

Abstract
Objective. To systematically review the evidence on treatment available to prevent an acute attack of gout when initiating a urate-lowering therapy (ULT) and for how long this treatment should be continued. To also evaluate the evidence on the optimal time to start a ULT after an acute attack of gout.
Methods. A systematic review as part of the 3e (Evidence, Expertise, Exchange) Initiative on Diagnosis and Management of Gout was performed using Medline, Embase, Cochrane Central Register of Controlled Trials (from 1950 to October 2011), and the European League Against Rheumatism (EULAR) and American College of Rheumatology (ACR) 2010/2011 meeting abstracts. Two reviewers independently screened titles and abstracts for selection criteria. Included articles were reviewed in detail, and a risk of bias assessment (using the Cochrane tool) was performed.
Results. The search identified 8168 articles and 197 abstracts, from which 4 randomized controlled trials were included in the review. Two of these studies compared placebo with colchicine, 1 compared differing durations of colchicine, and 1 compared colchicine with canakinumab.
Conclusion. Two randomized controlled trials have shown that colchicine prophylaxis for at least 6 months, when starting a ULT, reduces the risk of acute attacks. Canakinumab, although not currently licensed for gout, has been shown to provide prophylaxis superior to colchicine, when starting a ULT. There is no evidence on the optimum time to start a ULT after an acute gout attack.
This article is part of the 3e (Evidence, Expertise, Exchange) Initiative on Diagnosis and Management of Gout1. The objective of the current work was to systematically review the available literature concerning 1 of the 10 selected questions as an evidence base for generating the recommendations.
Acute gout attacks may be induced by the rapid reduction in serum uric acid that follows initiation or an increase in dose of urate-lowering drugs2. In clinical practice, treatments including nonsteroidal antiinflammatory drugs, colchicine, or corticosteroids are frequently coprescribed when urate-lowering therapies (ULT) are initiated, to reduce the likelihood of provoking attacks.
The above statements prompted 2 questions: (A) When introducing ULT, what is the best treatment to prevent an acute attack and for how long should it be continued? and (B) When is the optimum time to start ULT after an acute attack of gout?
MATERIALS AND METHODS
This systematic literature review (SLR) was performed according to the guidelines of the Cochrane Handbook for Systematic Literature Reviews3.
Rephrasing the research question
The initial questions were rephrased into epidemiological research questions according to the PICO (Population, Intervention, Comparison, Outcome) concept for the SLR suggested by the Cochrane Collaboration:
-
In patients with gout who are being started on a ULT, what is the most effective additional treatment to prevent an acute attack of gout, and for how long should this be continued?
-
When is the optimum time to start a ULT after an acute attack of gout?
In this context, for Question A, the population was defined as adults (age > 18 yrs) with gout who were starting a ULT. The interventions were nonsteroidal antiinflammatory drugs (NSAID), colchicine, steroids, cyclooxygenase II (COX-II) inhibitors, or interleukin 1 (IL-1) inhibitors while starting ULT (including allopurinol, febuxostat, pegloticase, rasburicase, probenecid, benzbromarone, or sulfinpyrazone). Interventions that had been withdrawn from use were excluded. The comparators were any of the intervention drugs, their combination, or a placebo. The primary outcomes were per OMERACT (Outcome Measures in Rheumatology)4: acute gout attacks, study participant withdrawal due to adverse effects, and serious adverse effects. Secondary outcomes included pain reduction, health-related quality of life (HRQOL), serum urate normalization, function (activity limitation), and tophus regression. Types of studies included SLR, randomized controlled trials (RCT), and clinical controlled trials (CCT).
For Question B, the population was defined as adults (age > 18 yrs) with gout who were starting a ULT after acute attack. The interventions were time and ULT (as above), and the comparator was time. The outcomes were identical to those in Question A. The types of studies included SLR, RCT, CCT, and cohort and case series > 20.
Systematic literature search
A comprehensive search strategy was generated for each question, aided by an experienced librarian. Where feasible, search terms were standardized. The complete search strategy can be viewed in an online appendix (available from www.3egout.com). Searches were conducted in Medline, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception to October 2011. Additionally, conference abstracts presented at 2010 and 2011 American College of Rheumatology (ACR) and European League Against Rheumatism (EULAR) scientific meetings were hand-searched and reviewed.
