

Abstract
The goal of treatment for patients with rheumatoid arthritis (RA) is to achieve remission, or at least a low disease activity state. A variety of useful and practical tools are available to rheumatologists to assess patient prognosis and evaluate response to treatment in clinical practice. Frequent assessments, ideally every 1 to 3 months, allow rheumatologists to adjust therapy according to patient outcomes. For patients who fail to respond to treatment with classic disease modifying antirheumatic drugs, combination therapies with biologic agents offer improved outcomes.
- ANTI-TUMOR NECROSIS FACTOR AGENTS
- BIOLOGIC THERAPIES
- DISEASE ACTIVITY SCORE
- RHEUMATOID ARTHRITIS
- CLINICAL DISEASE ACTIVITY INDEX
- SIMPLIFIED DISEASE ACTIVITY INDEX
For patients with rheumatoid arthritis (RA), the goal of therapy is to achieve a significant clinical response. However, depending on the patient and on the treating physician, the definition of significant clinical response can vary widely – from low disease activity to clinical remission. Even among patients with established disease, optimal treatment can lead to clinical remission.
INSTRUMENTS RECOMMENDED FOR ASSESSMENT OF RA IN DAILY CLINICAL PRACTICE
In addition to clinical response, a goal of RA therapy is radiographic remission; that is, in some patients structural damage may progress despite good clinical response. The most accepted clinical assessment tools are the American College of Rheumatology (ACR) response criteria1 and the European League Against Rheumatism (EULAR) response criteria2, as well as the Disease Activity Score (DAS)3 and its simplifications such as the Simplified Disease Activity Index (SDAI)4 and the Clinical Disease Activity Index (CDAI)5. Correlations at the group level have been demonstrated among the different measures; however, discrepancies may exist at the individual level. Using data pooled from several clinical trials of RA, Aletaha and colleagues compared the value of reporting treatment effects in RA by relative change from baseline (i.e., ACR response status) or by absolute disease activity state (DAS; i.e., remission)6. Among patients who had completed one year of treatment, 6% of those who achieved an ACR 70% response (ACR70) still had moderate disease activity and were progressing radiographically. Among those who achieved an ACR50 response, which is still considered to be a significant clinical response, 30% had moderate disease activity.
ACR response criteria, while valuable for comparing the efficacy of various RA therapies, do not provide a reliable assessment of disease activity in daily clinical practice. For this purpose, composite measures allow the various aspects of disease to be integrated into a single numerical value. The ACR currently recommends the DAS287, the SDAI, the CDAI, and the Rheumatoid Arthritis Disease Activity Index (RADAI)8, as well as some patient-driven tools such as the Patient Activity Scale (PAS) I or II and the Routine Assessment Patient Index Data (RAPID)9.
The DAS28 is a widely used indicator of disease activity and response to treatment in patients with RA. However, there are some obstacles to its use in daily practice. Calculation of the DAS28 requires a complicated formula that necessitates the use of a special calculator (Table 1)4. More weighting is also placed on the tender joint count than on the swollen joint count, despite some recent evidence to suggest that swollen joint count is better correlated with radiographic evidence10.
Elements of composite indices for evaluation of disease activity in rheumatoid arthritis4. Values in parentheses are ranges.
The search for a simplified measure led to the development of the SDAI, which eliminates the weighting of variables and utilizes a simple numeric calculation. The SDAI includes tender and swollen joint counts, as well as the patient’s and the physician’s assessment of disease activity and C-reactive protein (CRP) levels. The SDAI has been validated for the assessment of patients with RA in trials of leflunomide, where it showed good correlation with DAS28 and ACR responses11. A limitation of the SDAI is that the patient’s CRP values need to be available at the time of the assessment. In cases where this information is not readily available, the CDAI may be a valuable assessment tool. The CDAI has been validated against the SDAI4. Although developed primarily for use in clinical practice, the SDAI and CDAI have begun to be used as secondary outcome measures in clinical trials. Thresholds of different levels of disease activity and remission have been proposed.
To evaluate the usefulness of these instruments in daily clinical practice, Mierau and colleagues analyzed remission and sustained remission at 2 consecutive visits in 621 patients12. Remission was observed at either of the 2 visits in 33.5% of patients according to SDAI or CDAI criteria, 42.7% according to DAS28 criteria, and 38.6% according to modified ACR criteria (p < 0.01). Sustained remission ranged from 16.7% with the SDAI to 19.6% with the DAS28. Their study showed that the SDAI and CDAI criteria, which allow for less residual disease activity, appear to be more stringent than the DAS28 and ACR criteria. That sustained remission was achievable in clinical practice, even according to these stringent criteria, was an encouraging result of this study.
