

Abstract
Objective. Vascular pathology (changes in blood vessels) and osteoarthritis (OA) are both common chronic conditions associated with aging and obesity, but whether vascular pathology is a risk factor for OA is unclear. The aim of this study was to systematically review the evidence for an association between vascular pathology and risk of joint-specific OA.
Methods. Scopus, Ovid Medline, and EMBASE were searched from inception to February 2019. MeSH terms and keywords were used to identify studies examining the association between vascular pathology and OA. Two reviewers independently extracted the data and assessed the methodological quality. Qualitative evidence synthesis was performed.
Results. Fifteen studies with high (n = 3), fair (n = 3), or low (n = 9) quality were included. Features of vascular pathology included atherosclerosis, vascular stiffness, and endothelial dysfunction in different vascular beds. There was evidence for an association between vascular pathology and risk of hand OA in women but not men, and between vascular pathology and risk of knee OA in both men and women. Only 2 studies examined hip OA showing no association between vascular pathology and risk of hip OA.
Conclusion. There is evidence suggesting an association between vascular pathology and risk of hand and knee OA, with a potential causal relationship for knee OA. Based on the limited evidence, it is hard to conclude an association for hip OA. Further stronger evidence is needed to determine whether there is a causal relationship.
- VASCULAR PATHOLOGY
- ATHEROSCLEROSIS
- ARTERIAL WALL THICKNESS
- CAROTID INTIMA-MEDIA THICKNESS
- CAROTID PLAQUE
- OSTEOARTHRITIS
Osteoarthritis (OA) is a major cause of pain and disability, resulting in 128.9 million years lived with disability globally in 2015, an increase of 35% since 20051. OA affects the whole joint involving cartilage, subchondral bone, synovium, capsule, ligaments, and surrounding muscles2. No treatments for OA have been proven to have a disease-modifying effect, with joint replacement being the only option for endstage OA. Thus, prevention is important and will be optimized with a better understanding of the modifiable factors involved in the pathogenesis of OA.
Pathological changes in blood vessels (vascular pathology), particularly atherosclerosis or thickening of arterial wall, and OA are both common chronic conditions associated with aging and obesity2. People with OA are at higher risk of death from cardiovascular disease compared with the general population. Knee OA is more prevalent among hypertensive individuals compared with nonhypertensive individuals3. Higher levels of serum cholesterol are associated with increased risk of knee and generalized OA4,5. However, the association between vascular pathology and OA remained inconclusive because some studies reported a positive association between arterial narrowing and risk of hand and knee OA3,6,7,8,9, while others found no association between arterial stiffness and knee OA10,11.
Emerging evidence suggests that different joints are susceptible to different risk factors for OA. The knee and hand joints are more affected by obesity-associated inflammation12 and metabolic factors13. In contrast, alterations in bony shape or geometry are linked to hip OA, with weak or inconsistent associations for metabolic or inflammatory factors14. We aimed to systematically review the evidence for the relationships between vascular pathology and risk of joint-specific OA.
MATERIALS AND METHODS
The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines15.
Search strategy
These databases were searched: Ovid Medline (between January 1946 and February 2019), Scopus (between January 1937 and February 2019), and EMBASE (between January 1974 and February 2019), using MeSH terms and keywords to identify studies examining the role of vascular involvement in the pathogenesis of OA. The search terms are outlined in Supplementary Data 1 (available with the online version of this article). Searches were limited to human studies published in English. Identified manuscripts were reviewed manually and references searched for additional relevant studies.
Study selection
SMH and CD independently assessed the eligibility of studies using a 3-stage determination method, reviewing the title, abstract, and then full text. Any disagreement between the 2 authors was resolved by discussion. We included studies examining knee, hip, or hand OA using a validated definition including the American College of Rheumatology criteria, Kellgren–Lawrence (KL) score, and arthroplasty for OA. We also included studies that examined magnetic resonance imaging (MRI) structural changes associated with OA. Studies were included that assessed the exposure of interest, measuring vascular pathology comprising atherosclerosis, arteriolar or arterial wall thickness, vascular stiffness, microvascular derangement, endothelial dysfunction, and venous drainage. We excluded case reports, conference abstracts, review articles, and studies without a comparison group. We also excluded studies with heterogeneous populations that were a mix of participants with OA of the knee, hip, or hand, because previous studies showed that different sets of joint-specific risk factors are associated with the onset and progression of the disease16,17,18,19 and much of the genetic basis for OA occurs on a joint-specific basis20,21,22,23,24.
