

Abstract
Ultrasound (US) is a rapidly evolving technique that is gaining increasing success in the assessment of psoriatic arthritis (PsA). It permits early detection and careful characterization of the inflammatory process at different tissues, which is important in diagnostic and therapeutic procedures. US presents several advantages over other imaging techniques: it is patient-friendly, safe, noninvasive, free of ionizing radiation, less expensive, and permits multiple target assessment in real time without the need for external referral. The aim of this report was to analyze the potential role of US in the assessment and management of PsA and to discuss the current evidence supporting its application in daily clinical practice.
Psoriatic arthritis (PsA) is a chronic inflammatory disease with a widely variable intraindividual and interindividual clinical course and outcome that may develop in 5–40% of patients with psoriasis1. Its heterogeneity is such that the term “psoriatic disease” has recently been suggested to encompass the involvement at different tissue levels, including joint, tendon, enthesis, skin, and nails2,3.
Early detection and careful characterization of the inflammatory process play key roles in both diagnostic and therapeutic procedures.
Management strategies and pharmacological treatments in PsA have substantially changed over the last few years. The quality of life of patients greatly improved after the introduction of tumor necrosis factor-α (TNF-α) antagonists4,5.
Ultrasound (US) is a sensitive imaging technique for the assessment of anatomical changes, disease activity, and therapy efficacy in patients with rheumatoid arthritis (RA) and PsA6,7,8,9,10,11,12,13,14,15,16,17. It has, in particular, a great potential with respect to other imaging techniques in the early detection of aggressive arthritis and surveillance of disease activity. Moreover, US is patient-friendly, safe, noninvasive, free of ionizing radiation, and less expensive, and it allows multiple target assessment in real time without the need for external referral.
Here we analyze the potential role of US in the assessment and management of PsA and discuss the current evidence supporting its application in daily clinical practice.
JOINT INVOLVEMENT
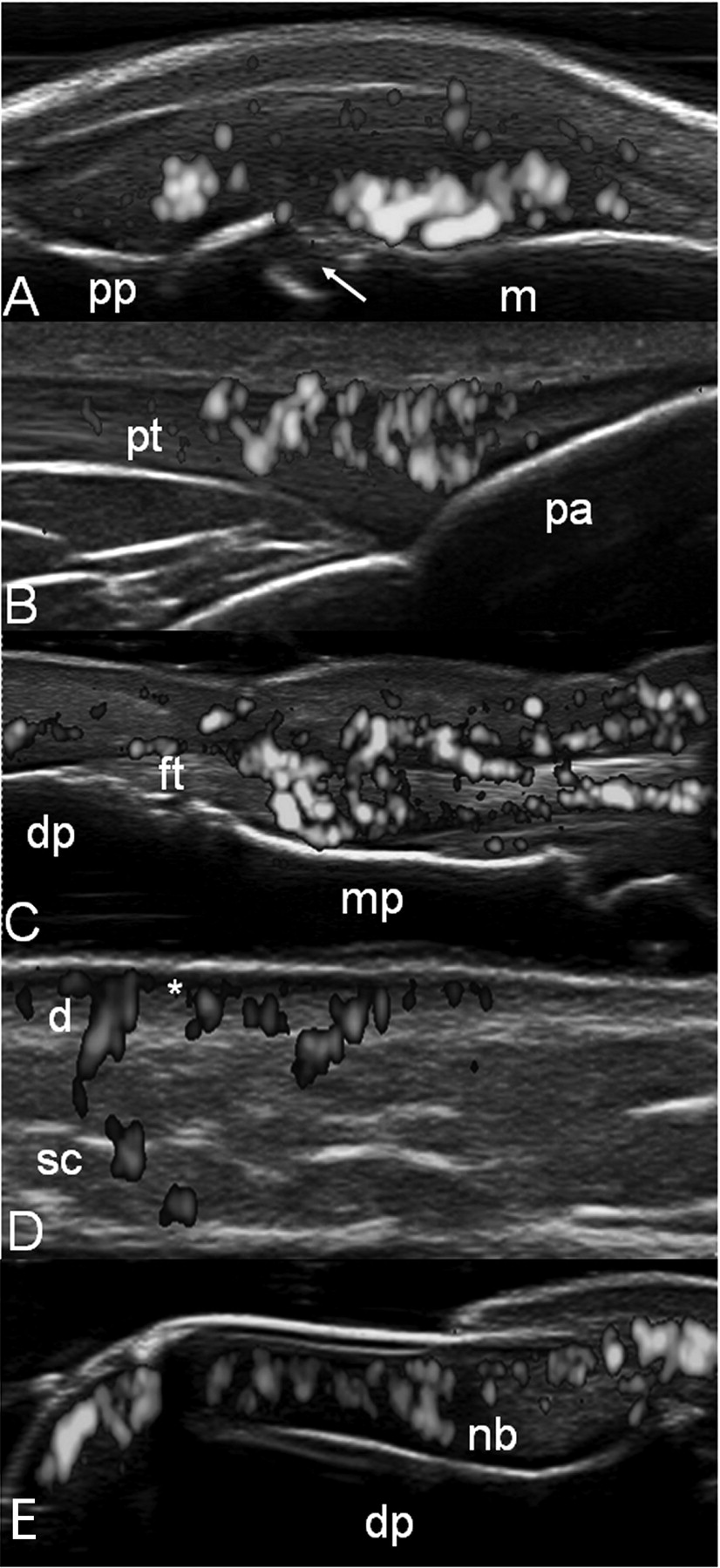
An accurate assessment of synovitis, enthesitis, and tenosynovitis plays a key role for the management of PsA (Figures 1A–C). The US definitions for nomenclature and methodological approaches were published by the Outcome Measures in Rheumatology Clinical Trials US group18 (Table 1).