RECOMMENDATIONS FOR THE MANAGEMENT OF EARLY RA
With the development of new effective treatments and sensitive outcome measures for RA, a number of associations have developed recommendations for the management of patients with early RA. Highlights of the EULAR recommendations include early referral, ideally within 6 weeks of the onset of symptoms, and early initiation of disease modifying antirheumatic drugs (DMARD); methotrexate (MTX) is preferred first-line for patients at risk of persistent or erosive arthritis, regardless of whether they fulfil the criteria for inflammatory rheumatological disease13. They also introduced the concept of remission as a goal, recommending regular assessments in 1 to 3 month intervals until this goal is achieved.
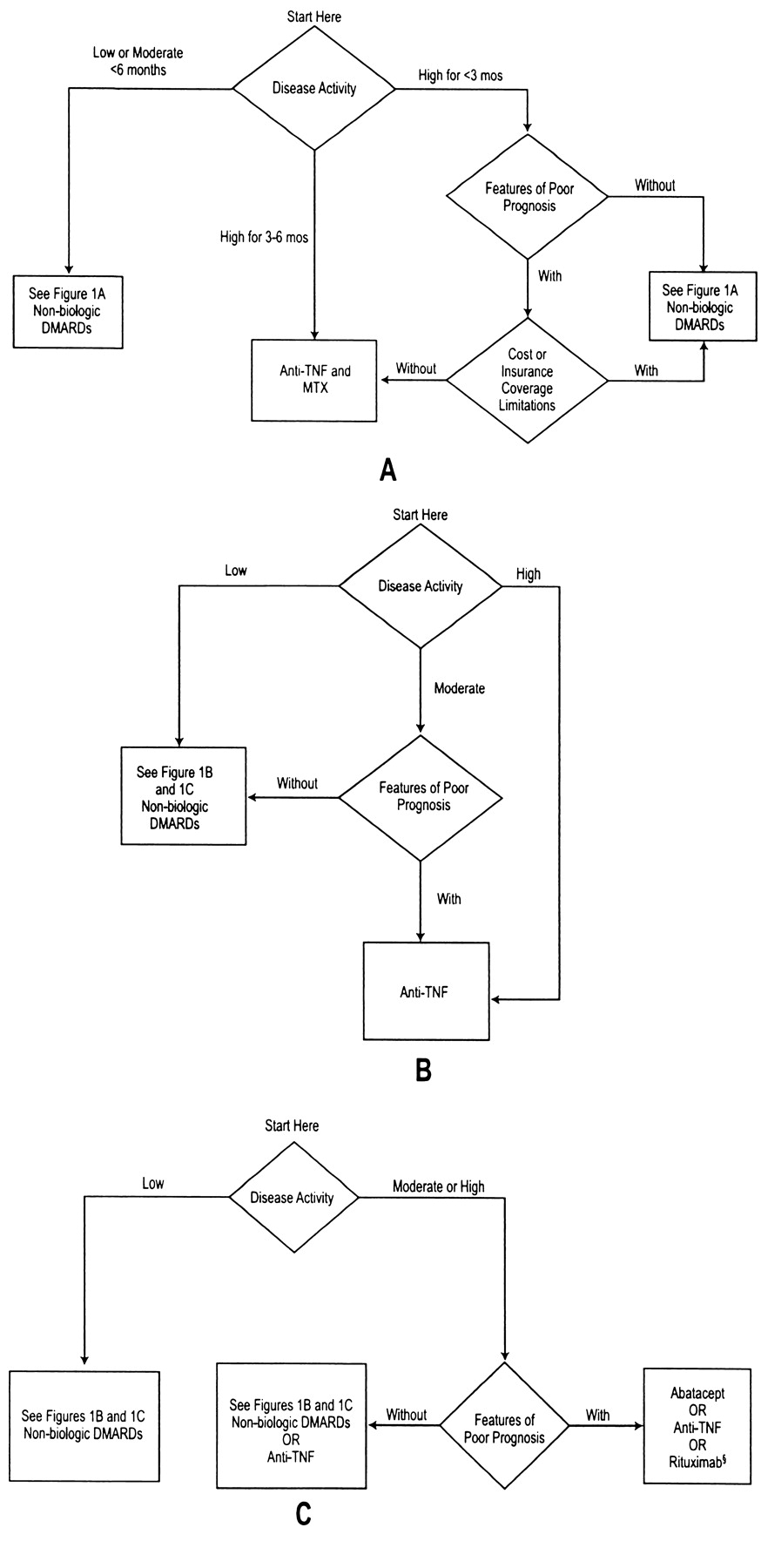
The recently published ACR recommendations provide a wider variety of treatment options than the European recommendations (Figures 1 and 2), depending on the patient’s disease duration and previous exposure to biologic DMARD9. The ACR also introduced into the treatment algorithms the features of poor prognosis. In the absence of biomarkers to assess prognosis, several clinical markers have been shown to correlate with long-term radiographic damage, including high baseline erosion scores, immunoglobulin M rheumatoid factor positivity, erythrocyte sedimentation rate (ESR) level higher than 33 mm/hour, the presence of DRB1*04 genes14, anti-cyclic citrullinated peptide antibody positivity15, and high CRP levels16. All these features, especially in combination, increase the likelihood of persistent and erosive disease. This concept of poor prognosis was taken a step further in the Active-Controlled Study of Patients Receiving Infliximab for the Treatment of Rheumatoid Arthritis of Early Onset (ASPIRE), where high DAS28 scores at Week 14 were also predictive of radiographic progression at one year16. This prognostic feature may be very valuable for assessing prognosis in daily practice. If patients do not respond to optimal MTX monotherapy after 3 months of treatment, the likelihood of radiographic progression is high; therefore, their DMARD therapy should be reassessed at this point.

