

Abstract
Objective. To examine to what extent disabling osteoarthritis (OA), leading to a prolonged sickness absence (SA), interferes with work participation and shortens working life–years.
Methods. A total of 4704 wage earners aged 30 to 59 years, whose SA due to OA started in 2006, were followed until October 31, 2014. Kaplan–Meier analysis was used to plot sustained (at least 28 consecutive days) return-to-work curves. The associations of potential determinants with early exit from paid employment were examined applying Cox proportional hazards regression analysis. Years expected to be spent in different work participation statuses until statutory retirement age were estimated based on daily work participation statuses using adapted Sullivan method.
Results. Persons with knee OA showed the fastest, and persons with hip OA the slowest, sustained return to work. Although most participants typically were at work during the first year of followup, a considerable proportion was permanently retired. Male sex, older age, low education, long initial SA, and having not returned to work sustainably, as well as receiving vocational rehabilitation, predicted early exit from paid employment during the followup. Overall, only 45–53% of potential working life–years were estimated to be spent at work, being highest for the oldest age group.
Conclusion. Our study showed a considerable effect of OA on work participation and working life duration. Clinicians should avoid prescription of long SA or temporary work disability due to OA without a clear treatment or return-to-work plan.
Musculoskeletal conditions such as osteoarthritis (OA) are the leading cause of reduced work participation and have raised the interest of clinicians in recent years1. OA affects 240 million people globally, about 10% of men and 18% of women over 60 years of age, and it has been ranked as the 10th leading contributor to global years lived with disability2,3. As populations are aging, the disability associated with OA can critically affect the extension of work careers.
Epidemiological evidence concerning the effect of OA on work participation is scarce and contradictory. A systematic review by Bieleman, et al4 concluded that knee and hip OA had only a mild negative effect on work participation. However, another review by Palmer5 reported that knee OA considerably impairs work participation. More recent studies suggest a major effect of OA on work participation and work retention. A population-based study found that men below 60 years with hip OA had a 20% lower employment rate compared to those without OA6. Further, men below 55 years with OA were 2 to 3 times more likely to be out of work for a full year compared with those without OA. Among persons with OA aged over 50 years, almost 1 of 4 left their workplace prematurely7. A qualitative study among younger and older persons with arthritis showed that work participation was primarily affected among the older persons8. Moreover, persons in physically demanding occupations are more likely to be on sickness absence (SA) or prematurely retired because of OA than those in occupations with physically less demanding work tasks9,10,11.
Most previous studies have focused on one outcome at a time, such as risk of SA or disability pension10,12, or return to work after arthroplasty13,14,15. Yet, the majority of persons with health problems are in transition between work, SA, unemployment, and retirement. Little is known concerning the pathways out of work among persons with disabling OA.
We studied time to sustained return to work after prolonged SA due to different types of OA among Finnish wage earners, as well as the transitions between, and time spent in, different work participation statuses during a followup of up to 9 years. Additionally, we estimated the expected years at work and years lost because of OA. Finally, we assessed the demographic, socioeconomic, and occupational determinants of early exit from paid employment.
MATERIALS AND METHODS
Setting, design, and data sources
We carried out a population-based study, using registry data from a 70% random sample of the Finnish population aged 18–70 years living in Finland on December 31, 2004 (∼2.5 million). Included in the study were persons aged 30–59 years who were employed or self-employed on January 1, 2006 (n = 1,210,231), and had SA due to OA ≥ 2 weeks starting in 2006. We excluded persons who had a prior SA due to OA in 2005 or received any retirement-related benefit prior to January 1, 2006. Our cohort consisted of 4704 persons (2644 men and 2060 women, 0.39% of the eligible study population) who were followed from the first day of their first SA due to OA in 2006 until October 31, 2014.
The data included information on SA benefits, rehabilitation allowances, and national pensions obtained from the Social Insurance Institution of Finland (SII); employment periods and earnings-related pensions from the Finnish Centre for Pensions (FCP); and sociodemographic factors and occupational history from the Finnish Longitudinal Employer–Employee Data (FLEED) of Statistics Finland. Date of death from the Population Information System was provided to the study by the SII.