Data extraction and synthesis
SMH and CD extracted data on study design, number/sex/age of study participants, type/definition/prevalence of OA, length of followup (Table 1), measures of vascular pathology, confounding factors being adjusted for, and associations (all available mean differences, risk ratios, OR, HR, regression coefficients) between vascular pathology and OA (Table 2 and Table 3). Qualitative synthesis was performed owing to the heterogeneity of the included studies.
General characteristics of included studies.
Association between vascular pathology and hand osteoarthritis (OA).
Association between vascular pathology and knee, hip, and facet osteoarthritis (OA).
Risk of bias assessment
SMH and LC independently assessed risk of bias of included studies using the US National Heart, Lung, and Blood Institute quality assessment tool for observational studies25. The tool includes 14 criteria for cohort and cross-sectional studies and 12 criteria for case-control studies. Each criterion was rated as yes, no, cannot determine, not applicable, or not reported, with overall quality of studies being scored as high (low risk of bias), fair (moderate risk of bias), or low (high risk of bias).
RESULTS
Search results
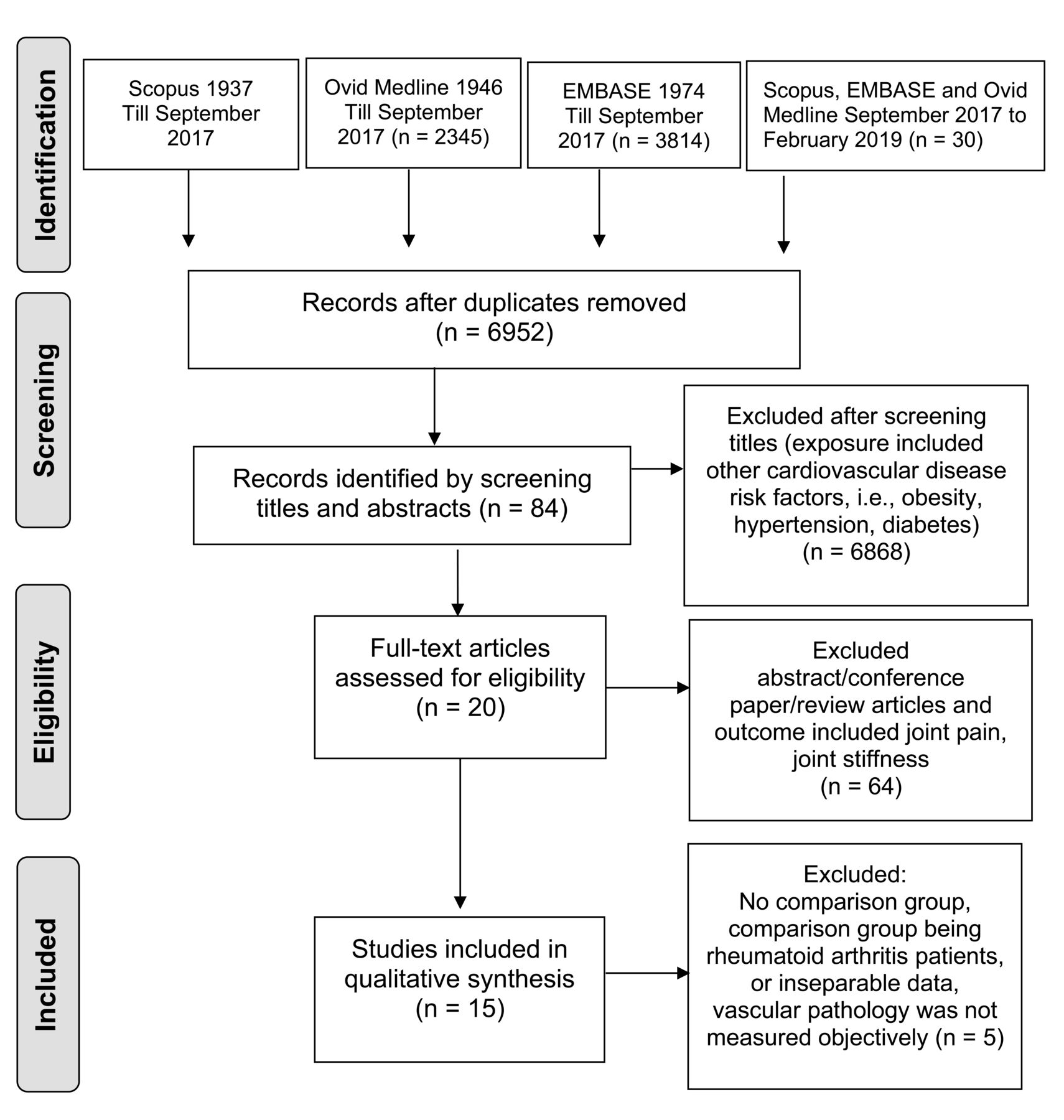
The search of the 3 electronic databases identified 8296 records until September 2017 (2137 from Scopus, 2345 from Ovid Medline, and 3814 from EMBASE) and a further 30 records from September 2017 to February 2019, with 6952 articles remaining after removal of duplicates. By screening titles and abstracts, 6868 articles were excluded because they assessed risk of OA in relation to markers or risk factors of cardiovascular disease (serum cholesterol, fatty acids, hyperuricemia, obesity, hypertension, diabetes, lipid abnormalities, or metabolic syndrome). Eighty-four articles were retrieved, with 64 studies excluded because they were abstracts, conference papers, or review articles, or the outcome was self-reported joint pain or stiffness. Full-text screening was performed for 20 articles, with 5 excluded because they had no comparison group, had an inappropriate comparison group (e.g., patients with rheumatoid arthritis), examined heterogeneous populations (i.e., where they were mixed regarding type of OA), or did not measure vascular pathology objectively (Figure 1). No additional article was found after searching the references of review articles.

Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram of included articles.
Description of included studies
Table 1 provides an overview of the included studies. The studies were published between 2007 and 2019, including 6 cohorts3,6,8,26,27,28, 3 case-control studies9,29,30, and 6 cross-sectional studies7,10,11,31,32,33. Four studies originated from Australia3,8,27,32, 3 from Turkey29,30,31, 3 from Iceland7,10,28, 2 each from the Netherlands6,26 and the United States11,33, and 1 from Greece9. The mean age of participants ranged from 50 to 76 years. Twelve studies included both men and women3,6–11,26,28,30,32,33, and 3 studies included women only27,29,31.
Assessment of OA
OA was examined in hand6,7,9,11,31, knee3,6,8,10,26,27,29,30,32, hip6,10, and facet joint33 by using the KL scores6,11,26,29,30,31, bone erosion from radiographs9, computed tomography (CT)7,10,28,33, scored hand photographs7,10,28, presence of cartilage defects or bone marrow lesions on MRI8,27,32, or arthroplasty for OA3,10,28.
Assessment of vascular pathology
Vascular pathology was examined for atherosclerosis3,6–10,26,27,29,31,32, vascular stiffness6,7,10,11,26, aortic elasticity and stiffness30, change in retinal vascular caliber3,28,32, and endothelial dysfunction9, in a number of different vascular beds including common carotid artery6,9,26,31, coronary artery7,10,11,31, abdominal aorta30,33, common femoral artery9,29, tibial artery29, popliteal artery8,27, or retinal vessels3,28,32. The variables used to measure vascular pathology were carotid intima-media thickness (IMT)6,7,9,10,26, carotid plaque severity6,9,26, coronary and/or aortic calcifications7,10,26, plasma levels of biomarkers (soluble CD40 ligand, vascular cell adhesion molecule 1, and vascular endothelial growth factor)26, Gensini scoring of coronary angiogram31, popliteal artery wall thickness8,27, retinal microvasculature3,28,32, arterial pulse wave velocity (PWV)11,29, flow volume29, flow-mediated dilatation and sublingual glyceryl trinitrate–induced dilatation of the brachial artery9, or transthoracic echocardiography of aorta30.