Selection of articles
Two reviewers (RS and AK) independently screened each title and abstract retrieved by the searches and selected studies for full-text review according to predetermined criteria as detailed above. Included articles were restricted to those published in 1 of the predefined languages including Dutch, English, French, German, Portuguese, or Spanish. Articles that did not fulfill the inclusion criteria or had insufficient data for analysis were excluded; all reasons for exclusion were documented.
Data extraction and assessment of risk of bias
For all included studies, the following data were extracted onto standardized forms: study design, characteristics of study population, intervention and comparator regimen, and duration and outcome including adverse events. The raw data (means and standard deviations for continuous outcomes and number of events for dichotomous outcomes) were extracted for outcomes of interest. To assess risk of bias within the trials identified, the Cochrane Risk of Bias assessment tool for intervention studies was used5.
RESULTS
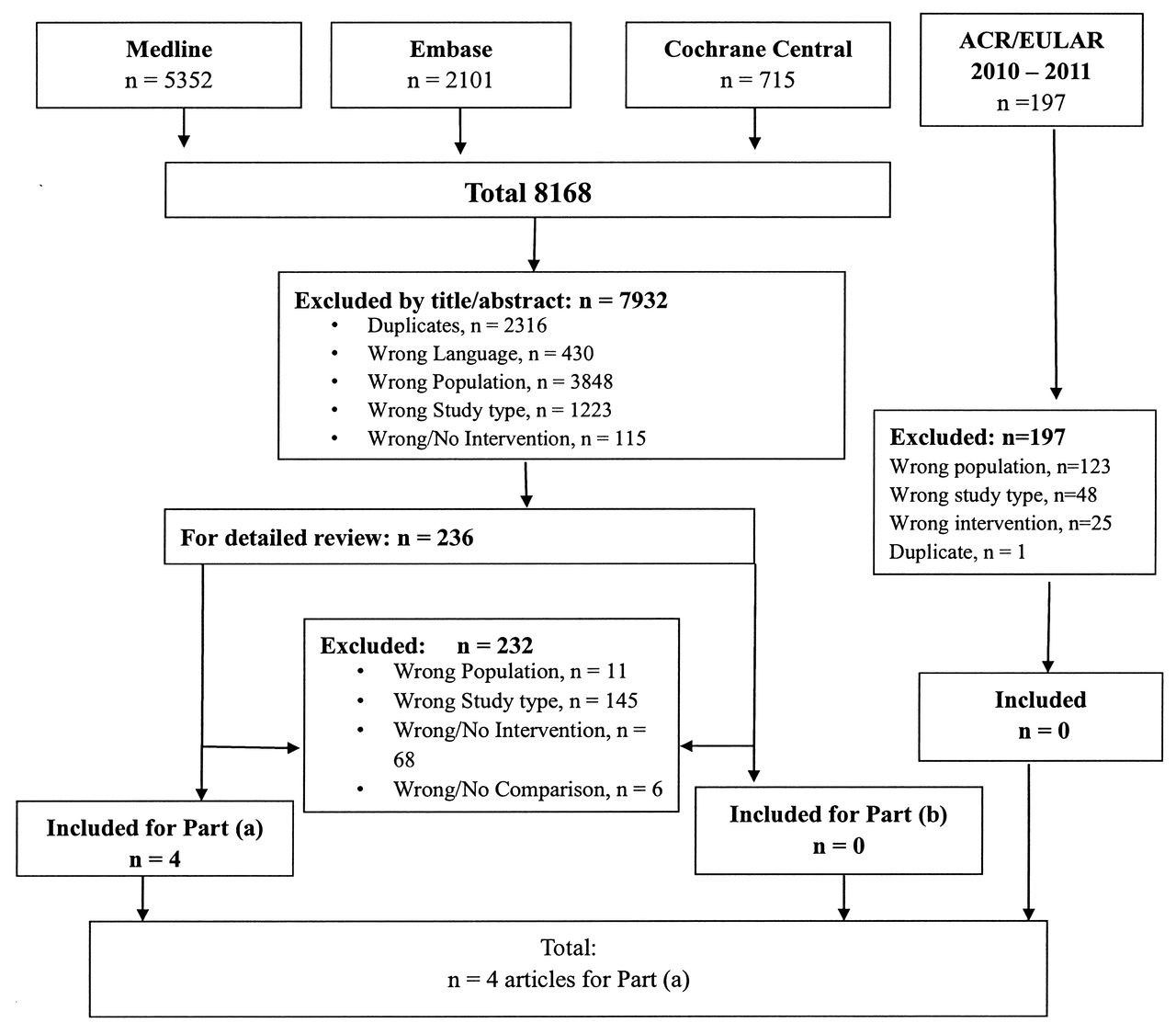
The search strategy identified 8168 articles from Medline, Embase, Cochrane CENTRAL, and 197 abstracts submitted for the EULAR (n = 89) and ACR (n = 108) 2010/2011 meetings. From these, 236 full articles were reviewed in detail, and 4 RCT were identified as fulfilling inclusion criteria for Question A addressing flare prophylaxis when initiating ULT. No studies were identified as fulfilling the inclusion criteria for Question B, suggesting no evidence is available on the optimum timepoint at which to start ULT after an acute attack of gout.