ACR recommendations for the initiation of non-biologic disease modifying antirheumatic drugs in patients with disease duration < 6 months (A), 6 to 12 months (B), and > 12 months (C)9. §Recommended only for patients with high disease activity with features of poor prognosis. IIRecommended only for patients with moderate disease activity irrespective of prognostic features and patients with high disease activity without features of poor prognosis. # Recommended only for patients with high disease activity without features of poor prognosis. HCQ: hydroxychloroquine; LEF: leflunomide; MTX: methotrexate; SSZ: sulfasalazine; MIN: minocycline. Reprinted from Arthritis Rheum 2008;59:762–84, with permission.
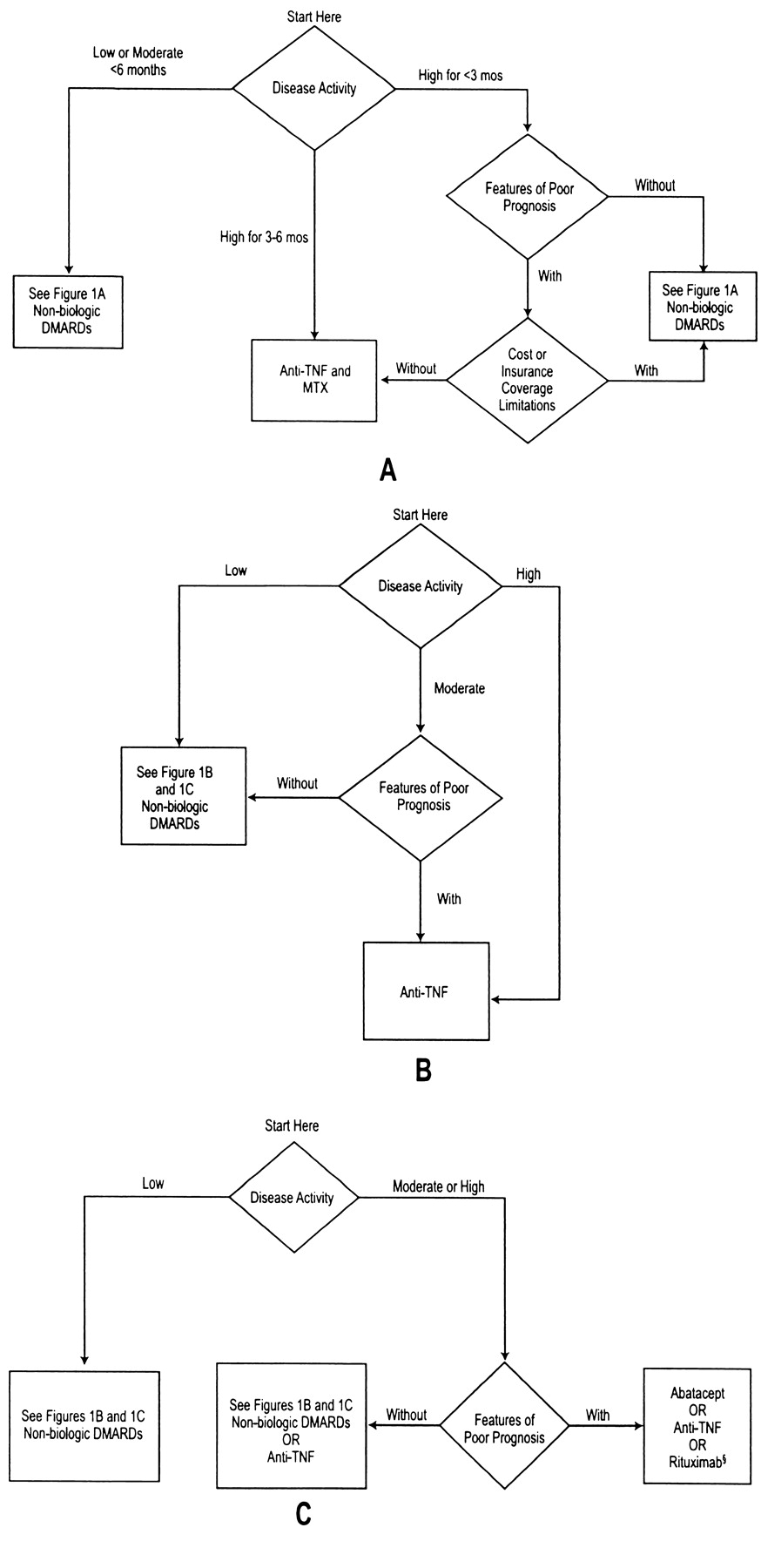
American College of Rheumatology recommendations for the initiation of biologic disease-modifying antirheumatic drugs (DMARD) in patients with disease duration of less than 6 months (A), 6 to 12 months (B), or longer than 12 months (C)9. § Recommended only for patients with high disease activity with features of poor prognosis. MTX: Methotrexate; TNF: Tumor necrosis factor. Reprinted from Arthritis Rheum 2008;59:762–84, with permission.
CONCEPTS OF TIGHT CONTROL AND TREATING TO TARGET
Since the 1990s, the standard of care for the treatment of early RA has been MTX monotherapy. Clinical trials have failed to show significant improvements in efficacy with initial combination therapies involving traditional DMARD, with the exception perhaps of hydroxychloroquine17. With the availability of tools to monitor disease activity in patients with RA, a relatively new concept in the treatment of RA is that of “tight control,” whereby strategies tailored to individual patients are implemented in order to meet predefined levels of low disease activity or remission18.