A. Metacarpophalangeal joint on dorsal longitudinal scan. Active synovitis. Note both the marked synovial proliferation and the intense hyperemia, detected by power Doppler, and the bone erosion in the neck of the metacarpal bone (arrow). B. Distal patellar enthesis on longitudinal scan. Hypoechogenicity (due to intratendinous edema) indicates an increase of the thickness of the enthesis. Note the intense intraentheseal power Doppler signal. C. Flexor tendons of second finger on volar longitudinal scan showing a tendon sheath widening with signs of synovial proliferation and presence of intense power Doppler signal inside and surrounding the tendon. D. Psoriatic plaque. Note that the dermal layer at psoriatic lesion appears thickened and nonhomogeneous (d), compared to the contiguous normal skin. Moreover, a focal hypoechoic band at the dermis level (*) is visible, with evident power Doppler signal. E. Nail. Longitudinal scan. Presence of power Doppler signal indicative of an increase of blood flow at the nail bed (nb) level. m: metacarpal bone; pp: proximal phalanx; et: extensor digitorum tendon; pt: patellar tendon; pa: patella; dp: distal phalanx; mp: middle phalanx; ft: flexor tendon; d: dermis, sc: subcutaneous fat; nb: nail bed.
Outcome Measures in Rheumatology Clinical Trials definitions for ultrasound findings.
Weiner, et al7 demonstrated a good diagnostic sensitivity of US in the detection of synovitis of hands and feet in a small cohort of patients. Similar results were found by Wiell, et al,8 who concluded that US was more sensitive than radiography and clinical examination in the assessment of inflammatory changes, particularly synovitis. That study also provides encouraging data about the interobserver reliability for the inflammatory and anatomic changes detectable by US.
Comparison studies between US and other imaging techniques, such as magnetic resonance imaging (MRI), radiography, and scintigraphy have also been conducted, confirming the validity of US for detection of synovial inflammation in PsA7,8.
Bone erosions are the hallmark of joint damage in PsA and both their early detection and increase in number or size over time are indicative of a poorer outcome19.
In daily clinical practice, conventional radiography is the standard imaging technique for detecting and scoring joint damage, in spite of its low sensitivity compared to computed tomography (CT), MRI, and US.
The feasibility and construct validity of US in visualizing bone erosions has been demonstrated mainly in patients with RA since the early 1990s20. The criterion validity of US has been investigated in a limited number of studies of PsA using MRI and scintigraphy as gold standards7,8. Conversely, there is little evidence about discriminant validity of US in patients with PsA.