The date of the search was April 10, 2011, for all 3 databases. There was 1 relevant abstract from ACR 2010, which was a duplicate of a report published in 2011 and had already been included for review. Figure 1 illustrates the process from the initial search to final inclusion.

Process from the initial search to the final inclusion.
Excluded studies
The main reason for exclusion of studies after detailed review was that they did not include patients with gout who were starting a ULT. Three articles were excluded because they concerned the drug azapropazone, which has been withdrawn from use6,7,8.
Included studies
Four studies identified to address flare prevention prophylaxis when initiating ULT are summarized in Table 1. Of these 4 studies, 2 compared placebo with colchicine, 1 compared differing durations of colchicine, and 1 compared colchicine with canakinumab.
Summary of the 4 included studies.
In 2 RCT9,10 use of colchicine (daily dose 0.6–1.5 mg) for the initial 3–6 months after starting ULT (allopurinol or probenecid) resulted in a reduction in the number of patients that developed acute gout attacks and a reduction in the severity of these flares compared to placebo.
Borstad, et al9 studied 43 people starting treatment with allopurinol for chronic gout, and found that acute gout flares occurred in 77% (17/22) of placebo subjects and 33% (7/21) of colchicine subjects (p = 0.008). Multiple gout flares occurred in 14% of the colchicine group and 63% of placebo subjects (p = 0.004). The number needed to treat (NNT) was 2 (95% CI 1–6), suggesting that colchicine would prevent 1 in 2 patients from experiencing an attack. The severity of gout flares measured by visual analog scale averaged 3.64/10 in the colchicine group and 5.08/10 in the placebo group (p = 0.018). The average length of gout flares did not vary significantly between the groups (6 days for colchicine and 5.56 days for placebo; p = 0.566). There were 7 withdrawals, 3 in the colchicine group and 4 in the placebo group. The colchicine group contained 1 subject who developed a stroke at 3 months, 1 subject who discontinued the drug due to subjective muscle weakness at 2.5 months, and 1 subject who was lost to followup after being treated for 3 months. The placebo group contained 2 subjects who withdrew due to a high frequency of flares (at 2 and 3 months), 1 subject withdrew due to inadvertent medication discontinuation after 3 months, and 1 subject withdrew because frequent travel prevented adequate followup after 4 months. The number needed to harm (NNH) is 26 for withdrawals: i.e., 26 patients need to be treated with colchicine before 1 additional withdrawal occurs compared to placebo, and the relative risk (RR) of withdrawals is 0.8 (95% CI 0.15–3.84). Adverse effects were seen in 36% of the placebo group and 43% of the colchicine group (p = 0.760). The NNH is 15. Diarrhea as a side effect was seen in 4.5% of the placebo group and 38% of the colchicine group (p = 0.009). The NNH is 3 and RR 8.38 (95% CI 1.25–178). Despite an increase in diarrhea in this study, overall adverse effects and withdrawals were similar between colchicine and placebo groups.
Paulus, et al10 performed a comparison trial of 52 patients with intercritical gout who were randomly allocated to probenecid 500 mg 3 times daily plus colchicine 0.5 mg daily or to probenecid 500 mg 3 times daily plus placebo daily for 6 months. They found that the number of acute attacks of gouty arthritis per patient per month in the colchicine-probenecid group was 0.19 (0.05) and in the placebo-probenecid group it was 0.48 (0.12) (p < 0.05). Therefore, there were significantly fewer acute attacks of gout in the colchicine-treated group. Both groups in this study had similar safety profiles. Side effects were reported by 75% (15/20) of subjects taking colchicine and 44% (8/18) taking placebo-probenecid, with a RR 1.69 (95% CI 0.91–3.03) and NNH of 3 (1.6–α) and with diarrhea as side effect, RR 1.35 (95% CI 0.54–3.62) and NNH of 9 (2.3–α).