SA
SA is compensated by the SII as part of the national social security system until a maximum of 300 weekdays (Sundays excluded). Both employed and self-employed are eligible for compensation. The register of the SII provides information on the start and end dates as well as primary diagnoses for all full SA spells longer than 10 working days, and for all part-time SA spells. The diagnoses, set by the treating physician, were classified according to the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10, Finnish version of ICD classification 1996). The diagnoses of primary interest for this study were M15 (polyarthritis), M16 (hip OA), M17 (knee OA), M18 [carpometacarpal (CMC) joint OA, later referred to here as CMC joint OA], and M19 (other OA). For the analysis, the OA of the CMC joint and polyarthritis were combined.
Disability retirement
In Finland, disability pension may be granted as full or partial, depending on the degree of decreased work ability. If there is a possibility to restore the employee’s work ability through rehabilitation or treatment, a temporary pension for a fixed period can be granted by the pension provider. Temporary disability pension can be continued after an initial period; however, a decision regarding permanent disability pension is made within 2 years. The decision on a disability pension is based on a review of documents by an insurance physician who is not involved in the treatment of the patient. The FCP register provides information on all disability retirement events (full or partial, permanent or temporary), with their primary and secondary diagnoses, which are classified according to ICD-10.
Employment and unemployment
All employment and unemployment periods with their start and end dates were provided by the registers of the FCP and FLEED.
Rehabilitation allowance
Vocational rehabilitation is a statutory right in Finland. Eligible are persons assessed to have a threat of disability retirement within the next few years due to a diagnosed disease or an injury and who are expected to benefit from vocational rehabilitation. The main types of vocational rehabilitation include work tryouts, training, and counseling. Medical rehabilitation is not part of vocational rehabilitation. The registers of the FCP and SII provided information on the start and end dates of the vocational rehabilitation periods16.
Sociodemographic factors and occupational history
The geographic region, level of education, annual income, and occupation and employment sectors of each person were obtained from FLEED based on information gathered in 2005. Geographic regions consisted of (1) Southern Finland, (2) Western Finland or Åland, (3) Eastern Finland, and (4) Northern Finland. Level of education was defined as (1) higher or lower tertiary, (2) secondary, and (3) primary. Employment sector was classified as (1) public, (2) private, and (3) other, including self-employment. The occupations were classified up to the 4-digit level according to the Classification of Occupations 2001 by Statistics Finland, which is based on the International Standard Classification of Occupations. Only major (1-digit level) occupational groups were used in the analysis. Income consisted of both wage and capital income of the individual and was categorized into tertiles (high, medium, and low).
Physical and psychosocial work-related factors
Heavy physical work, kneeling, or squatting at work, manual handling of heavy loads (heavy lifting), awkward trunk posture, high job demands, and low job control were estimated with a sex-specific job exposure matrix17,18.
Work participation statuses
We focused on 8 work participation statuses: (1) at work (having employment and not receiving any benefit); (2) on partial work disability (receiving partial work disability benefit, including partial sickness benefit and partial disability retirement); (3) on SA because of OA (receiving full SA benefit); (4) on time-restricted full work disability (including full sickness benefit owing to other reason than OA, temporary disability retirement, vocational rehabilitation); (5) unemployed; (6) economically inactive (not at work and not receiving ill health–related or unemployment benefit, or pension); (7) on permanent disability retirement; and (8) on old age retirement.
Outcomes
We defined sustained return to work as returning to regular duties for a minimum of 28 consecutive days immediately following SA19.
Time spent in different work participation statuses
Based on daily work participation statuses, we calculated the proportion of time the person spent in each status for each year of the followup. The followup started from the day following the last day of the initial SA period until death, permanent retirement, or October 31, 2014, whichever came first.
We calculated potential working life–years lost based on actual retirement age (permanent disability retirement or old age retirement) and working life expectancy tables forecasted for Finland for the time period in question20. For persons who retired during followup, we searched the expected remaining years spent at work for the age and year the person in question retired. For those who did not retire during followup, the potential working life–years lost were set to zero. We defined early exit from paid employment as transiting to permanent disability retirement or old age retirement prior to the age of 63 years.
Because potential working life–years lost were only partially observed for permanent disability retirement and early old age retirement at the end of the followup, we also estimated years expected to be spent in different work participation statuses (at work; on ill health–related benefit while employed; temporarily out of work due to being unemployed or economically inactive; permanently retired, including full disability retirement and early old age retirement) until the official retirement age (63 yrs).
Ethics approval
The researchers used fully anonymous registry data, for which ethics committee approval is not needed according to Finnish legislation. Statistics Finland linked its data to those of the SII and the FCP, after which the data were anonymized and stored by Statistics Finland. The researchers analyzed the anonymous data using a remote access system. All output extracted from the system was approved by Statistics Finland to ensure compliance with data protection regulations.