In a study including 15 patients with PsA, Wiell, et al8 reported that both US and MRI were more sensitive than clinical assessment and radiography for visualization of inflammatory and destructive changes in fingers and toes of patients with PsA. Moreover, they showed a high US interobserver agreement for bone erosions. It is noteworthy that in the cohort-case study conducted by Weiner, et al7, US detected more erosions than MRI. The main limitation of that study was that radiography was used as a gold standard for the erosions.
ENTHESIS AND TENDON INVOLVEMENT
US has demonstrated its ability to detect enthesitis more accurately than clinical examination in patients with PsA. Frediani, et al21, in a study including 40 patients with PsA and 40 patients with RA, showed a quadricipital enthesitis in 45% of patients with PsA and none in RA. They also reported isolated quadricipital enthesitis without knee effusion in only 16% of patients with PsA, whereas knee effusions were found more commonly in patients with RA22. Similar results were found by Delle Sedie, et al, who demonstrated a prevalence of knee enthesitis of 39.7% in a cross-sectional study of 83 patients with PsA10.
Scarpa, et al23, examined 47 patients with early PsA. All patients underwent clinical evaluation, bone scintigraphy, and US assessment. US was able to reveal signs of enthesitis in all the areas of increased radionuclide uptake on scintigraphy.
Studies have reported entheseal involvement in asymptomatic patients with psoriasis showing a high prevalence of subclinical enthesopathy24,25. Although this is an interesting field of research, the ability of US to detect enthesitis in patients with psoriasis should be the object of longitudinal investigations to define its value in revealing subclinical PsA.
US is an invaluable imaging method for the assessment of tendons with synovial sheath. Its role has been demonstrated especially in patients with RA. Its potential in patients with PsA awaits adequate investigation.
Fournié, et al26, conducted a single-center study comparing pulsed Doppler (PD) US findings in 25 fingers with RA and 25 fingers with PsA. Tenosynovitis was seen in both groups without significant statistical difference. Of interest is that extrasynovial changes (soft tissue inflammation or thickening and enthesitis) were found in 21/24 fingers with PsA (84%), compared to none in the fingers with RA. In another open-label study aimed at detecting tendon abnormalities at hand and wrist level in patients with PsA, Milosavljevic, et al27 demonstrated that US was more sensitive than clinical examination in detecting tendon pathology, particularly tenosynovitis. They found tendon involvement in 22 of 36 patients (61%).
There are a few data about the tendons without synovial sheath involvement in PsA28,29. The inflammatory changes detectable by US include tendon thickening and hypoechogenicity due to tendon edema, with or without intratendinous PD signal.
SKIN AND NAIL INVOLVEMENT
The recent availability of US equipment with PD frequency higher than 10 MHz also enables a very sensitive visualization of blood flow at the dermal level.
Preliminary results have been published demonstrating the potential role of PDUS in the assessment of psoriatic plaque and onychopathy in patients with psoriasis and/or PsA11,30,31,32 (Figures 1D–E). The PD criterion validity and responsiveness to change have been demonstrated by a positive correlation with the histology findings at psoriatic plaque level in patients receiving TNF-α antagonist therapy30. Further investigations regarding both intraobserver and interobserver reproducibility and studying larger series are still needed to confirm these preliminary results.
DIFFERENTIAL DIAGNOSIS
Although US has been demonstrated to be useful in the early assessment of joints and soft tissue inflammation in patients with chronic arthritis, there is a lack of evidence supporting its role in the differential diagnosis. Only 1 study conducted by our group33 demonstrated a potential role of US in the differential diagnosis between RA and PsA at metacarpophalangeal (MCP) joint level (Figure 2). Eighty patients with RA and 20 patients with PsA were studied, assessing the following measures: presence of joint cavity widening as a result of synovial fluid and/or synovial hypertrophy, hypoechoic swelling surrounding the extensor digitorum tendon, and intraarticular or peritendinous PD signal. The peritendinous extensor tendon inflammation (PTI pattern) was highly specific of PsA because it was present in 65.8% of MCP joints as the only US sign of inflammation, whereas no US signs of PTI pattern were found in patients with RA33. It is interesting to note that the PTI pattern was frequently observed in patients with shorter disease duration (mean 13.2 months; SD 3.67).