Data synthesis
The prevalence of OA at individual joints could be established in 9 studies3,6,7,10,11,26,28,31,33, which varied depending on the definition of OA. The prevalence of knee OA was 4–7% when defined by arthroplasty for OA3,10,28 and 14–18% when defined using the KL score from radiographs6,26. The prevalence of hip OA was 6% from radiographs and arthroplasty6,10. Two studies reported the prevalence of hand OA: 64% from radiographs31 and 68% from hand photographs7. One study reported the prevalence of OA of distal interphalangeal (33%), proximal interphalangeal (12%), metacarpophalangeal (MCP; 5%), and carpometacarpal/trapezoscaphoid joints (27%)6. The prevalence of facet joint OA was 30% using CT scans33. Three studies reported sex-specific prevalence of OA6,7,26,28. Knee OA was more prevalent in women than in men (20% vs 9%6, 23% vs 11%26, and 7% vs 5%28), while hand (69.8% vs 67.4% and 48% vs 43%28)7 and hip (7% vs 5%)6 OA had similar prevalence in women and men.
Risk of bias
There were 3 high-quality3,6,26 and 3 fair-quality8,27,28 cohort studies. All the 3 case-control and 6 cross-sectional studies were of low quality7,9,10,11,29,30,31,32,33. The study population and research question were defined clearly in most studies. The main issues were the lack of sample size justification, and measurement of exposures at only 1 timepoint for cohort studies. The overall quality assessment is shown in Table 1, with details of quality assessment presented in Supplementary Table 1 (available with the online version of this article) for cohort and cross-sectional studies, and Supplementary Table 2 for case-control studies. The initial agreement between the 2 reviewers was 78%.
Vascular pathology and hand OA
Six studies examined the relationship between vascular pathology and risk of hand OA6,7,9,11,28,31 (Table 2). In a high-quality cohort study, baseline IMT was associated with the progression of MCP OA in women but not the prevalence of hand OA6. Baseline carotid plaque was associated with greater baseline prevalence of distal interphalangeal and MCP OA in women but not the progression of hand OA6. After correction for multiple testing, the association persisted as statistically significant between baseline carotid plaque and prevalent distal interphalangeal OA6. There were no significant associations in men in all analyses6. One case-control and 2 cross-sectional studies found that atherosclerosis of carotid and coronary artery was associated with higher prevalence of hand OA7,9,31. Two studies also showed that those who had more severe atherosclerosis measured by IMT9 and Gensini score of angiogram31 were more likely to have hand OA, although they did not adjust for confounders. In the AGES-Reykjavik study, narrow retinal arteriolar caliber was associated with hand OA for both men and women28. Among the Framingham population, the association between PWV (a measure of vascular stiffness) and hand OA was no longer significant after adjustment for age11.
