

Abstract
The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA)-Outcome Measures in Rheumatology (OMERACT) Psoriatic Arthritis (PsA) Working Group reported at the 2018 GRAPPA annual meeting on the outcome of the OMERACT 2018 Conference in Terrigal, Australia. The working group presented the endorsement of the 66/68 joint count for the assessment of peripheral arthritis and the provisional endorsement of the PsA Impact of Disease 12 questionnaire for the assessment of PsA-specific health-related quality of life in PsA randomized controlled trials and observational studies. In this report, the group presents its plan to seek OMERACT endorsement for outcome measures that address the domains of MSK disease activity for enthesitis and dactylitis, physical function, fatigue, and structural damage following the OMERACT Filter 2.1 methodology.
In 2018, the Outcome Measures in Rheumatology (OMERACT) updated and outlined a conceptual framework for core set development (Filter 2.1) that encompasses both patient-centered and intervention-specific information to improve the measurement of outcomes in randomized controlled trials (RCT) and longitudinal observational studies (LOS)1. The OMERACT Filter 2.1 has also distinguished 2 major components in outcome research: determining “what to measure” before deciding on “how to measure.” This 2-stage process consists of the development of a “core domain set” that identifies important domains of disease that should always be measured and then a “core outcome measurement set” that includes measurement instruments that match the domains of disease2.
In 2016, the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA)-OMERACT Psoriatic Arthritis (PsA) Core Set Working Group updated the core domain set for all RCT and LOS3,4. The updated PsA Core Domain Set includes musculoskeletal (MSK) disease activity (peripheral arthritis, enthesitis, dactylitis, and axial symptoms), skin disease activity (including nails), pain, patient’s global, physical function, health-related quality of life (HRQOL), fatigue, and systemic inflammation, with structural damage as a middle-circle domain required once during the development program of a PsA treatment4.
After the GRAPPA-OMERACT PsA Working Group established the core domain set, it began to develop a PsA Core Outcome Measurement Set5,6. In 2018, the working group was the first disease group to take an outcome measure of physical examination and a patient-reported outcome measure (PROM) through the OMERACT Filter 2.1 and obtain the OMERACT community’s endorsement of the 66/68 joint count and provisional endorsement of the Psoriatic Arthritis Impact of Disease 12 (PsAID12)7,8. This is a report of the working group’s presentation at the GRAPPA 2018 annual meeting in Toronto, Ontario, Canada, where the process and voting outcomes from the 2018 OMERACT meeting in Terrigal, Australia, were presented to the GRAPPA membership. Also, the next steps in completing the core outcome measurement set using OMERACT methodology were defined.
Summary of the First 2 Instruments Endorsed for PsA Trials
Dr. Alexis Ogdie and Dr. Ana-Maria Orbai presented the Filter 2.1 methodology that seeks to evaluate each instrument using the 4 pillars of OMERACT2, which include truth 1 (domain match), feasibility, truth 2 (numerical sense), and discrimination:
Truth 1, domain match: Is an instrument a good match to the domain intended to be measured?
Feasibility: How feasible is the instrument to use?
Truth 2, numerical sense: How truthfully does the instrument numerically match the domain or construct?
Discrimination: How responsive is the instrument to capture change in disease status?
Dr. Ogdie and Dr. Orbai presented the group’s evaluation of the existing evidence on PsA instrument properties through systemic literature reviews and data analyses from RCT; followed by Delphi processes undertaken in partnership with stakeholders (including patients, clinicians, methodologists, and payers); working group meetings; and discussion. The following is a summary of the data presented.
The GRAPPA-OMERACT group has conducted a comprehensive systematic literature review (SLR) of measurement properties of PROM for PsA9, which serves as the basis for instrument selection. After thoughtful deliberation, the working group decided to take 2 instruments with a high level of face validity through the new OMERACT Filter 2.1 appraisal: 1 physical examination instrument (the 66/68 swollen and tender joint counts) and 1 PROM (PsAID12), for measuring domains of MSK disease activity (peripheral joints) and HRQOL, respectively. Each instrument was evaluated by healthcare providers and patients for domain match and feasibility. Measurement properties of truth and discrimination for both instruments were critically appraised. A posthoc analysis of data from RCT was performed for the 66/68 joint counts. Data from 2 longitudinal cohorts10,11 in patients with active PsA who experienced changes in treatments were evaluated to support the longitudinal construct validity for the PsAID12. Data were not yet available from RCT for the PsAID12, because the PsAID12 was developed in 2014 and uptake lag is expected. Evidence was consolidated in the OMERACT summary of measurement properties (SOMP) tables and presented at the OMERACT 2018 conference7,8. The 66/68 joint count was fully endorsed as a PsA core instrument. Because of the lack of data from RCT, the PsAID12 received provisional endorsement as a PsA core instrument. The working group is committed to deriving evidence that may confirm discrimination for the PsAID12.