Statistical analysis
We used Kaplan–Meier analysis to plot sustained return to work curves. The followup started on the first compensated day of SA due to OA and continued until the last day of SA. The followup time was counted in days.
We estimated the associations of potential determinants [sex, age, site of OA (dummy variable), duration of initial SA due to OA, education, geographic region of Finland, sector of employment, income, physical and psychosocial work-related factors, sustained return to work, dominant work participation status during the first followup year, and participation in vocational rehabilitation during followup] with early exit from paid employment, applying Cox regression analysis. We assessed visually the proportional hazard assumption through inspection of the log-log hazards plots21 and found it to be satisfactory. We used a constant time in Cox regression to control for variance instead of exact time to the event22; therefore, we exported the estimated associations as relative risk with 95% CI.
We adapted the Sullivan method23 for healthy life expectancy to calculate years expected to be spent in different work participation statuses. These calculations were carried out for the age range 30 to 59 years, corresponding to our study population at baseline and plotted in 5-year intervals (30, 35, 40, 45, 50, and 55 yrs).
The SAS 9.4 statistical software was used for the analyses (SAS Institute Inc.).
RESULTS
The average age of the study population was 51.5 years (95% CI 51.3–51.6) and there was a slight preponderance of women (56.2%). For more than half of the persons with SA due to OA, the knee joint was affected, followed by hip OA (18.6%) and other OA (16.2%), while polyarthritis or CMC joint OA was rare (7.8%; Table 1). In the polyarthritis or CMC joint OA group, more than three-quarters were women, while hip OA was more common among men. Those with polyarthritis or CMC joint OA were somewhat older, less educated, and more likely working in manual occupations than the others. There were no large differences between the hip and knee OA groups.
Baseline characteristics of the study population (n = 4704; 2060 men and 2644 women).
Persons with knee OA showed the fastest sustained return to work (median time to sustained return to work 31 days), while time to sustained return to work was the longest for persons with hip OA (median time 84 days; Figure 1). In all OA diagnosis groups, only a few persons returned to work after being 4 months on SA.

Time to sustained return to work after prolonged sickness absence due to osteoarthritis (OA) by type of OA. CMC: carpometacarpal.
The mean followup time was 8.01 years (95% CI 7.98–8.03) and maximum 8.8 years. On average, there were 5.9 transitions (95% CI 5.8–6.0) between different work participation statuses per person. Ten percent had only 1 transition and 12.5% had at least 11 transitions. The first transition was typically from SA to work. In case there were 2 transitions, the most common pathway was from SA to work, followed by a transition to full disability retirement or old age retirement.
The annual proportion of time spent in different statuses (mean time for all persons for each year) did not vary much between groups with knee, hip, or other OA; however, time spent at work was lowest during the first year of followup for persons with polyarthritis or CMC joint OA (Figure 2A–2D). Further, in the latter group only about 20% of time was spent at work during the last year of followup, and the proportion of permanent disability retirement was higher than in any other group. Although most participants typically were at work during the first year of the followup, a considerable proportion was permanently retired, especially in the polyarthritis or CMC joint OA group. During the followup, little time was spent on SA due to OA or on time-restricted work disability, including vocational rehabilitation. Among persons who did not retire, a considerable proportion of time (almost 10%) was spent being economically inactive.

Time spent (mean time for all persons for each year) during followup in different work participation statuses after the end of prolonged sickness absence due to (A) knee OA, (B) hip OA, (C) polyarthritis or CMC joint OA, and (D) other OA. Time-restricted full work disability includes full sickness benefit due to other reason than OA, temporary disability retirement, and vocational rehabilitation. OA: osteoarthritis; CMC: carpometacarpal; SA: sickness absence; pWD: partial work disability; TrFWD: time-restricted full work disability; UE: unemployed; Econ inactive: economically inactive; fDR: permanent full disability retirement; Old age ret: old age retirement.
A total of 412 persons received vocational rehabilitation during the followup. For those with a relatively short SA (up to 60 compensated, equaling 70 calendar days), the rehabilitation started after the first followup year. However, for those with a longer SA (> 90 compensated, equaling 105 calendar days), the rehabilitation typically started within the first months of followup and lasted < 3 months. A large proportion of this latter group transitioned to permanent disability retirement already at the early stages of followup (Supplementary Figure 1, available with the online version of this article).