The concept of tight control was recently evaluated in 4 clinical trials: the TIght COntrol for Rheumatoid Arthritis (TICORA) trial19, the Finnish Rheumatoid Arthritis Combination Therapy (FIN-RACo) trial20, the Behandelstrategieen voor Reumatoide Artritis (BeSt) trial21, and the Computer Assisted Management in Early Rheumatoid Arthritis (CAMERA)-I trial22. In the TICORA and CAMERA-I trials, patients were assessed and the medication adjusted at one-month intervals, resulting in remission rates of 65% (vs 16% in routine care) and 50% (vs 37% in routine care), respectively. The FinRACo and BeSt trials, which assessed patients every 3 months, achieved remission rates of 51% (vs 16% in routine care) and 42%, respectively.
Kuper, et al recently assessed the feasibility of a step-up, tight-control approach to the treatment of DMARD-naïve patients with recent-onset RA in daily clinical practice23. The goal of treatment was remission, defined as a DAS28 below 2.6. Patients were started on MTX 15 mg/week and assessed at Weeks 8, 12, 20, and 24. If remission was not achieved at the 8-week assessment, the MTX dosage was increased to 25 mg/week. At Week 12, patients who failed to achieve remission were given sulfasalazine 2 g/day, and this dosage was increased to 3 g/day if remission was not achieved by Day 20. By Week 24, the patients who still had not achieved remission were given adalimumab in addition to their MTX. Among 169 patients with a mean baseline DAS28 of 5.1, this approach resulted in remission rates of 15.5% at Week 8, 22% at Week 12, 30.7% at Week 20, 38.8% at Week 24, and 52.1% at Week 36. Remission was maintained in 51% of patients after one year. The results of this study confirm that remission is a realistic goal for patients with early RA when treated under conditions of tight control in daily clinical practice23.