Vascular pathology and knee OA
Ten studies examined the association between vascular pathology and risk of knee OA3,6,8,10,26–30,32 (Table 3). Among the 6 cohort studies, 4 studies examined the association between baseline vascular pathology and risk of knee OA6,26,28 or knee structure8 both cross-sectionally and longitudinally. Higher baseline levels of atherosclerosis markers (i.e., CD40L26 and carotid IMT6) were associated with higher prevalence of knee OA measured by radiological KL score in women; greater baseline popliteal artery wall thickness was associated with reduced medial tibial cartilage volume on MRI8; and narrow retinal arteriolar caliber was associated with knee replacement due to OA in men and women28. Three cohort studies examined the longitudinal relationship between baseline vascular pathology and risk of OA or knee structure and showed significant associations: retinal arteriolar narrowing was associated with increased risk of knee arthroplasty for OA in the AusDiab study population3; similarly, in the AGES-Reykjavik study, retinal arteriolar narrowing was associated with incident knee replacement for OA28, and greater popliteal arterial wall thickness was associated with increased rate of tibial cartilage volume loss on MRI27. In a low-quality study, aortic stiffness was associated with the prevalence and severity of knee OA measured by radiological KL score30. Wider retinal venular diameter was associated with increased prevalence of bone marrow lesions on MRI in a cross-sectional study32, and lower extremity arterial blood flow was associated with increased risk of knee OA in a case-control study29. In contrast, there was insufficient evidence to suggest either carotid IMT or plaque was associated with knee OA progression in women or men6. No significant association was found between the following: presence or progression of knee OA and baseline coronary artery calcification26; knee replacement for OA and retinal venular caliber3; knee arthroplasty and coronary and aortic calcification, periventricular white matter hyperintensities10; presence and progression of bone marrow lesion and popliteal artery wall thickness8,27; or presence of bone marrow lesion in the knee and arterial diameter32.
Vascular pathology and hip and facet joint OA
Two studies examined the association between vascular pathology and risk of hip OA6,10. There was no association between the prevalence of hip OA assessed by radiological KL score and coronary artery calcification or carotid plaque6, or between the incidence of hip arthroplasty for OA and coronary and aortic calcification, periventricular white matter hyperintensities, cardiac, or cerebral events10. One study examined the association between vascular pathology and risk of facet joint OA and found that abdominal aortic calcifications were associated with facet joint OA in a community-based population33.
DISCUSSION
This study systematically reviewed the evidence for an association between vascular pathology and risk of joint-specific OA, with syntheses derived from 15 studies. There was evidence, irrespective of the quality of the studies, that vascular pathology was associated with risk of hand and knee OA but not hip OA. Further, there was evidence that vascular pathology was associated with a spectrum of knee OA outcomes, including progression of structural changes that predict development of knee OA, progression of radiographic OA, and endstage OA requiring a joint replacement.
Five studies, including one high-quality cohort study, found that vascular pathology was associated with hand OA6,7,9,28,31. The only cohort study showed that in women carotid plaque was associated with higher prevalence of hand OA and carotid IMT with progression of hand OA6. Atherosclerosis measured in the carotid and coronary artery was associated with hand OA in a case-control9 and 2 cross-sectional studies7,31. Similarly, generalized vascular pathology was associated with prevalence of hand OA28. In contrast, a low-quality cross-sectional study that included subjects across a wide age range (19–93 yrs) and used PWV, a less accurate method to assess atherosclerosis34, did not show a relationship between arterial stiffness and risk of hand OA11.
Different measures of vascular pathology were associated with increased risk of knee OA and early knee structural changes predictive of knee OA, based on 9 studies including 3 high-quality and 3 fair-quality cohort studies3,6,8,26–30,32. The vascular pathologies included narrowing of large arteries (carotid artery, coronary artery, aorta, or popliteal artery), narrowing of small arteries, or dilation of small veins (retinal arterioles and venules). No association between arterial calcification and risk of knee OA could be established26. Measurements of IMT and arterial calcification are often discordant35, with IMT being more sensitive than arterial calcification for the detection of atherosclerosis36. In contrast, there was no association between vascular pathology and the risk of hip OA as evidenced from 1 high-quality cohort6 and 1 cross-sectional study10. Only 1 study examined the association between vascular pathology and facet joint OA and found a positive association33.
The results of this systematic review lend support to the hypothesis that vascular pathology may be involved in OA initiation and progression37, with consistent evidence for an association of vascular pathology with hand and knee OA. Among the 6 cohort studies of the knee, 2 examined early knee structural changes in people free from clinical OA8,27, and the other 4 studies included people with different stages of OA3,6,26,28. A positive association was found between the severity of vascular pathology and the likelihood of having hand or knee OA3,6,7,8,26,27,29,32. The association between vascular pathology and risk of OA was joint-specific, which was seen for hand and knee OA3,6–9,26–29,31,32 but not hip OA6,10. However, caution is needed given the limited number of studies on hip OA.