Persons with OA lost, in total, on average 2.1 (95% CI 2.0–2.2) potential working life–years. However, persons with polyarthritis or CMC joint OA lost significantly more working life–years (2.5, 95% CI 2.3–2.5) than persons with knee or hip OA (2.0, 95% CI 1.9–2.1 and 2.0, 95% CI 1.8–2.1, respectively).
These factors predicted early exit from paid employment during the followup: male sex, older age, low education, long initial SA, and having not returned to work sustainably after the initial SA, as well as receiving vocational rehabilitation (Table 2). In the univariable model, all physical work-related factors increased the risk of early exit; however, the associations lost their statistical significance in the multivariable model.
Determinants of early (before 63 yrs) exit from paid employment.
Figure 3 presents calculations for working life–years expected to be spent in different work participation statuses. For example, a 30-year-old person with a prolonged SA due to OA is expected to spend only 13 years at work and to lose almost 11 working life–years because of full disability or early old age retirement, more than 3 years due to being unemployed or economically inactive, and more than 1 year due to being on ill health–related benefits. On the other hand, a 50-year-old person is expected to work about 5 years and lose another 5 years predominantly as a result of disability or early old age retirement. Overall, 45–53% of potential working life–years were estimated to be spent at work, being highest for those aged 55 years.
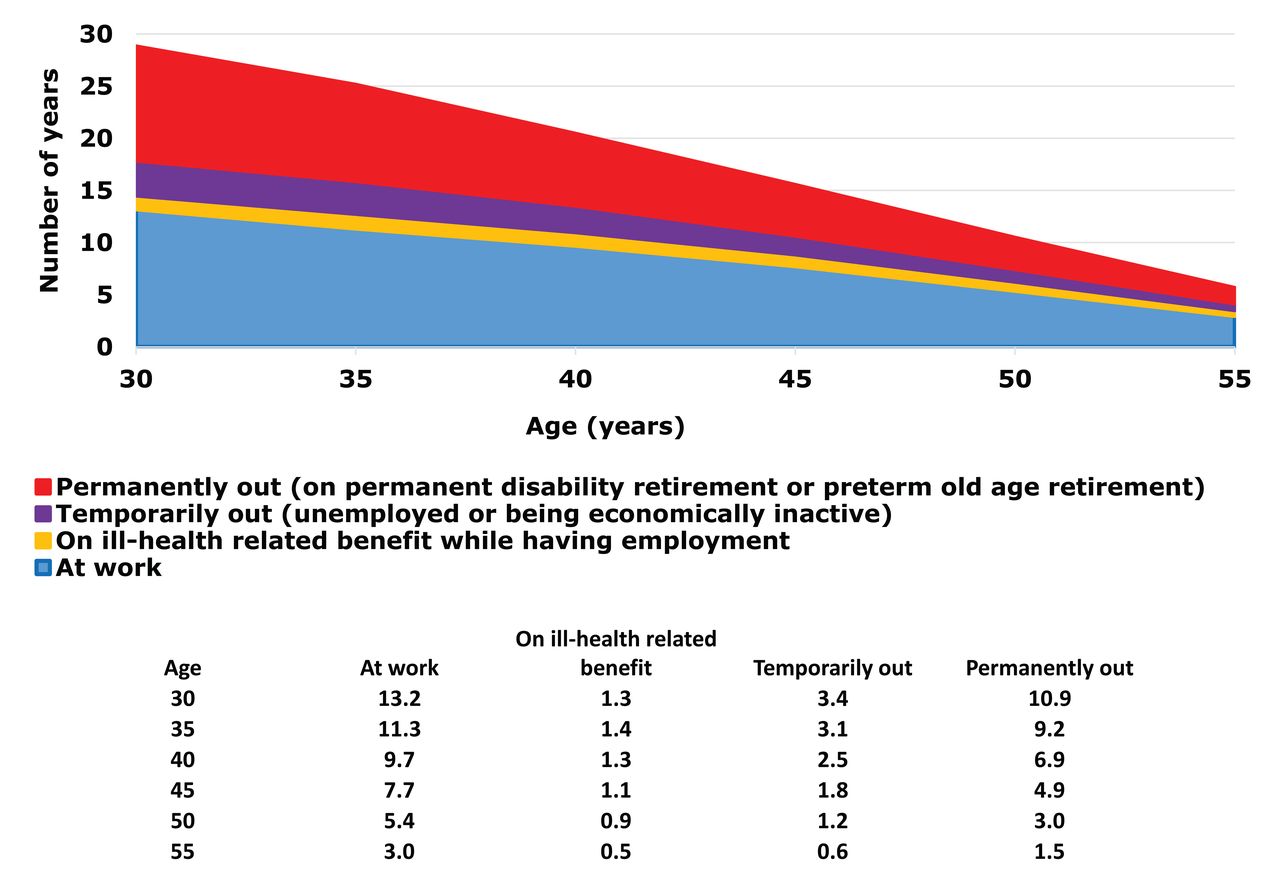
Years expected to be spent in different work participation statuses.
