3, SLE patients with vascular calcifications (i.e., total > 0) were significantly older, and had higher anti-dsDNA than those patients without any vascular calcification. However, there were no significant differences between the 2 groups in other cardiovascular risk factors, including prevalence of hypertension, hypercholesterolemia, smoking, diabetes, blood pressure, lipid prolife, medication, and inflammatory markers (Table 3, all p > 0.05). After adjusting for age and sex, hypertension, a higher anti-dsDNA and current use of azathioprine were found to be significant predictors for the occurrence of vascular calcifications in patients with SLE (Table 3). We further analyzed the data by evaluating individual predictors for coronary calcification. It was found that age (hazard ratio 1.40, confidence interval 1.14–1.72, p = 0.002) was the only variables associated with presence of coronary calcification but not with conventional cardiovascular risk factors, anti-dsDNA, or use of immunosuppressant.
Clinical characteristics of SLE patients with or without vascular calcification.
In SLE patients, total CS was significantly correlated with age and anti-dsDNA level (Table 4). Conversely, total CS was not correlated with body mass index, blood pressure, lipid profile, blood creatinine, and inflammatory markers.
Relationship between total calcium score and characteristics.
DISCUSSION
By using MDCT imaging of thoracic aorta, coronary, and carotid arteries, our study investigated the prevalence and extent of vascular calcification over multiple vascular beds in patients with SLE compared with age- and sex-matched controls. Our results extend previous observations on the occurrence of premature coronary atherosclerosis in patients with SLE6–8, and further demonstrate that SLE patients had early onset of diffuse calcification over multiple vascular beds. The risk of vascular calcification in patients with SLE was 33.6 fold higher than control subjects after adjusting for age and sex. Moreover, the prevalence and extent of calcification over thoracic aorta and coronary and carotid arteries were significantly greater in patients with SLE than controls across all age strata. In this study, the prevalence of vascular calcification observed in SLE patients with age < 40 years was higher than those observed in controls age > 49 years old, and all SLE patients had vascular calcification at age > 49 years compared to 10% in age-matched controls. Further, coronary calcification was the most prevalent site for calcification in both patients with SLE and control subjects. This is in accordance with Allison, et al15, where coronary bed had the highest prevalence of disease at young age (< 50 years). Indeed, in our study, simultaneous presence of calcification over thoracic aorta and coronary and carotid arteries was observed only in SLE patients over the age of 49 years, suggesting a different and accelerated pattern of vascular involvement in the atherogenesis process related to SLE compared to that observed in normal controls.
Except for the presence of hypertension, conventional risk factors for atherosclerosis including history of smoking, diabetes mellitus and hyperlipidemia were not associated with vascular calcification in this study. This lack of association with conventional cardiovascular risk factors for the development of premature atherosclerosis has also been shown by others4,16, while others have shown the opposite17. Systematic inflammation and immune mechanisms have been increasingly recognized as important causes for premature atherosclerosis. In this study, the level of anti-dsDNA and current use of azathioprine predicted the presence of arterial calcification but not coronary calcification in patients with SLE. Kiana, et al17 also demonstrated that the level of anti-dsDNA did not independently predict the presence of coronary calcification. This finding highlights that the process of atherosclerosis related to SLE disease activity is more diffuse and widespread rather than limited to the coronary arteries. Therefore, the use of coronary calcification alone as marker for atherosclerosis may fail to disclose this association. Nevertheless, future studies are required to identify the potential predictors for vascular calcification in patients with SLE.
While coronary CS has been extensively studied regarding its relationship with coronary atherosclerotic burden18 as well as future cardiovascular events10,19, the assessments of calcification over thoracic aorta and carotid artery have not been adequately evaluated. Previous studies showed that carotid artery CS reflects the calcium content of plaques in the carotid artery20, which correlates with coronary CS21 and predicts the risk of stroke22. Similarly, thoracic aorta atherosclerosis has also been shown to be associated with coronary calcification23 and future risk of stroke and cardiovascular events11,24. Therefore screening of CS in carotid and thoracic aorta of patients with SLE in addition to coronary arteries may allow earlier detection of subclinical atherosclerosis and provide incremental values in identifying high risk patients for secondary prevention measures reducing cardiovascular events. The potential benefits of screening and secondary preventive measures, such as lipid lowering and aspirin therapy for prevention of subclinical atherosclerosis in patients with SLE need to be confirmed by future studies.
Study limitations
First, this was a cross-sectional observational study and the temporal relationship between inflammation related to SLE and occurrence of calcified atherosclerotic plaques could not be assessed. Second, detail clinical assessment of disease severity of SLE was not performed, and only serum C-reactive protein level was measured to determine degree of systemic inflammation. Third, non-calcified atherosclerotic plaques can be detected by MDCT and therefore we may not have been able to detect the exact atherosclerotic burden.
In conclusion, our study demonstrates that the prevalence and extent of vascular calcification over thoracic aorta and coronary and carotid arteries is higher in patients with SLE compared with age- and sex matched controls. Further, the coronary artery was the most prevalent vascular bed, with calcification in both SLE patients and normal controls. Our findings have important implications for the understanding of the premature atherogenesis process and provide a cornerstone for future studies in this regard.
Footnotes
- Accepted for publication May 19, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.