Radiographic outcomes
Based on the probability plots of radiographic progression, it has been observed that only a minority of patients – between 5% and 20% – have significant deterioration greater than the smallest detectable change and that it correlates well with disease activity, as measured by the SDAI16. Patients with higher disease activity at baseline, Week 14, or Week 54 had greater radiographic progression at Week 54 if they were treated with MTX alone than if they were treated with the combination of infliximab and MTX. For patients with low disease activity at Weeks 14 and 54, radiographic progression was slowed by MTX monotherapy, but was eliminated altogether by the addition of infliximab, with no radiographic progression observed in the combination group at Week 54. A similar correlation was observed between swollen joint count at Week 30 and radiographic progression at Week 5411.
A correlation between radiographic progression and ACR response was also observed in the PREMIER trial, which compared adalimumab 40 mg every other week plus weekly MTX with either agent alone in MTX-naïve patients with early RA24. For patients who received MTX monotherapy, the mean change in Sharp scores declined proportionately with higher ACR responses. In the group treated with the combination of adalimumab and MTX, radiographic progression was minimal, regardless of the level of ACR response.
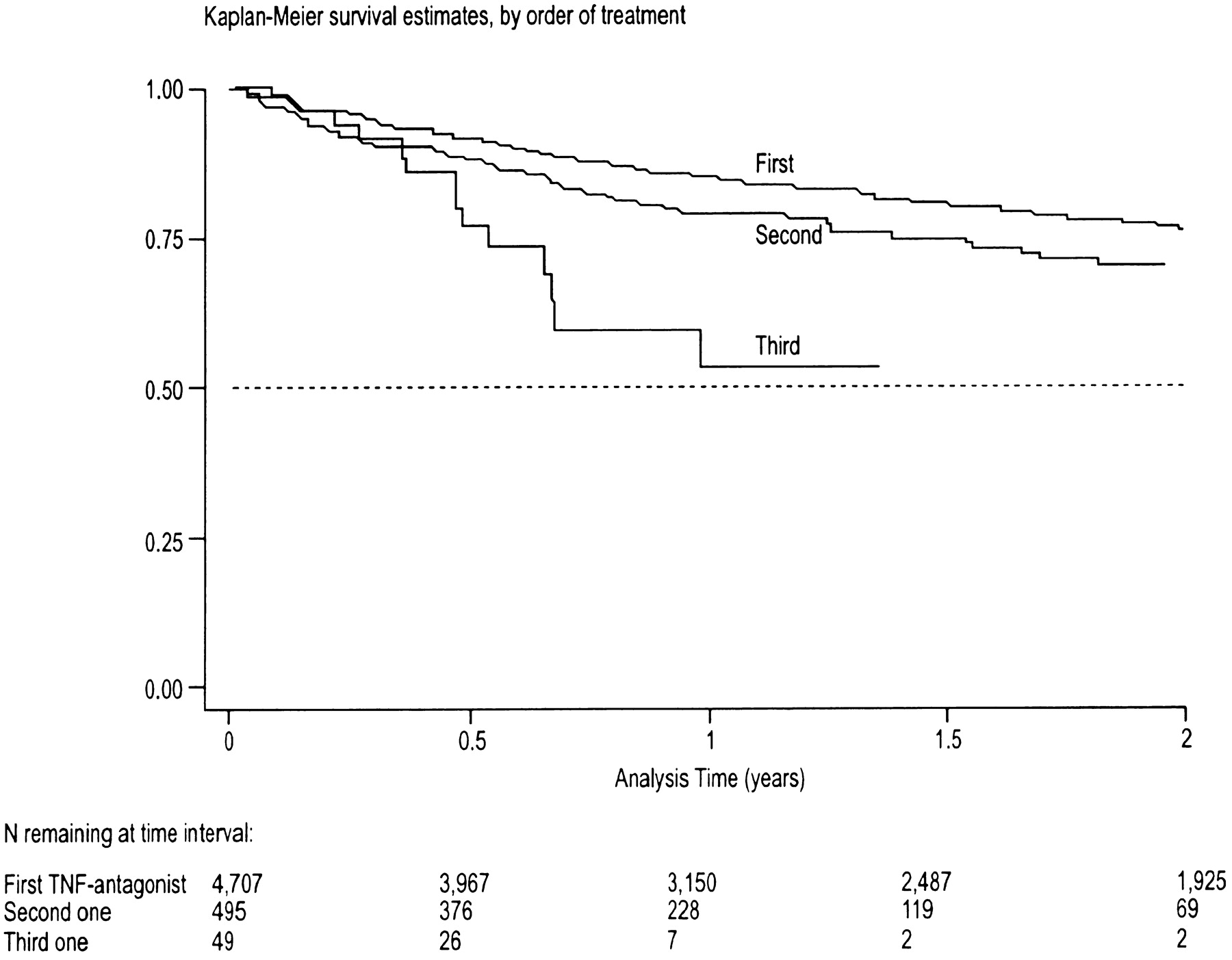
Despite advances in the treatment of early RA, a certain number of patients do not respond adequately to anti-tumor necrosis factor (TNF) agents and have persistent low or moderate disease activity. In the absence of radiographic progression, low levels of disease activity may be tolerated, as long as the patient is satisfied. There is significant evidence to suggest that patients with an