Karimzadeh, et al11 investigated 190 patients with gout who were all given allopurinol and randomly divided into groups 1, 2, and 3 to receive colchicine for 3 to 6 months, 7 to 9 months, and 10 to 12 months, respectively; patients were then followed for 1 year for recurrence of gouty attacks. For detecting the probability of recurrence of acute arthritis, they used survival analysis and Kaplan-Meier method (from SPSS Version 11.5). Survival curves of the 3 groups were compared with log-rank test. At the end of 6 months, the percentage of acute flare at 6 months (probability of recurrence of occurred attack) in group 1: 46%; group 2: 11%; and group 3: 6%. At the end of 1 year, the percentage of acute flare was 54%, 27.5%, and 23% in group 1, 2, and 3, respectively. Log-rank test showed significant differences between group 1 and the others (p < 0.001), and no difference between groups 2 and 3 (p = 0.1). The mean time of recurrence was 8 months in group 1 and 11 months in groups 2 and 3. Log-rank test showed a significant difference between group 1 and the others (p < 0.001) and no difference between groups 2 and 3 (p = 0.09). They concluded that the most suitable duration of colchicine prophylaxis accompanied with lower recurrence rate was 7–9 months, which seemed more cost-effective than a 10–12 month regimen. This study, however, was at high risk of bias.
Schlesinger, et al12 performed a double-blind, double-dummy, dose-ranging study with 432 patients with gout initiating allopurinol treatment; patients were randomized 1:1:1:1:1:1:2 to receive a single dose of canakinumab 25, 50, 100, 200, or 300 mg subcutaneously (SC); 4 × 4 weekly doses of canakinumab (50 + 50 + 25 + 25 mg SC; or, more precisely: 50 mg on day 1 and at week 4, and 25 mg at week 8 and week 12); or daily colchicine 0.5 mg for 16 weeks. The study aimed to determine the canakinumab dose having equivalent efficacy to colchicine 0.5 mg at 16 weeks. The estimated canakinumab dose with equivalent efficacy to colchicine was below the range of the doses tested. At 16 weeks, there was a 62%–72% reduction in the mean number of flares per patient for canakinumab doses > 50 mg versus colchicine, and the percentage of patients experiencing > 1 flare was significantly lower for all canakinumab doses (15%–27%) versus colchicine (44%; p < 0.05). The incidence of adverse effects was similar across treatment groups. They concluded that single doses of canakinumab ≥ 50 mg or four 4-weekly doses provided superior prophylaxis against flares compared with daily colchicine 0.5 mg.
No evidence for the use of COX-II inhibitors or glucocorticoids as prophylaxis when initiating ULT was retrieved. Three studies6,7,8 were retrieved on use of azapropazone, NSAID with uricosuric properties, as prophylaxis when initiating ULT, but were excluded from this review because the drug has been withdrawn.
No evidence was retrieved on the optimum time to start ULT after an acute attack of gout.
DISCUSSION
Acute gout attacks may occur as a consequence of the initiation of ULT and effective reduction of serum uric acid (SUA) concentrations13. Indeed, the more rapid and greater the reduction in SUA, the more likely it is that a flare will occur2,14. To help prevent flares, it has been recommended that initiation of ULT be accompanied by low-dose colchicine or NSAID15,16,17.
EULAR guidelines15 recommend the use of colchicine 0.5 to 1 mg per day (evidence level 1b: RCT) or an NSAID (evidence level 2a: non-RCT) during the first months of urate-lowering therapy for prophylaxis against acute attack. These guidelines do not commit to a specific duration of prophylaxis; rather they state that based on limited data, the duration of prophylaxis must be determined by balancing the risk of acute attack against the potential risk for toxicity. For patients receiving NSAID, gastroprotection is recommended when indicated.