Future Work Plan
Domains prioritized for instrument appraisal
The GRAPPA-OMERACT Working Group will continue to work on the appraisal of instruments for each domain in the core set. The prioritized domains consist of MSK disease activity for enthesitis and dactylitis, physical function, fatigue, and structural damage. These domains were chosen because of their importance in clinical trials and the urgent need to standardize instruments that evaluate these domains, or because the relevant systematic review for instruments for the particular domain has been completed. Thus far, the working group has completed SLR of all PROM9 and of systemic inflammation12 with other SLR in progress. Additional core domains (pain, patient’s global, and skin disease activity) are being evaluated as part of dedicated working groups within OMERACT and the International Dermatology Outcome Measures.
Selection of instruments for individual domains
The OMERACT Filter 2.1 has given clear guidance of appraisal and evidence synthesis for individual instruments. However, often numerous instruments exist for a particular domain. For the selection of 1 or more appropriate instruments for appraisal, the working group has developed an instrument selection guide to facilitate the process (Figure 1). This guide consists of:
Formation of a working group for the particular domain. The domain working group members preferably consist of care providers or others with expertise in the domain. Each domain working group should involve at least 2 patient research partners (PRP) with personal experience of PsA and preferably with the domain under study. They will be involved in all steps of the instrument assessment process.
Initial literature search and appraisal of instruments for the domain under investigation.
Domain working group discussion of the rationale to include or exclude an instrument.
Delphi consensus exercise to determine the instrument(s) to include. Up to 2 rounds of Delphi exercise for instrument selection are recommended, with interim discussions following each on rationale among working group members. The group will pilot this instrument selection process for the physical function domain.
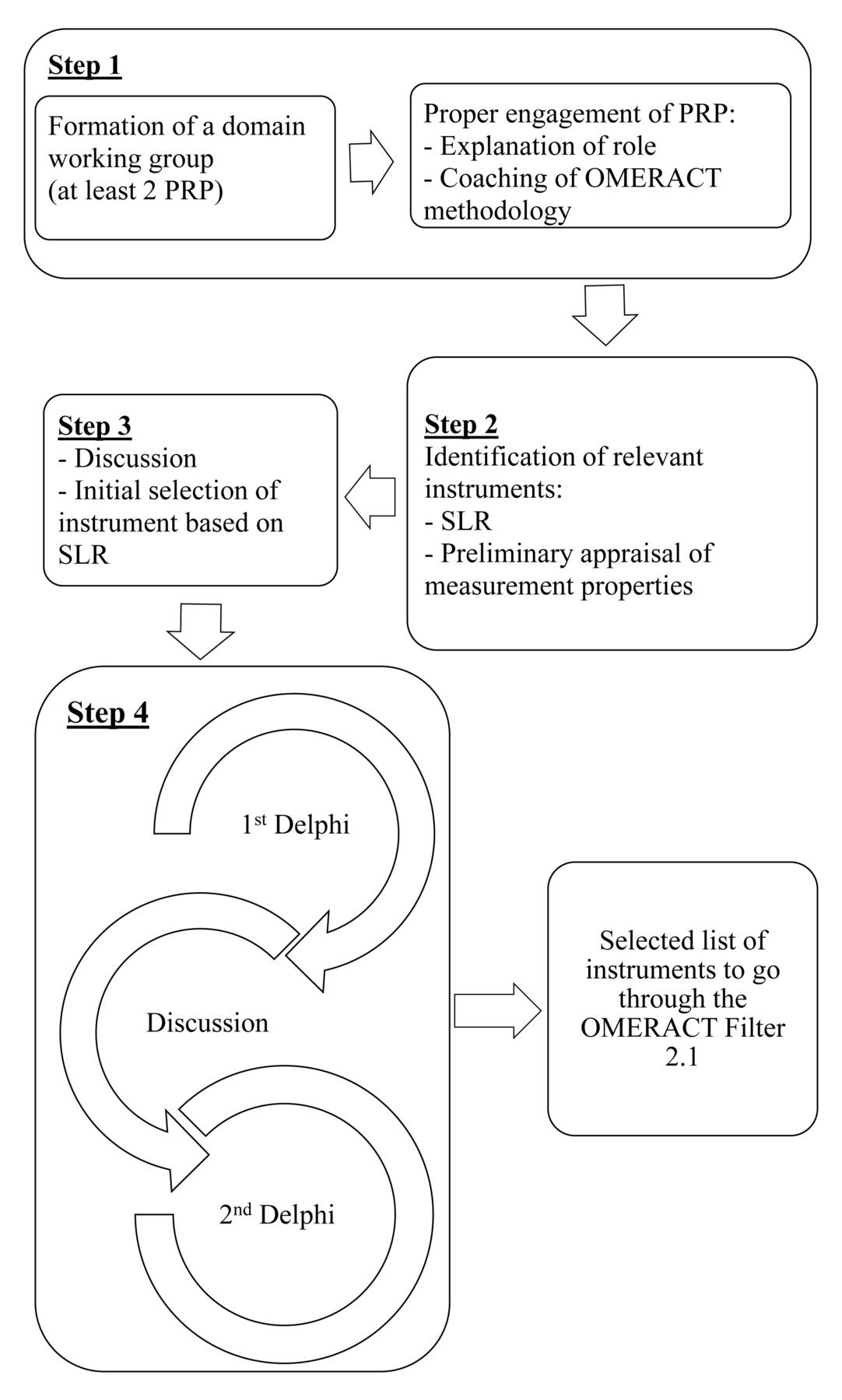
Proposed steps in preliminary instrument selection for PsA domains that are appropriate to further appraisal with OMERACT Filter 2.1. PSA: psoriatic arthritis; OMERACT: Outcome Measures in Rheumatology; PRP: patient research partners; SLR: systematic literature review.
Composite indices