inadequate response may benefit from switching to a second TNF inhibitor or to a biologic therapy with a different mode of action. In the British Society of Rheumatology Biologic Register, of the 6,739 patients with RA who were treated for the first time with an anti-TNF agent, 1,864 patients experienced treatment failure25. Among the 856 patients who switched to a second anti-TNF agent, the discontinuation rates ranged from 29% to 42%, depending on the agent, signalling some acceptable response rates. However, retention rates and clinical responses tend to decline further with repeated switching of anti-TNF agents, as shown by Spanish registry data (Figures 3 and 4)26,27. Only one randomized, controlled trial has assessed the efficacy of switching to a second anti-TNF agent. Golimumab, a new human anti-TNF-monoclonal antibody, was recently evaluated in patients with active RA despite previous treatment with an anti-TNF medication28. At the recommended dose of 50 mg monthly, patients achieved ACR20 and ACR50 values of 35.3% and 16.3%, respectively, compared with corresponding values of 18.1% and 6.5% in the placebo group at Week 14.

Survival curve for anti-tumor necrosis factor (TNF) usage among 488 patients (68% with RA) in a Spanish register during the first 2 years of treatment26.

European League Against Rheumatism (EULAR) response rates 3 months after initiation of anti-tumor necrosis factor (TNF) therapy in 488 patients in a Spanish register27.
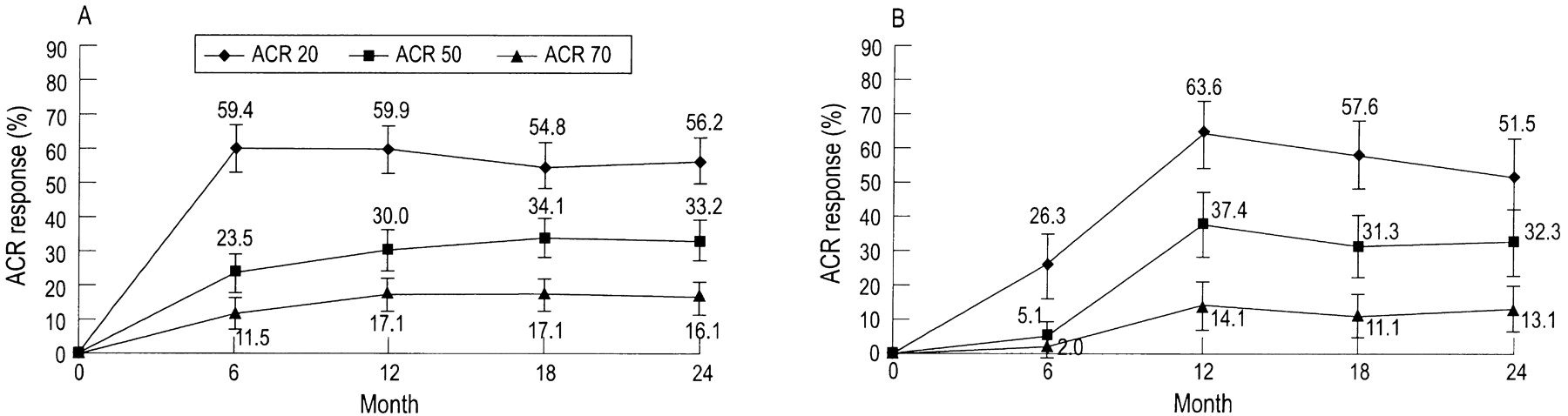
The mechanisms by which a patient would respond differently to agents within the same class have not yet been elucidated and would be an interesting subject for future study. Recent data also suggest that patients who fail to respond to an anti-TNF agent may benefit from switching to a biologic agent with a different mode of action. In