The British Society for Rheumatology/British Health Professionals in Rheumatology guidelines16 recommend colchicine 0.5 mg twice daily for up to 6 months upon initiation of ULT (evidence grade A: metaanalysis or RCT). The NSAID, including COX-II–selective agents, are reserved for patients who cannot tolerate colchicine, and their use is limited to ≤ 6 weeks (evidence grade C: expert reports and opinions).
This SLR has identified 3 RCT, of which 2 were double-blinded and support the use of colchicine 0.6–1.5 mg daily as flare prophylaxis when starting ULT for up to 6 months. Both double-blind RCT9,10 showed that patients starting ULT on colchicine had significantly fewer attacks of gout than those in the placebo group. Despite an increase in diarrhea in 1 study9, overall adverse effects and withdrawals were similar between colchicine and placebo groups. Limitations of these 2 studies were their small sample size, and although 1 was at low risk of bias9, the other was at high risk of bias10, as per the Cochrane tool for risk of bias assessment5.
The third RCT11 studied differing durations of colchicine prophylaxis on initiating allopurinol and found that colchicine prophylaxis given for 10–12 months was associated with the least risk of reccurrence of gout attack. However, there was no placebo group and this study was assessed as being at high risk of bias5.
In clinical practice, oral NSAID are often used for flare prophylaxis when initiating ULT. Although 2 controlled trials6,7 were identified comparing azapropazone (NSAID with uricosuric effects) 600 mg twice daily with allopurinol, 1 trial7 was part of the other multicenter study6. Further, they were excluded from this review because the drug has been withdrawn and there was no comparator NSAID. However Zhang, et al15 refer to the study by Templeton6 and so it is worth mentioning that overall they investigated 156 patients, and while both treatments showed similar reductions in SUA [effect size = 0.00 (95% CI −0.26 to 0.26)], azapropazone showed additional prophylactic benefit against acute attacks. The NNT was 7 (4 to 17), so treating every 7 patients with azapropazone would prevent 1 more patient from suffering an acute attack than would be the case if allopurinol was used alone. However, this was offset by a higher incidence of gastrointestinal upset in the azapropazone group.
A controlled trial by Fraser, et al8 was also excluded from the review because it compared azapropazone with indomethacin in patients with gout who were then started on allopurinol; again, this was because azapropazone has been withdrawn from use.
Another notable exclusion from this SLR was the post-hoc reanalysis of data on gout flares from 3 randomized, placebo-controlled, Phase III trials, in which patients with gout received ULT (febuxostat or allopurinol) or placebo for 6 months or 1 year and flare prophylaxis with colchicine 0.6 mg od or naproxen 250 mg bd for 8 weeks or 6 months18. The prophylactic regimen was chosen at the discretion of the investigator, based on renal function and known intolerance to either drug. Although these trials were not designed to assess different prophylactic regimens in a blinded, controlled manner, they were the largest trials of ULT to examine the effects of both colchicine and NSAID naproxen on flare rates over different durations of prophylaxis, and concluded that flare prophylaxis for up to 6 months during the initiation of ULT appeared to provide greater benefit than flare prophylaxis for 8 weeks, with no increase in adverse effects. However, this study was excluded, as it did not fulfill the strict inclusion criteria for this review.
In conclusion, 2 RCT support the use of low-dose colchicine for prophylaxis for at least 6 months to prevent acute attacks when initiating ULT, whereas evidence for licensed NSAID for the same purpose is not available. Both treatments have potentially serious side effects, so their risks and benefits need to be carefully weighed prior to their use in clinical practice. In addition, newer treatments such as canakinumab, although not currently licensed for gout, have been shown to provide superior prophylaxis to colchicine, when starting a ULT. However, data on this subject are still limited, and further prospective RCT are needed to evaluate flare prophylaxis for up to 6 months, after 6 months, and over time. There is no currently available evidence on the optimum time to start ULT after an acute attack, and further research into this area would also be useful to guide clinical practice.
Footnotes
-
The authors acknowledge the work of all members of the 3e scientific committees and all participants in the national meetings. This article is derived from the 3e Gout program, which was sponsored by AbbVie Inc. Margaux Orange, Paris, France, provided logistical and administrative support for the 3e Gout meetings; this work was funded by AbbVie Inc. AbbVie employees were present during the 3e meetings, but did not influence the scientific discussions. AbbVie did not review the content or have influence on this manuscript.








{kind=link}