Composite indices are commonly used in rheumatology for the combined assessment of disease activity and disease effect, as well as for defining a treatment target or disease state (e.g., remission). These indices typically span several domains to encompass a broader concept of disease activity including defining responders to treatment. Over the past decade, several composite indices have been developed specifically for PsA and used in RCT13. The composite indices commonly used for PsA are summarized in Table 1. Despite the extensive use of composite measures, the process for validation of these measures is not yet clear. A proposal has been made for a workstream within OMERACT to address this process. Members of the GRAPPA-OMERACT group will contribute to this process and develop consensus on how to validate these measures.
Commonly used composite outcome measures in clinical trials for psoriatic arthritis mapped onto corresponding domains.
DISCUSSION
It is the GRAPPA-OMERACT PsA Working Group’s objective to seek OMERACT’s endorsement of a full set of outcome measures that reflects the entire PsA Core Domain Set to facilitate comparison across clinical trials and collaboration between researchers in the PsA field. The working group has completed the process using the OMERACT Filter 2.1 to obtain OMERACT’s full or provisional endorsement of the first 2 instruments for the PsA Core Outcome Measurement Set. In addition, the working group has proposed a prioritized list of domains for instrument appraisal and a structure for the initial selection of instrument(s) for domains, while also highlighting the need for new guidelines to appraise composite indices.
Acknowledgments
The GRAPPA-OMERACT PsA Working Group acknowledges the support of GRAPPA, as well as Pam Love for her organizational efforts in supporting the working group’s meetings. The working group also acknowledges those working group members who were unable to attend the 2018 GRAPPA annual meeting. We acknowledge C.A. Lindsay (PharmD, Patient Research Partner employed by Amgen Inc.) who has contributed as a collaborator.
Footnotes
As part of the supplement series GRAPPA 2018, this report was reviewed internally and approved by the Guest Editors for integrity, accuracy, and consistency with scientific and ethical standards.
YYL is funded by the Clinician Scientist award of the National Medical Research Council, Singapore (NMRC/CSA-INV/0022/2017). AMO is funded by the Jerome L. Greene Foundation Scholar Award, the Staurulakis Family Discovery Award, the Rheumatology Research Foundation, and the US National Institutes of Health (NIH) through the Rheumatic Diseases Resource-based Core Center (P30-AR053503 Cores A and D, and P30-AR070254, Cores A and B). LCC is funded by a National Institute for Health Research Clinician Scientist award. The research was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC). AO is funded by the Rheumatology Research Foundation and NIH/National Institute of Arthritis and Musculoskeletal and Skin Diseases K23 AR063764 and R01 AR072363.








{kind=link}