We applied the Bradford Hill criteria38 to further explore whether there was a causal relationship between vascular pathology and OA. The criteria, along with a description of how an association was established, are included in Supplementary Table 3 (available with the online version of this article). All the Bradford Hill criteria were met for knee OA. However, none of the high- and fair-quality studies were designed with the primary aim of examining the association between vascular pathology and OA. Thus, although the evidence supports a causal link, further high-quality studies are needed to determine whether targeting vascular pathology will reduce the burden of OA.
These findings cannot be simply explained by reverse causation, in which pain resulted from OA may reduce physical activity and thus increase the risk of obesity and metabolically driven inflammation and vascular disease. This is because 6 cohort studies included in this review showed that vascular pathology at baseline predicted structural progression of OA over the subsequent 2–10 years3,6,8,26,27,28 (Supplementary Table 4, available with the online version of this article). The 2 cohort studies of asymptomatic participants without clinical knee OA found an association between vascular pathology and early structural changes that are predictive of knee OA development8,27. Animal studies, where vascular changes were induced in a laboratory environment, showed that vascular pathology is involved in the initiation of OA39,40. Data from human cohort studies showed that statins used to treat atherosclerosis were associated with reduced progression of knee OA21 and reduced risk of OA at any site41. Taken together, these findings suggest that vascular pathology may be on the causal pathway of OA development and progression. Further, all the high- and fair-quality studies and most of the low-quality studies controlled for obesity, dyslipidemia, hypertension, and diabetes as confounders in the statistical analyses. It is less likely that the observed association is due to residual confounding, because we observed consistent results in all the included studies with a variety of study designs, study populations, methods, and stages of OA.
In this review, conducting a metaanalysis was not possible owing to the heterogeneous characteristics of study populations, definition of OA, and measurement of vascular pathology. The extent to which individual studies measured and adjusted for potential confounders varied. The quality of the included studies was generally low. As with any systematic reviews, our study is subject to the potential of publication bias that may have inflated the association between vascular pathology and the risk of OA. To minimize this, we performed an extensive search for all relevant studies in 3 databases, examined biological plausibility (with obesity, lipids, glucose) and animal data, and considered the Bradford Hill criteria. Nonetheless, we carefully assessed the risk of bias for each included study using established tools.
Articular cartilage is avascular and depends on synovial fluid secreted by synovium42 and subchondral bone for nutrition and gas exchange37. Narrower arterioles in synovium may result in localized hypoxia that stimulates angiogenesis, development of an immature vasculature and inflammation predictive of cartilage damage, and catabolic effects on chondrocytes42. The growth, repair, and metabolism as well as modeling and remodeling of subchondral bone may depend on blood flow and hemopoiesis37. Decreased blood flow may initiate osteoclastic resorption resulting in impaired integrity of subchondral bone, leading to reduced bony support for the overlying cartilage and subsequent higher susceptibility of cartilage to damage37. Arterial narrowing may also affect the integrity of ligaments43, tendons44, and skeletal muscles45, which are important structures for joint health. Venous occlusion and stasis may result in increased intraosseous pressure. Compromised venous drainage may decrease interstitial fluid flow; as a result, the removal of waste products is reduced, an extremely deleterious situation for osteocytes and surrounding tissues37,46.
There is evidence of an association between vascular pathology and the risk of hand and knee OA, but not hip OA. Although these findings need to be confirmed by further high-quality studies, including longitudinal studies of disease-free participants at study inception, our systematic review provides support for the heterogeneity in the pathogenesis of OA. Understanding this will be important in optimizing the prevention and treatment of OA.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
SMH is the recipient of NHMRC Early Career Fellowship (#1142198); AEW is supported by NHMRC TRIP Fellowship (#1150102); and LC is the recipient of an Australian Postgraduate Award and Arthritis Foundation (Victoria) Fellowship.
- Accepted for publication May 17, 2019.








{kind=link}