Psoriatic arthritis. Metacarpophalangeal joint on dorsal longitudinal scan (A) and transverse scan (B), showing the peritendinous extensor tendon inflammation pattern. The ultrasound findings are characterized by a hypoechoic swelling surrounding the extensor digitorum tendon (*) associated with subcutaneous edema and power Doppler signal surrounding the extensor digitorum tendon (et). m: metacarpal bone.
US-GUIDED PROCEDURES
US-guided needle placement within the target area is an accurate and safe approach for patients with PsA who require aspiration of synovial fluid or injection therapy. Under US guidance it is possible to visualize the progression of the needle in the soft tissues toward the target area, avoiding tissue damage. Moreover, US-guided injections for PsA are significantly less painful than palpation-guided models.
THERAPY MONITORING
As mentioned, the introduction of biological drugs has dramatically modified the clinical approach of patients with PsA. US offers some advantages with respect to other imaging techniques, such as conventional radiography or CT, in therapy monitoring because it can reflect both morphostructural changes and inflammatory activity.
To date, the role of US in therapy monitoring of PsA is not adequately defined. Fiocco, et al16 demonstrated the potential role of US in evaluating the response to therapy of persistent knee joint synovitis by a 12-month longitudinal study in prearthroscopic and postarthroscopic synovectomy in patients with RA and PsA. In another 12-month open-label single-center study, Fiocco, et al17 followed up 27 knees in a small cohort of 20 patients (12 with RA and 8 with PsA) receiving TNF-α antagonist therapy. US showed a reduction of synovial membrane thickness (grayscale) and intraarticular blood flow (PD signal) over time.
Aydin, et al34, in a study that included 43 patients with spondyloarthritis, found a significant decrease in blood flow at the Achilles enthesis level after 2 months of TNF-α antagonist therapy. Naredo, et al35, in a large study involving 35 centers, demonstrated that US including PD assessment can be used as a valuable tool to assess enthesis response to therapy in spondyloarthritis. That was the first study that separately evaluated response to therapy of different US abnormalities at multiple entheseal sites, demonstrating a highly significant improvement of both grayscale abnormalities (hypoechogenicity and/or thickening) and PD signal. A significant improvement of adjacent bursitis has also been observed. Conversely, entheseal cortical abnormalities (bone erosion and/or enthesophytes) and calcifications did not improve throughout the followup period, in spite of therapy.
Recently, our group30 demonstrated the sensitivity to change of PDUS assessments of psoriatic plaque over an 8-week period in a cohort of patients with psoriasis and PsA who were receiving TNF-α antagonist therapy.
To date, the few data available in literature testing the sensitivity to change of PDUS in PsA have depicted its potential at assessing only a single domain (i.e., joint, enthesis, tendon, or skin). We have recently proposed36 a preliminary PDUS composite score for the global assessment of blood flow changes after treatment in patients with PsA. The PDUS composite score was called “Five Targets Power Doppler for Psoriatic Disease (5TPD)”, which combines the assessment of joint, tendon with synovial sheath, enthesis, skin, and nail. PD for each target was graded from 0 to 3 on the basis of the semiquantitative scoring systems previously suggested. The maximum total score of 5TPD is 15. Our preliminary results showed a significant improvement of global 5TPD scores from baseline to 8 weeks after anti TNF-α treatment. Moreover, the interobserver and intraobserver κ values varied from good to excellent at baseline and followup, and the time spent on baseline US examinations was mean 10.5 ± SD 2.0 min, and no more than 7 min for followup assessment. The preliminary results may indicate that the 5TPD is a feasible, reliable, and comprehensive approach for multitarget treatment monitoring of PsA.
The currently available data demonstrate that the standard clinical approach could result in reduced sensitivity in the assessment of patients with PsA. The data also demonstrate that US can be regarded as a feasible and effective imaging technique that can allow early recognition of anatomical changes, careful guidance for aspiration and/or local treatment, and short-term therapy monitoring at joint, tendon, enthesis, nail, and skin levels.








{kind=link}
{kind=link}