the Randomized Evaluation of Long-Term Efficacy of Rituximab in RA (REFLEX) trial, patients with active RA who had failed to respond to one or more anti-TNF agents were randomly assigned to treatment with rituximab or placebo, both with background MTX treatment29. After 24 weeks of treatment, the overall ACR20, ACR50, and ACR70 responses were 51%, 27%, and 12%, respectively, in the rituximab group, compared with 18%, 5%, and 1%, respectively, in the placebo group. Response rates were lower among patients who had failed on 2 or more anti-TNF agents than among those who had failed on only one anti-TNF agent30. However, the change in response rate was still significant, as the response rates in the placebo group were also lower among patients who had failed 2 or more anti-TNF agents. These findings are not surprising, given the recalcitrant nature of disease among the subpopulation of patients who have failed multiple anti-TNF agents. Longterm followup in the REFLEX trial has shown that radiographic progression continues to decline after 2 years of therapy with rituximab versus placebo31. Similar results were seen in the Abatacept Trial in Treatment of Anti-TNF INadequate responders (ATTAIN), which randomly assigned 391 patients with RA and inadequate response to anti-TNF therapy to either abatacept or placebo32. After 6 months of treatment, the ACR20, ACR50, and ACR70 responses were significantly greater in the abatacept group than in the placebo group (Figure 5).
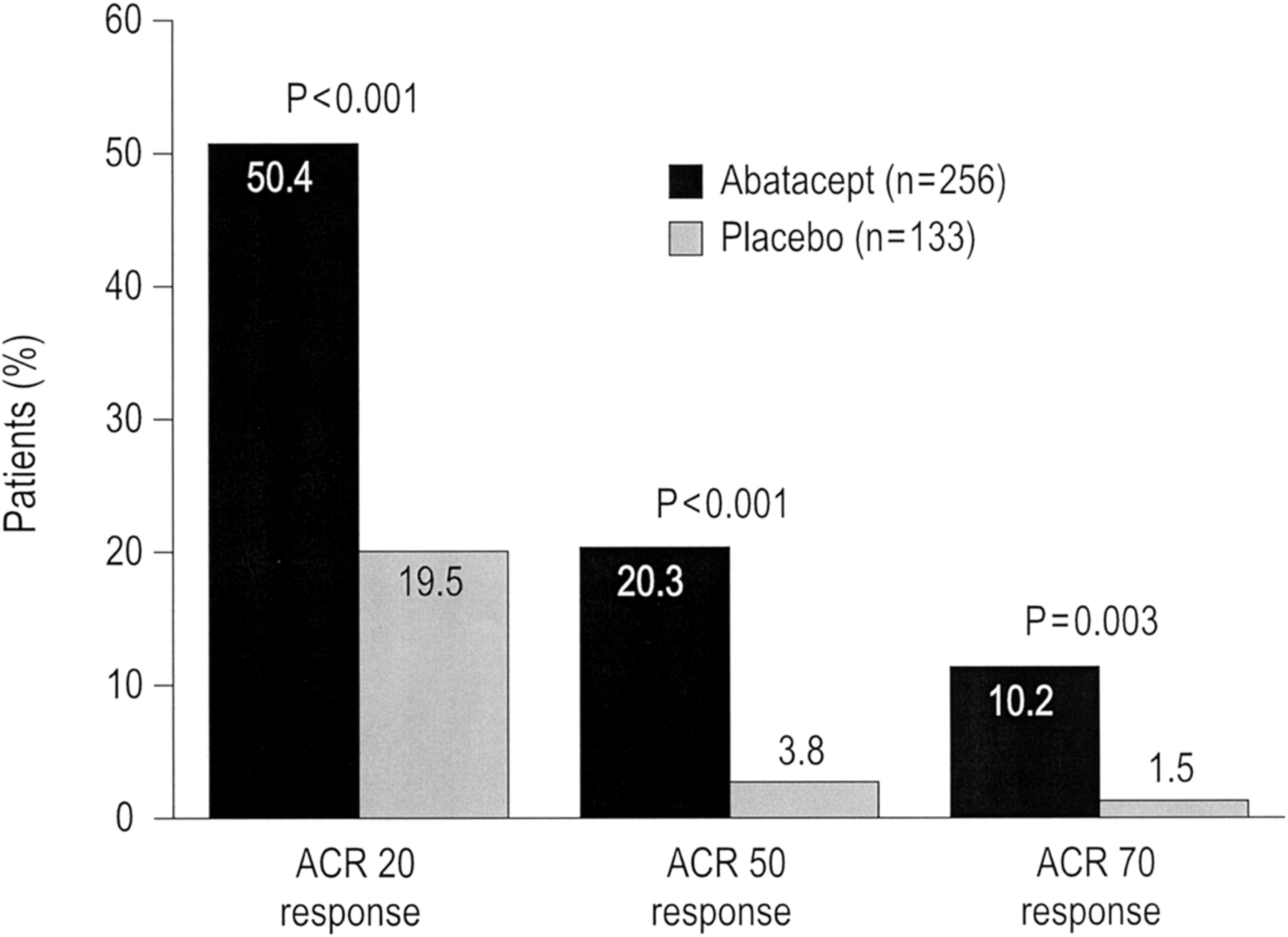
American College of Rheumatology (ACR) response rates among patients with rheumatoid arthritis who were switched to treatment with abatacept or placebo following failure to respond to an anti-tumor necrosis factor (TNF) therapy in the ATTAIN trial32. Reprinted from N Engl J Med 2005;353:1114–23, with permission.