DISCUSSION
We found that persons with disabling OA leading to a prolonged SA have a substantially reduced work participation in the long term, despite their initial return to work within a few months. According to our estimation, they will lose about half of their expected working life–years. Predictors of early exit from work included male sex, older age, lower education, long initial SA, and not having returned to work sustainably after the initial SA, as well as receiving vocational rehabilitation.
This study has several strengths. We used nationally representative registry data with complete information on work participation and ill health–based benefits, including vocational rehabilitation. Moreover, the data allowed identification of transitions between the different work participation statuses for each participant during the entire followup period. Further, because of the large sample size, we could analyze the most common types of OA separately. The selected age range of 30–59 years with a 9-year followup allowed tracking of the population until the end of potential working age. Our results regarding persons with disabling OA can be generalized to societies with a relatively generous social security system.
The limitations of our study include some of the typical features of register-based studies: information on the time of onset or the severity of the condition, surgical treatment such as arthroplasty, and medical rehabilitation was unavailable. Moreover, our cases represent a fraction of persons with clinically diagnosed OA in Finland24 or elsewhere25. We also lacked lifestyle factors and comorbidities among our covariates.
Previous studies have looked at return to work after total knee and hip arthroplasty26, employment rate among persons with knee and hip OA4, as well as occupation-specific SA and disability retirement rates9,10,12. To our knowledge, this is the first study with a long followup, using a wealth of registry information to quantify the burden of OA on work participation among persons with incipient work disability due to OA. Our outcomes included time to sustained return to regular duties after SA, time spent in different work participation statuses on average during 8 years, and potential working life–years lost because of permanent exit from paid employment, as well as years expected to be spent in different work participation statuses until statutory retirement age.
Because of large differences in the outcomes of previous studies and the current study, the results are not directly comparable. Nevertheless, our results, indicating a considerable effect of OA on work participation, are in agreement with the review by Palmer of the effect of knee OA on work participation5. Moreover, our results are in line with an earlier Finnish study reporting a lower employment rate for persons with hip OA as compared with those without OA in the general population6.
The gold standard to treat severe forms of knee and hip OA in particular is arthroplasty27,28. However, surgical treatment involves risks, the lifespan of prostheses is still rather limited, and functional outcomes can be poor. Further, orthopedic surgeons often refrain from operating on young persons or persons with other relative contraindications. So persons with physically heavy work tasks or tasks overloading the affected joint may not be able to return to their earlier work duties and may need retraining to lighter duties29. Vocational rehabilitation, particularly when it involves retraining, has been considered an effective means to prevent early exit from work30. However, our study suggests that vocational rehabilitation was not effective in preventing early exit from paid employment. One reason might be that the vocational rehabilitation was started at a late stage and its short duration suggested that it did not involve retraining.
Clinicians should pay more attention to OA patients with a lower education or those with physically heavy work. Prescription of SA or temporary work disability without a clear treatment or return-to-work plan should be avoided. Indeed, a previous study reported that the durations of past SA predict future absence episodes31. Reducing exposures to affected joints, other work modifications, and retraining to lighter duties could enhance work participation.
Our results show that persons with disabling OA, leading to a longer SA spell, are expected to lose about half of their potential working life–years. For a clinician, a clear message is that prescription of SA or temporary work disability without a clear treatment or return-to-work plan should be avoided. More research is needed on the effectiveness of surgical and conservative treatments of OA on work ability and work participation.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
This study was funded by NordForsk (grant number 76659, SS), the Finnish Work Environment Fund (grant number 115105, SS), and by the Academy of Finland (grant number 303534, EV-J).
- Accepted for publication April 9, 2019.








{kind=link}
{kind=link}
{kind=link}