These ACR responses were maintained in the abatacept group over 2 years, as shown in the longterm extension of the ATTAIN trial, where patients received abatacept at a dose of 10 mg/kg in addition to conventional DMARD (Figure 6)33. Retention rates for abatacept were high. At 2 years, 70% of patients were still taking abatacept; reasons for discontinuation included lack of efficacy (16.4%), adverse events (7.6%), and death (0.3%). Recent data presented in abstract form suggest that these responses and retention rates are maintained over 3 years34.

American College of Rheumatology (ACR) response rates over time among patients with rheumatoid arthritis who were originally switched to treatment with abatacept (A) or placebo (B) following failure to respond to an anti-tumor necrosis factor (TNF) therapy in the longterm extension of the ATTAIN trial33. Reprinted from Ann Rheum Dis 2008;67:547–54, with permission.
Randomized trials have not yet been conducted to compare the benefit of switching to a biologic agent with the benefit of switching to another anti-TNF agent. In one head-to-head observational study, patients with RA who had an inadequate response to at least one anti-TNF medication were subsequently treated with either one cycle of rituximab or with an alternative anti-TNF medication, at the discretion of the treating physician35. Of the 116 patients who met the inclusion criteria for the study, 50 received rituximab and 66 received a second or third anti-TNF agent. After 6 months of treatment, the changes in DAS28, ESR, and tender joint count were more favorable in the rituximab-treated group than in the group that had received an alternative anti-TNF agent.
CONCLUSIONS
With the advent of the biologic agents, tremendous progress has occurred in the paradigm of treatment of RA:
-
Treat early with rapid optimization of traditional DMARD. The cornerstone of treatment is the rapidly escalating doses of MTX to 20 to 25 mg per week, over 4 weeks, with a switch to the parenteral route when tolerability issues or suboptimal response is observed with the oral route36.
-
While there is no strong evidence that initial combination of DMARD with MTX is superior to MTX monotherapy, there is a general Canadian consensus that it is preferable to start with such combinations rather than wait to assess response to MTX monotherapy and subsequently add another DMARD when remission is not achieved.
-
Aim for remission or a minimal disease activity without further structural damage. In order to reach this target, patients need to be assessed as frequently as is feasible (every 1 to 3 months), using validated clinical outcome measures with frequent therapy adjustments aiming for the set goal.
-
Radiographic assessment should be carried out at regular intervals and therapy adjusted in those patients who display significant progression, even in the face of good clinical response. Patients should undergo regular radiographic assessment, regardless of their clinical status, as clinical trials continue to demonstrate a disconnect between clinical and radiographic progression.
-
Biologic agents should be initiated in patients who fail to achieve remission, or at least low disease activity without further radiographic damage and progression despite optimal treatment with traditional DMARD. The anti-TNF agents, as well as abatacept, have been shown to be effective clinically and radiographically, and are indicated.
-
Special attention should be carried out in patients with poor prognostic markers.
-
For patients who fail to have a satisfactory response to an anti-TNF agent, several options exist: abatacept, a switch to a second anti-TNF agent, or rituximab.
-
The choice of a biologic agent should be tailored to the individual patient based on the efficacy and the safety profile of the drug and the patient’s preference in terms of ease of administration.
Footnotes
-
Supported by an unrestricted educational grant from Bristol-Myers Squibb Canada.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}